Supplemental Content - Annals of Internal Medicine

© 2015 American College of Physicians
The information contained herein should never be used as a substitute for clinical judgment.
BEYOND THE GUIDELINES:
Screening Pelvic Examination in Adult Women
Medicine Grand Rounds
March 12, 2015
Discussants
Jennifer Potter, MD
BIDMC Series Editor
Risa Burns, MD,
MPH
Hope Ricciotti, MD
Moderator
Eileen Reynolds
MD
The Series Editors have no conflicts of interest to disclose.
CONFLICT OF INTEREST DISCLOSURE:
The speakers have no financial relationships with a commercial entity producing healthcare-related products and/or services.
Risa Burns, MD, MPH
Eileen Reynolds, MD
Jennifer Potter, MD
Hope Ricciotti, MD
OUR PATIENT
Medical History
• Ms C is a healthy 41 year old woman who recently visited her primary care physician for a periodic health exam.
• She has had mammograms performed annually and Pap tests every 3 years.
OUR PATIENT
Past Medical and Surgical History
• Past medical history
• Gastroesophageal reflux
• Migraine headaches
• Scoliosis
• Past surgical history
• Multiple knee surgeries
OUR PATIENT
Social and Family History
• Social History
• Lives with her son
• Works as an administrator
• Exercises regularly
• No tobacco use
• Rare alcohol use
• Family History
• No history of breast, cervical, ovarian or colon cancer
OUR PATIENT
Medications
• Norethindrone 0.35mg once daily
• Calcium and Vitamin D supplement daily
• Ibuprofen 800mg as needed for pain
• Acetaminophen as needed for pain
OUR PATIENT
Periodic Health Examination
• Well appearing
• BP 124/81
• BMI 25.2
• Normal external and vaginal exam
• Pap test and HPV co-testing performed
• Bimanual examination was not performed
BACKGROUND
• Pelvic examinations have historically been a part of regular preventive care with 62.8 million performed in the US in 2010.
• Historically the examination was conducted in conjunction with annual cervical cancer screening.
• As cervical cancer screening can now be performed at intervals up to every 5 years, depending on the patient, there are questions about whether women need to be seen annually for a routine pelvic examination.
• Many women and providers continue to believe that routine pelvic examination should be a part of the well woman visit.
• And yet, performing routine pelvic examinations adds direct and indirect costs to the health care system as well as opportunity costs.
THE PELVIC EXAMINATION - 3 parts
• Visual inspection of the external genitalia.
• Speculum examination which allows for both a visual inspection of the vagina and cervix and specimen collection for cervical cancer screening.
• Bimanual examination to palpate the uterus, ovaries and adjacent structures.
THE GUIDELINES:
Screening Pelvic Examination in Adult Women
• The American College of Physicians, in July 2014, issued a
Guideline presenting the available evidence on screening for pathology using pelvic examination in adult, asymptomatic, average-risk non-pregnant women.
• The American College of Obstetrics and Gynecology
Committee on Gynecologic Practice had previously issued a
Committee Opinion in August 2012 on the need for annual assessments and provided Guidelines on important elements of the annual examination.
• The American College of Obstetrics and Gynecology reaffirmed its position in a press release following publication of the ACP Guideline.
THE ACP GUIDELINE:
Screening Pelvic Examinations in Asymptomatic, Average-Risk Adult Women:
THE ACP GUIDELINE:
Screening Pelvic Examination in Adult Women
The American College of Physicians Guideline is based on a background article written by Bloomfield and a systematic evidence review sponsored by the
Minneapolis Department of Veterans Affairs Health
Care System’s Evidence-based Synthesis Program
Center.
THE ACP GUIDELINE:
Key Questions
• Evidence review was conducted to address 3 key questions:
• How accurate is the screening pelvic examination for detection of cancer (other than cervical), pelvic inflammatory disease, or other benign gynecologic conditions?
• What are the benefits (reduced mortality and morbidity rates) and harms (over-diagnosis, over-treatment or diagnostic procedure related) of the routine screening pelvic examination?
• What are the examination-related harms and indirect benefits of performing screening pelvic examinations in asymptomatic women? And, do these harms vary by patient characteristics?
THE ACP GUIDELINE:
Summary of Evidence Review- Benefits of Screening
• The diagnostic accuracy of the screening pelvic examination for detecting ovarian cancer or bacterial vaginosis is low.
• The screening pelvic examination rarely detects noncervical cancer or other treatable conditions and was not associated with improved health outcomes.
• There were no studies identified that addressed the diagnostic accuracy of the pelvic examination for other gynecologic conditions such as asymptomatic pelvic inflammatory disease, benign conditions or gynecologic cancers other than cervical and ovarian.
THE ACP GUIDELINE:
Summary of Evidence Review - Harms of Screening
• Many false positive findings are associated with pelvic examination, with attendant psychological and physical harms, including unnecessary laparoscopies or laparotomies.
• Other harms of the pelvic examination include fear, anxiety, embarrassment, pain and discomfort.
• Women with a history of sexual violence, especially those with PTSD, may experience more pain, discomfort, fear, anxiety or embarrassment.
THE ACP GUIDELINE:
ACP Recommendations
• Based on the evidence review the ACP recommends against performing routine screening pelvic examination in asymptomatic, non-pregnant, adult women. (strong recommendation, moderate quality evidence)
• The current evidence suggests that the harms of performing routine screening pelvic examination outweigh any demonstrated benefit .
• Indirect evidence shows that routine screening pelvic examination does not reduce morbidity or mortality in asymptomatic adult women.
THE ACP GUIDELINE:
ACP Recommendations
• As pelvic examination is low-value care it should be omitted from the well-woman visit.
• Cervical cancer screening should be limited to visual inspection of the cervix and cervical swabs for cancer and human papillomavirus.
• Screening for chlamydia and gonorrhea should be done with self-collected vaginal swabs.
• Pelvic examination should not be required before prescribing hormonal contraception.
THE ACOG Opinion:
The Well-Woman Visit
ACOG Committee Opinion
Well-Woman Visit
August 2012
• Well-woman visit. Committee Opinion No. 534. American College of Obstetricians and
Gynecologists. Obstet Gynecol 2012;120:421–4.
ACOG OPINION:
Well-Woman Annual Visit
• Annual visit fundamental part of medical care and provides:
• An opportunity to promote prevention practices
• An opportunity to recognize risk factors for disease
• An opportunity to identify medical conditions
• An opportunity to establish the clinician-patient relationship
• Annual visit should include:
• Screening, evaluation, counseling and immunizations based on risk factors and age
• Performance of a physical examination is a key part of an annual visit though the components may vary depending on patient age, risk factors, and physician preferences
ACOG OPINION:
Well-Woman Annual Visit - Pelvic Examination
• The ACOG opinion is that a pelvic examination should be performed on an annual basis in all patients aged
21 years and older.
• Acknowledge, no evidence supports or refutes the annual pelvic examination for the asymptomatic, lowrisk patient.
• An annual pelvic examination seems logical but also lacks data to support a specific time frame or frequency of such examinations.
ACOG OPINION:
Well-Woman Annual Visit - Shared Decision Making
• The decision whether or not to perform a routine pelvic examination at the time of the periodic health examination for the asymptomatic patient should be a shared discussion between the patient and her health care provider.
• The decision to receive an exam can be left to the patient if she is asymptomatic and has undergone a TAH-BSO for benign indications, has no history of vulvar or cervical neoplasia, is
HIV negative, is not immunocompromised and was not exposed to DES.
• It is reasonable to stop performing pelvic examinations when a woman’s age or other health issues reach a point where the woman would choose not to intervene on conditions detected during the examination.
QUESTIONS
For Dr. Potter and Ricciotti
To help us decide how to apply these divergent recommendations in Ms C’s case we asked our discussants the following questions:
1. Would you recommend a pelvic examination for this patient on an annual basis and if so, why or why not?
2. What do you think the impact will be on the care of this patient and other patients if physicians stop routinely performing routine pelvic examinations?
3. What do you think are the pros and cons of performing a routine pelvic examination on this patient?
OUR MODERATOR & DISCUSSANTS
• Eileen Reynolds, MD (Moderator)
Associate Professor of Medicine, HMS
Vice Chair for Education in the Department of Medicine at BIDMC
General Medicine and Primary Care, BIDMC
• Jennifer Potter, MD
Associate Professor of Medicine, HMS
Director of Women’s Health Program at BIDMC and Fenway Health
• Hope Ricciotti, MD
Associate Professor of Medicine, HMS
Chair and Residency Program Director in the Department of
Obstetrics and Gynecology at BIDMC
Dr. Potter
Primary Care Viewpoint
Routine Pelvic Examination:
An Evidence-Based Appraisal
CHOOSING WISELY:
Questions to Ask and Discuss with Patients
• What benefits do we hope to achieve?
• Is there evidence that these benefits are attainable?
• Is there evidence for harm?
• Is the service a rational way to utilize available resources?
• Or should other services be considered that are of definitive value?
BURDEN OF PROOF
• To meet effectiveness criteria for a screening test, conclusive evidence must show that bimanual examination (BME):
• Accurately detects disease at an early stage
• Is acceptable to patients
• Is cost effective
• Reduces morbidity and mortality in a large-scale, randomized, controlled trial.
DIAGNO ST IC ACCURACY O F BME: D ETEC T IO N
O F UPPER GENITAL T RAC T ABNO RMALITIES
Experienced gynecologists (n=52) examining anesthetized patients (n=84; average age 37.7 years) with known upper genital tract abnormalities undergoing surgery
Outcome Sensitivity Specificity
Positive Predictive
Value (PPV)*
Adnexal Mass ≥ 5 cm
Abnormal Uterine Size
0.28 (0.13, 0.46) 0.93 (0.83, 0.96) 0.64 (0.35, 0.74)
0.64 (0.45, 0.83) 0.80 (0.67, 0.87) 0.57 (0.37, 0.72)
Abnormal Uterine Contour 0.62 (0.43, 0.80) 0.78 (0.64, 0.85) 0.55 (0.37, 0.66)
*PPV = True positives/All positives
• Padilla LA, Radosevich DM, Milad MP. Limitations of the pelvic examination for evaluation of the female pelvic organs. Int J Gynaecol Obstet. 2005;88:84-88.
DIAGNOSTIC ACCURACY OF SCREENING
BME FOR DETECTION OF OVARIAN CANCER
Prospective
Cohort Study*
(Year)
Study
Population
Abnormal or
Ambiguous
BME
28 (2.7%)
1 Year Incidence of Ovarian Cancer
1/1010 (0.1%)
Positive
Predictive Value
(PPV) of
Abnormal BME
3.6% (1/28) Jacobs et al.
(1988)
Grover et al.
(1995)
Adonakis et al.
(1996)
N=1010
Mean age 54
N=2623
Mean age 51
N=2000
Mean age 58
40 (1.5%)
174 (8.7%)
1/2623 (0.04%)**
2/2000 (0.1%)
0% (0/40)
1.2% (2/174)
*None designed/powered to detect morbidity/mortality benefits.
**Single case occurred in a woman with a normal exam.
• Jacobs I, Stabile I, Bridges J, Kemsley P, Reynolds C, Grudzinskas J, et al. Multimodal approach to screening for ovarian cancer. Lancet.
1988;1:268-71.
• Grover SR, Quinn MA. Is there any value in bimanual pelvic examination as a screening test. Med J Aust. 1995;162:408-410.
• Adonakis GL, Paraskevaidis E, Tsiga S, Seferiadis K, Lolis DE. A combined approach for the early detection of ovarian cancer in asymptomatic women. Eur J Obstet Gynecol Reprod Biol.
1996;65:221-5.
DIAGNOSTIC ACCURACY OF BME FOR
DETECTION OF ENDOMETRIAL CANCER
• No specific studies.
• Given the biology of endometrial CA, would not expect
BME to detect disease until late in the course.
• High proportion of patients present with symptoms
(abnormal bleeding).
• Patient education, rather than pelvic exam, a key early detection strategy .
• Trimble CL, Method M, Leitao M, Lu K, Ioffe O, Hampton M, et al. Management of endometrial precancers. Obstet Gynecol.
2012;120:1160-75.
• Modesitt S. Missed opportunities for primary endometrial cancer prevention: how to optimize early identification and treatment of high-risk women. Obstet Gynecol. 2012;120:989-
91.
DIAGNOSTIC ACCURACY FOR DETECTION
OF UPPER GENITAL TRACT INFECTIONS
• Retrospective cohort study (n=2169) of asymptomatic women presenting to an STI clinic:
• 26/2169 (1.2%) had upper genital tract findings; infection was confirmed in only 7/26.
• CDC recommends presumptive treatment for PID only if patients have both signs and symptoms .
• Patient-collected vaginal swabs are the specimens of choice when screening at-risk women for STIs.
• Singh RH, Erbelding EJ, Zenilman JM, Ghanem KG. The role of speculum and bimanual examinations when evaluating attendees at a sexually transmitted diseases clinic. Sex
Transm Infect. 2007;83:206-10.
• Chernesky MA, Hook EW 3rd, Martin DH, Lane J, Johnson R, Jordan JA, et al. Women find it easy and prefer to collect their own vaginal swabs to diagnose Chlamydia trachomatis or Neisseria gonorrhoeae infections. Sex Transm Dis. 2005;32:729-33.
• Schachter J, Chernesky MA, Willis DE, Fine PM, Martin DH, Fuller D, et al. Vaginal swabs are the specimens of choice when screening for Chlamydia trachomatis and Neisseria gonorrhoeae: results from a multicenter evaluation of the APTIMA assays for both infections. Sex Transm Dis.
2005;32:725-8.
• Workowski KA, Berman S, Centers for Disease Control and Prevention (CDC). Sexually transmitted diseases treatment guidelines, 2010. MMWR Recomm Rep. 2010;59:1-110.
DIAGNOSTIC ACCURACY IN DETECTING
PELVIC FLOOR DYSFUNCTION
• No studies on the role of vaginal palpation in screening asymptomatic women.
• Literature has focused on identification and treatment of symptomatic women.
• Emerging data suggest that preemptive pelvic floor muscle training (PFMT) at strategic points across the reproductive continuum may have preventive value .
• Boyle R, Hay-Smith EJ, Cody JD, Mørkved S. Pelvic floor muscle training for prevention and treatment of urinary and faecal incontinence in antenatal and postnatal women. Cochrane Database Syst Rev.
2012;10:CD007471.
IMPACT OF BME ON QOL & MORTALITY
• No RCTs have evaluated the impact of either BME or combined speculum/BME on morbidity or mortality from any gynecological condition.
• BME was dropped from the screening protocol of the Prostate
Lung Colorectal Ovarian (PLCO) trial (n=78,216) after 5 years because no ovarian cancer cases were detected solely by adnexal palpation .
• PLCO results: no significant differences in number of ovarian cancer cases detected by CA-125/TVUS (212 vs. 176 cases; RR
1.21 [95% CI, 0.99-1.48]), stage of disease, or ovarian cancer mortality (118 vs. 100 deaths; RR 1.18 [95% CI, 0.82-1.71]).
• Buys SS, Patridge E, Black A, Johnson CC, Lamerato L, Isaacs C, et al. Effect of screening on ovarian cancer mortality: the Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Randomized Controlled
Trial. JAMA. 2011;305:2295-303.
PELVIC EXAM IS ASSOCIATED WITH
PSYCHOLOGICAL / PHYSICAL DISTRESS
• Data from 14 low quality survey studies and 1 cohort study (median n=409; range 40-7168).
• Fear, embarrassment, or anxiety endorsed by 10-
80% (median = 34%).
• Pain or discomfort endorsed by 11-60% (median =
35%).
• No studies have examined the degree of distress attributable to different pelvic exam components.
• Bloomfield HE, Olson A, Greer N, Cantor A, MacDonald R, Rutkus I, et al. Screening pelvic examinations in asymptomatic, average-risk adult women: an evidence report for a clinical practice guideline from the
American College of Physicians. Ann Intern Med. 2014;161:46-53.
PATIENT-CENTERED CARE PARAMOUNT
• Low patient acceptability reduces adherence:
• Women reporting pelvic exam-related pain or discomfort less likely to follow-up (5/5 studies).
• High patient acceptability increases adherence:
• Increased utilization of hormonal contraceptives when receipt is uncoupled from pelvic exam.
• Patient preference for (and better performance of) self-collected vaginal swabs for STI screening.
• Bloomfield HE, Olson A, Greer N, Cantor A, MacDonald R, Rutkus I, et al. Screening pelvic examinations in asymptomatic, average-risk adult women: an evidence report for a clinical practice guideline from the
American College of Physicians. Ann Intern Med. 2014;161:46-53
• Harper C, Balistreri E, Boggess J, Leon K, Darney P. Provision of hormonal contraceptives without a mandatory pelvic examination: the first stop demonstration project. Fam Plann Perspect. 2001;33:13-8.
• Chernesky MA, Hook EW 3rd, Martin DH, Lane J, Johnson R, Jordan JA, et al. Women find it easy and prefer to collect their own vaginal swabs to diagnose Chlamydia trachomatis or Neisseria gonorrhoeae infections. Sex Transm Dis. 2005;32:729-33.
• Schachter J, Chernesky MA, Willis DE, Fine PM, Martin DH, Fuller D, et al. Vaginal swabs are the specimens of choice when screening for Chlamydia trachomatis and Neisseria gonorrhoeae: results from a multicenter evaluation of the APTIMA assays for both infections. Sex Transm Dis. 2005;32:725-8.
DIAGNO ST IC PRO CEDURES A FTER SCREENING -
RELAT ED F INDINGS MAY ALS O INCUR HARM
• False reassurance patient ignores or delays evaluation for new symptoms.
• Overdetection (diagnosis of a clinically irrelevant abnormality).
• Overtreatment (treatment for a clinically irrelevant abnormality that would never have adversely affected
QOL or survival).
• Diagnostic procedure-related complications .
• No studies have directly assessed any of these potential harms .
• Bloomfield HE, Olson A, Greer N, Cantor A, MacDonald R, Rutkus I, et al. Screening pelvic examinations in asymptomatic, average-risk adult women: an evidence report for a clinical practice guideline from the American College of Physicians. Ann Intern Med.
2014;161:46-53.
FALSE PO S ITIVE BME FIND INGS LEA D TO
UNNECES SARY SURGERIES ( I N D I R E C T E V I D E N C E )
In 1 prospective cohort study, 174/2000 (8.7%) asymptomatic, average-risk women aged 45-80 had abnormal adnexal findings on BME and a normal serum CA-125
31/174 (18%) underwent surgery
2/31 (6.5%) were found to have ovarian cancer
Performance of screening BME led to unnecessary surgery in 1.5%
(29/2000)
62.8 million screening pelvic exams were performed in the US in 2010 (NAMCS and NHAMCS data); therefore, the number of false positive tests occurring nationwide is likely substantial .
• Adonakis GL, Paraskevaidis E, Tsiga S, Seferiadis K, Lolis DE. A combined approach for the early detection of ovarian cancer in asymptomatic women. Eur J Obstet Gynecol Reprod Biol. 1996;65:221-25. http://www.cdc.gov/nchs/data/ahcd/namcs_summary/2010_namcs_web_tables.pdf
UNNECES SARY SURGERIES CA N CAUSE
SERIOUS CO MPLICAT IO NS ( I N D I R E C T E V I D E N C E )
In the PLCO trial, 1080/3285 women
(33%) with false positive screening tests (serum CA-125 and TVUS) for ovarian cancer underwent surgery
15% (163/1080) experienced at least one serious complication
• Buys SS, Patridge E, Black A, Johnson CC, Lamerato L, Isaacs C, et al. Effect of screening on ovarian cancer mortality: the Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer
Screening Randomized Controlled Trial. JAMA. 2011;305:2295-303.
REDUCING UNNECESSARY PELVIC EXAMS
WOULD RESULT IN SIGNIFICANT SAVINGS
• Annual cost of preventive GYN exams was $2.6 billion in 2002-2004 (NAMCS & NHAMCS data).
• Average per-visit laboratory and radiology costs were $136.
• Current costs likely substantial due to inflation and performance of pelvic exams more often than recommended by current cervical cancer screening guidelines.
• Mehrotra A, Zaslavsky AM, Ayanian JZ. Preventive health examinations and preventive gynecological examinations in the United States. Arch Intern Med. 2007;167:1876-83.
CURRENT PRACTICE: NOT EVIDENCE -BASED
• Paps still being done on women < 21 years of age and after
hysterectomy for benign disease.
• 2010 survey of US physicians and APRNs (n=1196; response rate 65%): 1/3 still required pelvic exam prior to provision of
OCs.
• 2009 survey of US physicians (n=2825; response rate 44%):
30-95% routinely performed pelvic exams to screen for ovarian cancer , 41-96% to screen for other GYN cancers, and
40-92% to screen for STIs.
• Morioka-Douglas N, Hillard PJ. No Papanicolaou tests in women younger than
21 years or after hysterectomy for benign disease. JAMA Intern Med.
2013;173:855-6.
• Henderson JT, Harper CC, Gutin S, Saraiya M, Chapman J, Sawaya GF. Routine bimanual pelvic examinations: practices and beliefs of US obstetrciangynecologists. Am J Obstet Gynecol. 2013;208:109.e1-7.
• Stormo AR, Hawkins NA, Cooper CP, Saraiya M. The pelvic examination as a screening tool: practices of US physicians. Arch
Intern Med. 2011;171:2053-4.
EVIDENCE-BASED PREVENTIVE HEALTH
INTERVENTIONS ARE UNDERUTILIZED
• In 2012, HPV vaccine uptake among US females aged 19-26 (≥ 1 dose, ever) was 34.5%.
• In 2001, 7% of women aged ≥ 18 in a nationally representative sample (n=4821) reported ever being asked about domestic
violence.
• Between 1999-2010, chlamydia screening coverage among eligible US females ranged from 40-60%.
• In 2009, the proportion of contraceptors using long-acting reversible contraception (LARC) was 8.5%.
• Williams WW, Lu PJ, O'Halloran A, Bridges CB, Pilishvili T, Hales CM, et al.
Noninfluenza vaccination coverage amoung adults - United States, 2012. MMWR
Morb Mortal Wkly Rep. 2014;63:95-102.
• Klap R, Tang L, Wells K, Starks SL, Rodriguez M. Screening for domestic violence amoung adult women in the United States. J Gen Intern Med. 2007;22:579-84.
• Hoover KW, Leichliter JS, Torrone EA, Loosier PS, Gift TL, Tao G, et al.
Chlamydia screening amoung females aged 15-21 years--multiple data sources, United States, 1999-2010. MMSW Surveill Summ. 2014;63:80-8.
• Finer LB, Jerman J, Kavanaugh ML. Changes in use of long-acting contrceptive methods in the United States, 2007-2009. Fertil Steril. 2012;98:893-7.
‘ASYMPTOMATIC ’ AND ‘AVERAGE -RISK’ ARE
OPERATIVE WORDS, BUT…
• Only 40% of US OB GYNs routinely ask about sexual function
(2012 survey, n=1154, response rate 66%).
• Only 38% of women with urinary incontinence asked about symptoms (2006 study, n=321 patients presenting to a UK general GYN clinic).
• Patient-reported family histories of ovarian and uterine cancer
are often unreliable:
• Negative likelihood ratios 0.51 [95% C, 0.13-2.10] and 0.68 [95% CI, 0.31-
1.52], respectively.
• Dyer K, das Nair R. Why don't healthcare professionals talk about sex? A systematic review of recent qualitative studies conducted in the United
Kingdom. J Sex Med. 2013;10:2658-70.
• Griffiths AN, Makam A, Edwards GJ. Should we actively screen for urinary and anal incontinence in the general gynaecology outpatients setting? - A prospective observational study. J Obstet Gynaecol. 2006;26:442-4.
• Murff HJ, Spigel DR, Syngal S. Does this patient have a family history of cancer? An evidence-based analysis of the accuracy of family cancer history. JAMA. 2004;292:1480-9.
WHAT WILL HAPPEN IF WE STOP ROUTINELY
PERFORMING PELVIC EXAMS?
• Improve care by refocusing efforts on:
• Communicating more effectively with patients.
• Optimizing delivery of evidence-based preventive
health interventions.
• Redirect resources toward:
• Developing novel research, policy, and educational strategies to enhance female sexual and reproductive health outcomes.
WHAT TO SAY TO OUR PATIENT
Choosing Wisely Questions, Revisited
• What benefits do we hope to achieve?
• Is there evidence that these benefits are attainable?
• Is there evidence for harm?
• Is the service a rational way to utilize available resources?
Screening BME should not be done as it has no
demonstrable benefits and may cause harm.
Services with proven benefits should be offered.
WHAT TO SAY TO OUR PATIENT
• For a woman of Ms C’s age, comorbidities, and stated risks, the periodic health visit provides an appropriate context to :
Elicit symptoms (incl. taking a thorough sexual and urological history) and respond to concerns ;
Identify risk factors (incl. updating her family history);
Screen for domestic violence ;
Screen for STIs (if at-risk; patient-collected vaginal swab);
Discuss ‘alarm’ symptoms (e.g., abnormal bleeding);
Provide counseling re: highly effective contraception , healthy lifestyle behaviors ; and
Offer same-day access to LARC insertion (if desired).
Dr. Ricciotti
Gynecology Viewpoint
HOPE RICCIOTTI’S VIEWPOINT
I recommend annual pelvic examination
(speculum and bimanual examination) for women over 21 years (as recommended by the American College of Obstetricians and
Gynecologists)
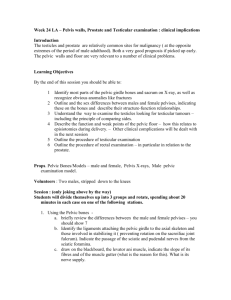
ACOG RECOMMENDATIONS
Population
Women younger than
21 years
Women aged 21-29
Women aged 30-65
Annual Pelvic Examination
Only when indicated by medical history
Yes
Yes
Cervical Cancer Screening
No screening
Cytology alone every 3 years
Human papillomavirus and cytology
Co-testing (preferred) every 5 years
Cytology alone
(acceptable) every 3 years
Women over 65
Women who underwent total hysterectomy
Yes
Decision to receive an internal examination can be left to the patient if she is asymptomatic
No screening necessary after adequate negative prior screening results
No screening necessary in low-risk women
CERVICAL CANCER SCREENING IS NOT
PART OF DEBATE
• Pap testing very effective in prevention and early detection of cervical cancer
• Intervals have been lengthened to every three to five years
• May prompt women to question coming in to see health provider in years test not indicated
PELVIC EXAMINATION IS
NOT NECESSARY
• To screen for sexually transmitted infections
(STIs) - Urine or vaginal swab samples can be tested using nucleic acid amplification, and do not require a pelvic examination
• Before initiating contraception in healthy, asymptomatic individuals; does not help identify contraindications to hormonal contraception
OVARIAN CANCER AND
PELVIC EXAMINATION
• Consensus - no evidence for effectiveness of pelvic examination in early detection of ovarian cancer
• No effective test for early detection of ovarian cancer in asymptomatic low-risk women – not pelvic examination, ultrasound, or Ca125 blood testing
PELVIC EXAMINATION FOR BENIGN
CONDITIONS OR CANCERS OTHER THAN
CERVIX OR OVARY
• No studies done
• All women in studies on ovarian cancer were older than 45 or postmenopausal
• Deciding when sufficient quality evidence to make a broadly applied practice recommendation is a complex task
MORE STUDY NEEDED TO ANSWER:
• Does pelvic examination have effect on benign conditions?
• Does pelvic examination improve quality of life among women of all ages, especially reproductive aged women?
PROS OF PELVIC EXAMINATION
• Enhances informed decision-making, provider judgment (difficult outcomes to measure)
• Prolapse, vaginal discharge, atrophic changes, and fixed organs might prompt health care provider to ask additional pointed questions
• Basing decision to do pelvic examination on report of abnormal symptoms or risk factors may not be universally effective
CONS OF PELVIC EXAMINATION
• Potential harms of over-diagnosis and overtreatment, increased health care costs
• Patient fear, anxiety, embarrassment and pain
• May prompt patients to avoid care
IMPLICATIONS OF NOT DOING
ROUTINE PELVIC EXAMINATIONS
• Women may stop coming for preventive reproductive care health care
• Could limit health insurance coverage for well women examinations
• Provider skill decline, especially in obese or challenging patients
• Resident training decline
WHY MORE SCRUTINY OF PELVIC
EXAMINATION THAN OTHER PARTS
OF PHYSICAL EXAMINATION?
• Is pelvic examination being held to higher standard?
• Consider prostate screening “shared decision making” model
• Pelvic examination should not be stigmatized
PATIENT-CENTERED APPROACH
• Allow the patient to be final arbiter of what tradeoffs they are willing to make to decrease their risk of developing a condition
• Gone are days when physicians are final arbiter of what tradeoffs patients are willing to make to decrease their risk of developing a condition
EDITOR’S SUMMARY
Ms C’s request
“ I want to see proof. I respect the professionals, so if you are able to provide proof over whatever studies have been done, then I think I would be more comfortable with it.
”
EDITOR’S SUMMARY
Would you recommend a pelvic examination for Ms C?
• Dr Potter agrees with the ACP Guideline. She would not recommend a pelvic examination based on the currently available scientific evidence.
• Dr Ricciotti concurs with the ACOG Opinion. She would recommend a pelvic examination though she acknowledges that there is no current scientific evidence that supports or refutes an annual pelvic examination for an asymptomatic, average-risk woman.
• They both agree that there are potential harms of performing pelvic examinations including over-diagnosis and over-treatment as well as patient fear, anxiety, embarrassment and pain.
EDITOR’S SUMMARY
Impact of the Recommendation - Dr Potter
• Providers could refocus their efforts on communicating more effectively with patients and increasing receipt of evidence-based care.
• Messaging to patients could be changed to highlight services of proven value that should be offered during a periodic health visit.
• Medical education programs could supplement opportunities to practice examination techniques with actual patients by using simulation and genital teaching associates.
EDITOR’S SUMMARY
Impact of the Recommendation - Dr Ricciotti
• The pelvic examination provides an opportunity to start a conversation about symptoms and this would be lost.
• Women may not come in for care and would miss regular screening.
• Insurance coverage may become limited for routine care.
• Providers are at risk of losing skills and training opportunities.
EDITOR’S SUMMARY
High Value Care Considerations
• Agreement:
• GC and chlamydia screening can be self-collected
• No need for pelvic examination before providing birth control
• Disagreement:
• Need for performing a bimanual examination when doing Pap test
• Need for routine annual pelvic examination
EDITOR’S SUMMARY
Unanswered Questions
• Ms C asked us - Are you able to provide proof?
• Deciding when there is sufficient quality evidence to conclude that a broadly applied practice should be stopped is a difficult task.
• Future Research
• What is the value of pelvic examination in detecting benign conditions?
• Do pelvic examinations improve quality of life for women?
• What is the optimal method and timing for sensitive conversations?
• Do we have enough evidence to stop performing routine pelvic examination or should there be a discussion with shared decision making between a patient and her physician until more evidence is available.
We would like to thank…
Our Patient
Discussants
Hope Ricciotti, MD
Jennifer Potter, MD
Beyond the Guidelines Editors
Risa Burns, MD, MPH Eileen Reynolds, MD
Deborah Cotton, MD, MPH Gerald Smetana, MD
Video Production
Last Minute Productions
We would like to thank…
BIDMC Media Services
Series Coordinator
Lizzie Williamson
© 2015 American College of Physicians
The information contained herein should never be used as a substitute for clinical judgment.