Creating a
Centennial Vision:
Four Possible Scenarios
The American Occupational Therapy
Association
© Association of Computing Machinery. Used with permission.
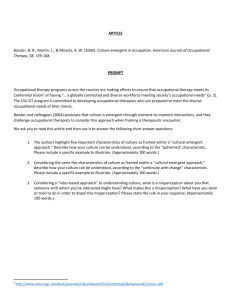
A VISIONARY EXAMPLE
Apple’s Vision of the “Knowledge Navigator” in 1987
Apple’s Vision Fostered the
Development of:
Portable,
wireless flat screen computers
Multiple input devices (voice, touch)
Simultaneous applications
Agents (AI)
Integrated IT (phone, data, network)
Personal data managers (calendar, tasks)
Videoconferencing
Data mining and retrieval
(Sculley, 1989)
When
we imagine future worlds
and create visions,
by acting on those visions
we set in motion
circumstances that enable
our imagination to
become reality.
Mahatma Gandhi
(1869–1948)
“Be the change you want to see in the world.”1
1ThinkExist.com,
2005a.
Imagine a world different
than the one you now inhabit...
© Sonia Coleman. Used with permission.
Shaping the Centennial Vision
What must the
profession of
occupational
therapy do
during the next
twelve years to
best position
itself for the
world of 2017
and beyond?
© Sonia Coleman. Used with permission.
Looking to the Future:
Some Common Mistakes
Making predictions rather than attaching
probabilities to possibilities
Simply extrapolating current trends
Overestimating the influence of shortterm change
Underestimating the influence of longterm change
Thinking of only one future
Planning for Change
Change is constant
In the present age, change is not
incremental, it is exponential
No one can exactly predict the future, but
we can anticipate the course of known
trends
Unexpected or “wildcard” events are key
reasons why known trends are not
foolproof in predicting the future
Examples of Wildcards
The stock market
crash of 1929
The attack on Pearl
Harbor
Shooting of Martin
Luther King, Jr.
The advent of HIVAIDS
The fall of the
Soviet Union
The 9-11 attacks
From Photos To Go Unlimited. Used with permission.
Therapeutic Positioning in the
Strategic Sense
Consider where the profession is now
Anticipate what the public’s needs are
likely to be as the country moves into the
third decade of this century and beyond
Identify the services that must be
provided at that point to meet those
needs
Take steps to prepare the profession to
provide those services
“Skate to where the puck is
going to be.” —Wayne Gretzky1
From Photos To Go Unlimited. Used with permission.
• Identify and
understand
important trends
1ThinkExist.com,
• Take steps
to shape
events
2005b.
The point
is not to
predict the
future,
but to
prepare for
it and to
shape it.
© Health Canada, www.hc-sc.gc.ca. Used with
permission of the Minister of Public Works and
Government Services, Canada, 2005.
Occupational Therapy
Current profile and emerging areas of practice
© Health Canada, www.hc-sc.gc.ca. Used with
permission of the Minister of Public Works and
Government Services, Canada, 2005.
Occupational Therapy
Workforce
Total Practitioners: 112,653
OTAs
19,990
OTs
82,990
(AOTA, 2005)
Workforce Trends
1968–2003
120,000
100,000
80,000
60,000
OTAs
OTs
40,000
20,000
1968
1978
1988
1998
2003
Year
(AOTA, 2005)
Practice Settings
(AOTA, 2005)
Today’s Emerging Areas of
Occupational Therapy Practice
Ergonomics consulting
Design and accessibility consulting and home
modification
Older driver assessment and training
Consulting to assisted-living facilities
Technology and assistive-device development and
consulting
Health and wellness consulting
Low vision rehabilitation
Addressing Alzheimer's disease and caregiver training
Addressing the needs of children and youth
Community services
Important Drivers of Change
Aging and longevity
Universal design
Internet and the Information Age
Prospective and preventive
medicine
Changing world of work
Information access
Drivers of Change (cont.)
Diversity of population
Stress and depression
Developments in assistive
technologies
Changes in lifestyle values and
choices
Health care costs, reimbursement
issues, and the efficacy of care
Change in Population
2000–2020
75%
54%
Total U.S.
Population
Growth:
10% 14%
(9%)
Under
15
15–34
35–44
18%
5%
45–54 55–64
65+
Age (years)
(U.S. Census Bureau, 2002)
UNIVERSAL DESIGN
Equitable use
Flexibility in use
Simple and intuitive
use
Perceptible
information
Tolerance for error
Low physical effort
Size and space for
approach and use
Copyright © 1997 NC State University, The Center for
Universal Design
From Photos To Go Unlimited. Used with permission.
Recognizes that people are different
• Rise of the personal
computer
• The Internet
• Wireless
connectivity
• Personalization
• Privacy/identity
concerns
From Photos To Go Unlimited. Used with permission.
Information Age
Changing World of Work
• Growth in the service sector,
more specific risks
• New forms of work (e.g.,
telework, job sharing, contracting)
• Growing interest in autonomous
work (entrepreneurism)
• Changing management
structures (flatter, smaller, leaner)
• Increasing work pace and
workload
About 25 million (10%) of
current U.S. residents
were not born in the U.S.
The Hispanic population
will increase from 37
million today to 55 million
by 2020 (49% increase).
By 2020, the median age
of Hispanics will be 28.8
versus 37.6 for the total
population.
From Photos To Go Unlimited. Used with permission.
Cultural Diversity in 2020
There is growing
evidence of a clear
connection between
stress and chronic
disease through the
immune system.
The term
“allostasis” refers to
the body’s response
to the stress of life
over time.
From Photos To Go Unlimited. Used with permission.
Stress-Related Disorders
Chronic Stress
“Provides a hormonal milieu conducive to
the development” of
Visceral obesity
Insulin resistance/dyslipidemia syndrome
Hypertension
Atherosclerosis
Osteoporosis
Immune dysfunction
Depression
Irritable colon
Peptic ulcer
Substance abuse
(VanItallie, 2002, pp. 40–45)
Specific Measures:
Allostatic Load
Blood
pressure
Cortisol
excretion
C-reactive
protein
LDL, HDL
Total
cholesterol
Body mass index
Waist-to-hip ratio
Noradrenalin
Epinephrine
DHEA
Why Zebras
Don’t Get Ulcers
Robert M.
Sapolsky
A readable and
useful overview
of the
relationship
among stress,
disease, and
coping
Depression
The inability to cope with the demands of
everyday life can lead to depression.
About 26% of Americans had a mental
health disorder in 2002.
Two thirds (66%) of these cases were
moderate or severe.
Only 52% of the severe cases, 34% of the
moderate cases, and 23% of the mild
cases were treated by professionals.
(Narrow, 1999)
Assistive Technologies
Smart home monitoring
Robotics
Programmed electrical stimulation of
muscles to enable movement
Cochlear implants
Biosensors and biomonitoring
New uses of telemetry
Nanotechnology:
Molecular-scale
machines to deliver
drugs, repair cells, or
produce needed
proteins or enzymes
Use of genetic markers
Regenerative
medicine/stem cell
breakthroughs
Wearable
diagnostics/monitoring/
imaging
From Photos To Go Unlimited. Used with permission.
Technological Advances
Lifestyle Values & Choices
Continued debate on the meaning of family
Greater emphasis on balancing work and
family
Less interest in lifelong careers
Growing acceptance of end-of-life options
Growing recognition of the importance of
social factors influencing health (e.g., ICF)
Greater appreciation for quality-of-life issues
DALYS*
DALYs
(thousands)
All causes
1. Ischaemic heart disease
2. Unipolar major depression
3. Cerebrovascular disease
4. Road traffic accidents
5. Alcohol use
6. Osteoarthritis
7. Trachea, bronchus, and lung cancers
8. Dementia & other degenerative CNS disorders
9. Self-inflicted injuries
10. Congenital abnormalities
Percent
of total
160,944
100.0
15,950
9.9
9,780
6.1
9,425
5.9
7,064
4.4
6,446
4.0
4,681
2.9
4,587
2.9
3,816
2.4
3,768
2.3
3,480
2.3
*Disability Adjusted Life Years (a measure of disease burden)
(Murray & Lopez, 1996)
DALYS*
DALYs
(thousands)
All causes
1. Ischaemic heart disease
2. Unipolar major depression
3. Cerebrovascular disease
4. Road traffic accidents
5. Alcohol use
6. Osteoarthritis
7. Trachea, bronchus, and lung cancers
8. Dementia & other degenerative CNS disorders
9. Self-inflicted injuries
10. Congenital abnormalities
Percent
of total
160,944
100.0
15,950
9.9
9,780
6.1
9,425
5.9
7,064
4.4
6,446
4.0
4,681
2.9
4,587
2.9
3,816
2.4
3,768
2.3
3,480
2.3
*Disability Adjusted Life Years (a measure of disease burden)
(Murray & Lopez, 1996)
Number of Medicare Beneficiaries
The number of people Medicare serves will nearly double by 2030.
76.8*
Medicare Enrollment
(millions)
80
61.0*
8.6
Disabled & ESRD
Elderly
70
60
39.6
50
40
28.4
8.7
34.3
7.3
20.4
5.4
68.2
3.3
30
3.0
52.2
20
10
45.9*
20.4
25.5
31.0
34.1
38.6
1990
2000
2010
0
1970
1980
Calendar Year
* Estimated. Numbers may not sum due to rounding.
Source: CMS, 2004.
2020
2030
Percent of Individuals
Limited in Activities Because of
Chronic Conditions (By Age)
45
40
35
30
25
%
20
15
10
5
0
< 18
18Ğ44
45Ğ64
Age
65Ğ74
75 +
(Robert Wood Johnson
Foundation, 1996)
U.S. Health Care Costs
Medical care at end of life consumes 10%–12% of
total health care budget and 27% of Medicare
budget.
At least one third of all Medicare expenditures
provide care for eventually fatal illnesses.
About 27%–30% of the total Medicare budget is
spent in the final year of life.
Of total amount spent in final year of life, nearly
40% is spent in the last 30 days.
Hospice care can save 25%–40% of health care
costs during the last month of life.
(Trupin, Rice, & Max, 1995)
One view of what we need to design a
successful health care system for the
future
Crossing the Quality Chasm:
A New Health System for the
21st century
—Institute of Medicine (IOM),
2001
IOM Report: Issues
Between the health care we have and the
care we could have lies not just a gap,
but a chasm.
A system full of under use, inappropriate
use, and overuse of care
A system unable to deliver today’s
science and technology; will be worse
with innovations in the pipeline
IOM Report: Issues
(cont.)
A fragmented system characterized by
unnecessary duplication, long waits, and
delays
Poor information systems and
disorganized knowledge
“Brownian motion” rather than
organizational redesign
A system designed for episodic care when
most disease is chronic
Health care providers operate in silos
IOM Report:
Recommendations
Commit to a national statement of
purpose for the health care system
Six aims
–
–
–
–
–
–
Safety: Avoid injuries
Effective, evidence-based practice
Patient-centered: Patient values guide
decisions
Timely: Reduce waiting and delay
Efficient: Avoid waste
Equitable: Care doesn’t vary by gender,
ethnicity, etc.
(IOM, 2001, pp. 5–6, 9–12)
IOM Report: Getting Evidence
Into Health Care Delivery
Ongoing analysis and synthesis of medical
evidence
Delineation of guidelines
Identification of best practices in design of care
processes
Better dissemination to professionals and public
Decision support tools
Goals for improvement
Measures of quality for priority conditions
(IOM, 2001, pp. 19–20)
Question:
Are today’s emerging
areas of practice
aligned with the needs
that will be present
in the year 2020?
Answer:
We can’t know with
certainty. But one approach
that will help answer that
question and guide planning
in an informed way involves
the creation of scenarios.
How to Best Think About the Future?
No absolute answer to the question, but
tarot cards and crystal balls are not the
answer.
Think of the drivers of change.
Use the drivers of change to imagine
different scenarios of the future.
Imagine at least three scenarios; each
should be plausible but different.
Step backward from future scenarios to
think about what to do now to prepare.
What is Scenario Planning?
A way of analyzing known trends in
order to imagine conditions that
define views of possible worlds
These possible worlds are used as
planning structures to guide thinking
about potential courses of action
Four Scenarios
A. Familiar Territory (Expected)
B. Scare City (Feared)
C. Bold New Frontier (Aspirational)
D. Shining City on the Hill (Visionary)
Scenario Profile Categories
Demographics
Health care
Mental and physical well-being
Design and technologies for quality living
Education
Occupational therapy practice
environment
OT Scenarios
Familiar Territory
Describes an expected
future with enough
opportunity for the
profession to progress
steadily along
Scare City
Bold New Frontier
Describes an aspired future
shaped by scientific and
technological advances
that could alter the
practice of occupational
therapy
Describes a feared
future where current
challenges cascade into
an era of limited
opportunities for
occupational therapy
Shining City on the Hill
Describes a visionary
future where a more
holistic view of health
transforms occupational
therapy and its role in
society
Familiar Territory
Expected Future Overview
Increasing numbers of elderly
people benefit from early
interventions, living longer and
with less disability
Community design aids mobility
Health care services become
more client-centered for clients
who have insurance or can
afford to pay
Schools diversify in their ability
to meet student needs
© Health Canada. Used with permission of the
Minister of Public Works and Government Services, Canada, 2005.
Scare City
Feared Future Overview
Increases in disability
overwhelm health care
and school systems
Promising alternatives
exist, but they elude
the majority
As resources for quality
of life grow scarce,
mental and physical
well-being decreases
© 2003 Kevin Bubriski. Used with permission.
The lucky few buy their
way up to the services
they need
Bold New Frontier
Aspirational Future Overview
© Independence Technology, LLC. A Johnson & Johnson Company.
Used with permission.
Advanced science
and technology
transforms health
care and learning
Buildings and
communities are
rationally designed
for mobility and
independence
Traditional
institutions are
yielding to distributed
venues for health,
education, and social
services
iBOT 3000 ™
Shining City on a Hill
Visionary Future Overview
The values of holistic
approach to health lead to
longer, more meaningful
lives for everyone
Prevention is reinforced
by caring relationships
People of all ages interact
in livable environments
Disabilities have lost their
stigma as people openly
pursue their full potential
Connecting the Dots
Current
State
Future
Scenario
Possible
Implications
Fewer than
1% of OTs work
in mental health.
Much content in
educational
programs is about
body structure and
function.
Mental illness is
becoming a major
health burden.
Developments in
stem cells, assistive
technologies, etc.,
may restore
functional ability.
Continuing
education,
education, licensure
Educational
programs may need
to shift focus to
lifestyle and QOL
strategies.
What Will Be Likely, Regardless of
Which Scenario is Closest to
Predicting the Future?
Demonstrating value/efficiency
Being clear about our mission
(scope of practice)
Putting patients first
Constantly trying to improve
Basing what we do on evidence
Addressing needs of elderly
Group Assignments
Rank importance of drivers for the
profession
Consider current conditions
Discuss scenarios
Identify population needs for OT in
the imagined world (scenario)
Identify changes needed to get there
in policy, education, practice, research
to the unreasonable
ones, the ones who
look forward not
backward, who are
certain only of
uncertainty, and who
have the ability and
the confidence to
think completely
differently.”1
- George Bernard Shaw
1Handy,
p. 16.
From Photos To Go Unlimited. Used with permission.
“The future belongs
Task Group Deliverables
•Group rank of importance of
drivers
•Specific ideas about needed
change in practice, education,
research, policy
•Summary of recommendations in
written form
•Demographic forms completed by
each group member
National Dialogue
Conference focus groups, RA,
ASAP, ASD
Collate, digest information
Encourage state area dialogues
with members and nonmembers
Interactive Web site
Planning council to digest
feedback and propose vision and
10-year plan (by 2007)
References
American Occupational Therapy Association. (2005). [Membership survey]. Unpublished raw data.
Centers for Medicare and Medicaid Services. (2005). Public programs: Medicare, Medicaid, SCHIP. In Health
Care System: Facts and Figures. Retrieved June 1, 2005 from
http://www.cms.hhs.gov/charts/healthcaresystem/chapter3.pdf
Handy, C. B. (1996). Beyond certainty: The changing worlds of organizations. Boston: Harvard Business
School Press.
Institute of Medicine. (2001). Crossing the quality chasm: A new health system for the 21st century.
Washington, DC: National Academy Press.
Murray, C. J. L., & Lopez, A. D. (Eds.) (1996). Summary: The global burden of disease: A comprehensive
assessment of mortality and disability from diseases, injuries, and risk factors in 1990 and projected to
2020. Cambridge, MA: Harvard School of Public Health on behalf of the World Health Organization and the
World Bank.
Narrow, W. E. (1999). One-year prevalence of mental disorders, excluding substance use disorders, in the
United States. Unpublished.
National Institute on Aging. (2002). Aging in the United States: Past, present, and future (NIH Publication
No. 95 4009). Washington, DC: U.S. Government Printing Office.
Robert Wood Johnson Foundation. (1996, August). Chronic care in America: A 21st century challenge. San
Francisco: Institute for Health & Aging: University of California.
Sculley, J. (1989). The relationship between business and higher education: A perspective on the 21st
century. Communications of the Association of Computing Machinery, 32, 1056–1061.
The Center for Universal Design. (1997). The Principles of Universal Design, Version 2.0 Raleigh, NC: North
Carolina State University.
ThinkExist.com. (2005a). Retrieved June 1, 2005, from http://en.thinkexist.com/quotes/mahatma_gandhi
ThinkExist.com. (2005b). Retrieved June 1, 2005 from http://en.thinkexist.com/quotes/wayne_gretzky
Trupin, L., Rice, D., & Max, W. (1995). Medical expenditures for people with disabilities in the United States,
1987. San Francisco: University of California.
VanItallie, T. B. (2002). Stress: A risk factor for serious illness. Metabolism: Clinical and Experimental, 51(6
Suppl. 1), 40–45.
Acknowledgments
This slide presentation was
developed by the AOTA VicePresident pursuant to his
responsibilities for Strategic
Planning. Appreciation is extended to
Carolyn Baum, PhD, Leti Ford, Judy
Wolf, Maureen Peterson, Cynthia
Johansson, and Barbara Dickson for
their assistance in its preparation.
© 2005 by the American Occupational Therapy Association, Inc. All rights
reserved.