XPECT Study
Physician Presentation
XPECT Study1 Purpose
• Quantify the performance of the first
implantable leadless cardiac monitor (ICM)
with dedicated AF detection capabilities
1 Hindricks G, Pokushalov E, Urban L, Taborsky M, Kuck K. Performance of a new leadless
implantable cardiac monitor in detecting and quantifying atrial fibrillation: results of the XPECT trial.
Circulation. Arrhythmia and Electrophysiology. Published online February 16, 2010.
Background
Occurrence of Asymptomatic AF
and Reliability of Symptoms
Strickberger1
Methods:
• Multicenter trial following 48 patients for
12 months to correlate pacemaker-detected
atrial tachyarrhythmia (AT) events with
symptoms
Results/Conclusions:
• “Almost 95% of documented AT episodes
were asymptomatic, and symptoms attributed
to atrial fibrillation were associated with AT
only approximately 15% of the time.”
• “No significant differences in the specific
symptoms that correlated with or without a
documented atrial tachyarrhythmia were
observed.”
1
Strickberger SA, et al. Heart Rhythm. 2005;2:125-131.
Unpredictable and Late
Recurrences of AF
ID
24
1
0
24
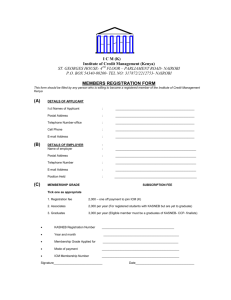
Martinek2
2
0
24
3
Methods:
0
24
4
0
24
• Fourteen patients with an
implanted pacemaker device
were selected for
radiofrequency ablation, with a
mean follow-up of 41.4 months
5
0
24
6
0
24
7
0
24
8
0
24
9
0
24
10
• “Continuous monitoring is able
to detect significantly more AF
episodes than routine followup. AF may reoccur very late
after long-lasting (>1 year)
episode-free intervals.”
2
Martinek M, et al. J Cardiovasc Electrophysiol. 2007;18:818-823.
ATB (hours/day)
Results/Conclusions:
0
24
11
0
24
12
0
24
13
0
24
14
0
-36
-24
-12
0
12
24
36
PRE
48
60
72
POST
MONTHS FROM ABLATION
Atrial tachyarrhythmia burden plot (ATB, hours per day) in all 14 patients over time. Zero
line indicates first ablation procedure; additional late-term ablations are marked by arrows.
Intermittent and Symptom-Based
Monitoring
Ziegler3
Methods:
• Data from 574 AT500 IPG patients were
analyzed retrospectively over 1 year
• Intermittent monitoring was simulated by
analyzing data from randomly selected
days within a prescribed monitoring
window
Results/Conclusions:
• “Intermittent and symptom-based monitoring
is highly inaccurate for identifying patients
with any or long-duration AT/AF and for
assessing AT/AF burden.”
3
Ziegler P, et al. Heart Rhythm. 2006;3:1445-1452.
Example: Quarterly Holter recordings detect AF in 54% of the patients
with AF, and is correct 29% of the time in ruling out AF in patients.
Relationship between Atrial
Arrhythmia Burden and Stroke Risk
Glotzer4
AT/AF Burden Subset
Methods:
• Prospective, observational study
analyzing 2,486 patients with ≥ 1 stroke
risk receiving pacemakers or defibrillators
that monitor atrial tachycardia (AT)/AF
burden
• Annualized TE rates were determined
according to AT/AF burden subsets: zero,
low (< 5.5 hours [median duration of
subsets with nonzero burden]), and high
(≥ 5.5 hours)
Results/Conclusions:
• AT/AF burden ≥ 5.5 hours on any of
30 prior days appeared to double TE risk
4
Glotzer T, et al. Circ Arrhythm Electrophysiol. 2009;2:474-480.
Annualized TE Rate
(95% Confidence
Interval)
Zero AT/AF burden
1.1 [0.8, 1.6] %
Low AT/AF burden (< 5.5 hours)
1.1 [0.4, 2.8] %
High AT/AF burden (≥ 5.5 hours)
2.4 [1.2, 4.5] %
Implications of Varying Levels
of AF on Stroke Risk
Botto5
Methods:
• Analysis of 568 patients with an IPG and a
history of AF
• Three AF groups were considered: patients
with < 5-minutes AF on 1 day (AF-free);
patients with > 5-minutes AF on 1 day but
< 24 hours (AF-5 minutes); patients with AF
episodes > 24 hours (AF-24 hours)
Results/Conclusions:
• “In patients with recurrent AF episodes, risk
stratification for thromboembolic events can be
improved by combining CHADS2 score with
AF presence/duration.”
5
Botto G, et al. J Cardiovasc Electrophysiol. 2009;20:241-248.
Risk of Thromboembolic Events
Consensus Conference
on Trials in AF
• Assessment of rhythm
• “To assess freedom from AF, continuous ECG recording is the
gold standard.”
• “This gold standard is not available at present, and will be available
only using advanced technology (implanted devices or special
garments with ECG-recording capabilities and satellite- or GSM-based
transmission) in the foreseeable future.”1
• 2009 EHRA position paper on indications for the use of loop
recorders
• “…only continuous monitoring is able to elucidate the full amount
of symptomatic and asymptomatic AF episodes.”2
1
2
Kirchhof P, et al. Europace. 2007;9:1006-1023.
Brignole, et al. Europace. 2009;11:671-687.
Indications
The Reveal® XT Insertable Cardiac Monitor is an
implantable patient-activated and automatically
activated monitoring system that records
subcutaneous ECG and is indicated in the following
cases:
• Patients with clinical syndromes or situations at
increased risk of cardiac arrhythmias
• Patients who experience transient symptoms such
as dizziness, palpitation, syncope, and chest pain,
that may suggest a cardiac arrhythmia
Reveal® XT
Implantable Cardiac Monitor (ICM)
• 49.5 minutes of ECG storage, with additional episode logs
(22.5 minutes patient-activated and 27 minutes auto-activated
ECG data)
• 3 years longevity
• MRI conditional (tested with 1.5 and 3 Tesla)
• Triggers: AT/AF detection; asystole, Brady, VT/FVT
• Cardiac Compass® summary report
• Histograms (ventricular rate during AF, AF duration)
• Remote patient management through the Medtronic
CareLink® Network
Reveal® XT Clinician Manual
Information recorded in the Reveal® XT ICM may help you to
monitor and assess the patient’s condition in the following ways:
• Monitor the patient’s AT/AF burden and the occurrence of asymptomatic
episodes of AT/AF, to assess whether medical treatment is necessary or
should be adjusted
• Monitor the patient’s ventricular rhythm during atrial arrhythmia episodes, to
assess whether a rate control therapy is having the desired effect or needs
to be adapted
• Record incidents of symptomatic events to correlate symptoms with cardiac
rhythm and aid diagnosis
• Continuously record other patient information that may help you to assess
the patient’s condition, such as heart rate variability or patient activity
Source: Reveal ® XT Clinician Manual
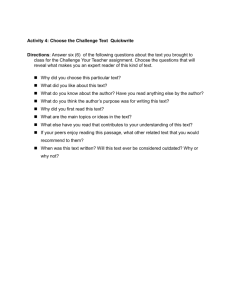
ICM Detection Algorithm
AF detection via R-R variability pattern recognition
Atrial Fibrillation
Normal Sinus Rhythm
2 minutes
Automatic detection
Source: Reveal ® XT Clinician Manual
Study Overview
• Purpose:
– To quantify the AF detection performance of the Reveal® XT ICM
• Method:
– Comparative analysis of automatically detected AF episodes
by Reveal® XT ICM and 46 hours of Holter recordings
– All arrhythmias detected on the surface ECG were reviewed on a
beat-by-beat basis by a cardiologist (blinded to Reveal® XT ICM data)
• 24 enrolling study sites from Europe and Canada, 247 patients
enrolled
• 206 patients included in analysis, 76 (36.9%) had AF during
the study
Results: Patient Population
• Gender:
• Age:
66.8% male, 33.2% female
57 ± 10 years (26 – 82 years)
• Hypertension:
• Diabetes:
• Prior CVA or TIA:
55.3%
7.7%
10.2%
• Any structural cardiovascular disease:
–
–
–
–
–
CAD:
Valvular disease:
MI:
HF:
Nonischemic cardiomyopathy:
27.6%
16.7%
6.5%
5.7%
2.8%
1.6%
1:1 Comparison of Holter
and ICM Data
False positive episodes
Correctly detected episode
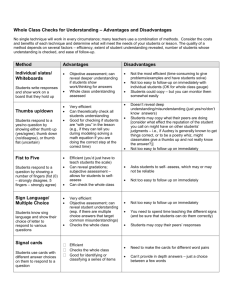
Results (I)
Patient detection
metrics:
247 patients enrolled
206 patients with analyzable
Holter recordings
76 patients had AF on Holter
71 patients had
AF burden
> 1% on Holter
71 patients had
AF classified
by ICM
130 patients had no AF on Holter
5 patients had
AF burden
< 1% on Holter
3 patients had
no AF classified
by ICM
2 patients had
AF classified
by ICM
111 patients had
no AF classified
by ICM
Sensitivity
96.1%
Specificity
85.4%
PPV
79.3%
NPV
97.4%
19 patients had
AF classified
by ICM
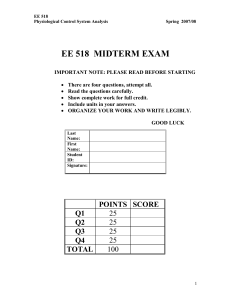
Results (II)
AF Burden (Pearson correlation)
AF Burden metrics:
Sensitivity
98.1%
Specificity
98.5%
PPV
91.9%
NPV
99.7%
Results (III)
AF Episode Detection Performance
Conclusions
• Continuous monitoring with Reveal® XT ICM reliably
identifies patients with AF (sensitivity = 96.1%) and
correctly confirms the absence of AF (negative
predictive value = 97.4%) in patients without AF
• Reveal® XT ICM is the only insertable continuous
monitoring device with a dedicated AF detection
algorithm and a published clinical study that provides
the information physicians need to make informed
decisions
When May Continuous Long-Term Monitoring Be
an Applicable Option?
• To detect AF in patients who experience transient symptoms or are at
high risk for the presence of AF (e.g., cryptogenic stroke)1
• To provide information that may assist in AF patient management
strategies such as:
1. Determine if an AF patient is in sinus rhythm following a rhythm control
intervention (e.g., antiarrhythmic drugs, cardioversion, ablation) to guide
ongoing therapy2
2. Monitor the patient’s ventricular rhythm during AF episodes to assess if
rate control therapy is effective or needs to be adapted3 (e.g., beta
blockers, AV nodal ablation)
3. Document AF presence and duration to assist in anticoagulation
management in intermediate stroke risk patients4 (e.g., CHADS 1 or 2
patients)
1
Kimmel SE, et al. Arch Intern Med. 2007;167:229-235.
Ziegler P, et al. Heart Rhythm. 2006; 3:1445-1452.
3 Ziegler, et al. Poor ventricular rate control in the persistent versus paroxysmal atrial fibrillation population:
continuous monitoring data from 141,231 patients in the CareLink® database. Poster submitted HRS, May 2009.
4 Botto GL, et al. J Cardiovasc Electrophysiol. 2009;20:241-248.
2
Backup
Brief Statement
Indications
9529 Reveal® XT Insertable Cardiac Monitor
The Reveal ® XT Insertable Cardiac Monitor is an implantable patient-activated and automatically activated monitoring system that records
subcutaneous ECG and is indicated in the following cases:
patients with clinical syndromes or situations at increased risk of cardiac arrhythmias
patients who experience transient symptoms such as dizziness, palpitation, syncope, and chest pain, that may suggest a cardiac arrhythmia
9539 Reveal® XT Patient Assistant
The Reveal ® XT Patient Assistant is intended for unsupervised patient use away from a hospital or clinic. The Patient Assistant activates one
or more of the data management features in the Reveal Insertable Cardiac Monitor:
To verify whether the implanted device has detected a suspected arrhythmia or device related event.
To initiate recording of cardiac event data in the implanted device memory.
Contraindications
There are no known contraindications for the implant of the Reveal ® XT Insertable Cardiac Monitor. However, the patient’s particular medical
condition may dictate whether or not a subcutaneous, chronically implanted device can be tolerated.
Warnings/Precautions
9529 Reveal ® XT Insertable Cardiac Monitor
Patients with the Reveal ® XT Insertable Cardiac Monitor should avoid sources of diathermy, high sources of radiation, electrosurgical cautery,
external defibrillation, lithotripsy, therapeutic ultrasound, and radiofrequency ablation to avoid electrical reset of the device, and/or inappropriate
sensing. MRI scans should be performed only in a specified MR environment under specified conditions as described in the device manual.
9539 Reveal ® XT Patient Assistant
Operation of the Model 9539 Patient Assistant near sources of electromagnetic interference, such as cellular phones, computer monitors, etc.,
may adversely affect the performance of this device.
Potential Complications
Potential complications include, but are not limited to, device rejection phenomena (including local tissue reaction), device migration, infection,
and erosion through the skin.
See the device manual for detailed information regarding the implant procedure, indications, contraindications, warnings, precautions, and
potential complications/adverse events. For further information, please call Medtronic at 1 (800) 328-2518 and/or consult Medtronic’s website at
www.medtronic.com.
Caution: Federal law (USA) restricts this device to sale by or on the order of a physician.
www.medtronic.com
World Headquarters
Medtronic, Inc.
710 Medtronic parkway
Minneapolis, MN 55432-5604
USA
Tel: (763) 514-4000
Fax: (763) 514-4879
Medtronic USA, Inc.
Toll-free: 1 (800) 328-2518
(24-hour technical support for
physicians and professionals)
UC201004626 EN
© Medtronic, Inc. 2010
Minneapolis, MN
All Rights Reserved
01/2010