Hospital Financial Assessment: NICU Lactation Program Justification
advertisement

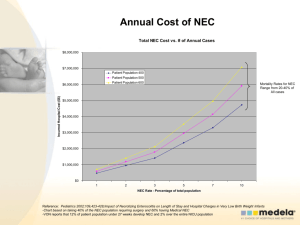
Hospital Financial Assessment Annual Cost of NEC Total NEC Cost vs. # of Annual Cases $8,000,000 $7,000,000 Patient Population 400 Patient Population 500 Patient Population 600 Incurred Hospital Cost ($$) $6,000,000 Mortality Rates for NEC Range from 20-40% of All cases $5,000,000 $4,000,000 $3,000,000 $2,000,000 $1,000,000 $0 1 2 3 5 7 10 NEC Rate - Percentage of total population Reference: Pediatrics 2002;109,423-428;Impact of Necrotizing Enterocolitis on Length of Stay and Hospital Charges in Very Low Birth Weight Infants -Chart based on taking 40% of the NEC population requiring surgery and 60% having Medical NEC -VON reports that 12% of patient population under 27 weeks develop NEC and 2% over the entire NICU population Increased Breastmilk Usage Translating into Savings • • • • Exclusively formula fed babies are 6-7 more times likely to develop NEC than exclusively breastmilk fed babies and 3 times more likely than those receiving both. (Graph assumes a 7x increase) Chart Based on VON data of ~50% as a baseline of Population receiving some breastmilk by discharge Baseline NEC rates are on the bottom and are represented with the 50% BF rate. By increasing the BF rates, the NEC percentages decrease Based Hospital Admission of 500 annually 6,000,000 Hospital Incurred Cost ($$) 5,000,000 4,000,000 50% BF Rate Baseline 60% BF Scenario 70% BF Scenario 80% BF Scenario 90% BF Scenario 100% BF Scenario 3,000,000 2,000,000 1,000,000 0 Baseline 1%NEC Baseline 3%NEC Baseline 5%NEC Baseline 7%NEC Baseline 10%NEC NEC • Medical NEC – – – – exhibits signs/symptoms without perforation Adds 22 additional days to LOS Increases death by 14% Overall hospital charges $300,000 $73K in incremental hospital charges • Surgical NEC – – – – radiographic evidence of perforated bowel Adds 60 additional days to LOS Increases death by 24.5% Overall hospital charges $450,000 $190K in incremental hospital charges Additional Benefits of Breastmilk in the NICU Outcome Fortified HM Preterm Formula 19+21 33+41 1(1.6%) 6(13%) 0 3 Late-Onset Sepsis n, (%) 19(31%) 22(48%) Late-Onset Sepsis # of episodes/patient 0.3+0.5 0.6+0.7 Positive Blood Cultures (#/infant) 0.5+0.9 1.2+1.7 NEC or Sepsis, n (%) 19(31%) 25(54%) 16% 39% O2 Therapy (days) NEC (n) Surgical NEC (n) GERD Medications (%) Schanler et al., Pediatrics 103, 1999;1150-1157 For every 10-ml/kg per day increase in Breastmilk ingestion: • The Mental Development Index Increased by 0.53 points • The Psychomotor Development Index increased by 0.63 points • Behavior Rating Scale Percentile Score increased by 0.82 points • Likelihood of rehospitalization decreased by 6% Vohr et al., Beneficial effects of breastmilk in the neonatal intensive care unit on the developmental outcome of extremely low birthweight infants at 18 months of age; Pediatrics 2006;118;e115-e123 Impact of a Strong Lactation Program for Neonates 2 Year Study Performed at Children’s Hospital of the King’s Daughters in Norfolk, VA • Usual Support encompassed period between 1996-1998 when no lactation support was available • IBCLC Support encompassed 2 full time IBCLC’s with RN backgrounds and a 3rd in training Gonzalez et al.,Journal of Human Lactation 2003:19:286 Cost Benefit of a NICU Lactation Program Lactation FTE’s – Assume $100,000 (Salary + Benefits) Assume RN with IBCLC Assume 2 FTE = $200,000 Pumps No Charge Kits Based on 500 Annual Admissions 80% Breastfeeding Rate Total Kits Consumed 400 + 20% contingency for replacements Total Kits Consumed 480 $13,000 Annually Containers Assume Annual Usage of 140,000 units Annual Cost = $35,000 Total Cost: $257,000 annually References