Radiological aspects of bone giant cell tumor
advertisement

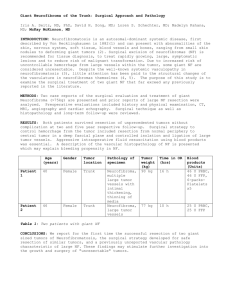
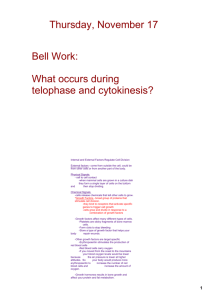
MK4 Giant cell tumor of the bone is a relatively uncommon tumor usually regarded as benign tumor with local aggressiveness. In this work we detail the appearance of this tumor in the various radiological examinations, namely the standard radiography, CT and MRI and we describe the signs in favor of the diagnosis. We report the case of 3 patients ,explored in our service ,for tumefaction of periarticular tissues in two cases and bone pain in 1 case . All patients had a radiography and MRI . One patient also had a CT . Diagnosis raised by radiological exploration, was confirmed after biopsy of the tumor in all cases. 27-year-old patient left hip pain for two years with partial functional imptence . X RAY Expansile, osteolytic, radiolucent lesions without sclerotic margins and without a periosteal reaction ,located in sacrum . Intralesionnel septa ,cortical destruction , and soft-tissue masses. CT Voluminous expansive process of the left sacral wing responsible for a replacement cord with rupture of the anterior and posterior cortical bone, with significant endopelvi expansion displacing the rectum to the right side . This process extends to the sacral body, measuring 10cm long axis, invaded the joint space with extension into the controlateral iliac wing . On MRI, this process is of mixed signal, low signal T1, isointense T2, with areas of hyperintensity and nodular hyposignal. AX T2 FAT SAT SAG T2 Those zones are enhanced in a heterogeneous way, landscaping hypointense areas of necrosis Intraducta extension encompassing the first sacred nerve. Extension to the gluteal region AX T1 CORO T1 FAT SAT GADO •25 old girl •Painful subcutaneous mass ,adjacent to the left wrist •Rapid evolution. •Metaphyseal epiphyseal osteolytic eccentric lesion ,of the distal radius, with fine internal partitions . •Extends to the subchondral bone, thinner and blows cortical. •Compact periosteal reaction and invasion of soft tissues AX T1 SAG T1 CORO T1 CORO T2 •Epiphyseal metaphyseal expansive process of the distal let radius. •Hypointense T1 and T2, enhances after gadolinium injection. • Cortical blowing, and replacement cord •Breach of the anterior and posterior cortex with extension to soft tissue . CORO T1 SAG T1 FAT SAT GADO 34 old patient Painful subcutaneous mass ,adjacent to the wright wrist. Ax T1 Ax T2 Ax T2 AXT1 FAT SAT GADO CORO T1 CORO T1 FAT SAT GADO Epiphyseal metaphyseal tumor lesion of the right radius, measuring 5.5 x 4.7 cm , with sharp contours hypointense on T1and T2, with intense heterogeneous enhancement. blows the cortical lesion which seems broken in some places and extends to the adjacent soft tissues Most giant cell tumors occur in the long bones; approximately 50% are located in the bones around the knee. Location is important in the diagnosis of giant cell tumor. Most tumors are eccentric and are seen in a subarticular location ; however, the tumor originates in the metaphysis, and the common epiphyseal involvement is the result of the patient's skeletal maturity . Early lesions may lie solely in the metaphysis. A narrow zone of transition with a lack of sclerosis at its margins is a distinctive finding and strongly suggestive of the diagnosis. When sclerosis of the tumor margins is present, it is seldom complete. Periosteal reactions are not usually seen; the lack of a host-reactive response is typical of giant cell tumors. Giant cell tumors in the spine are uncommon and account for only 5% of giant cell tumors. The sacrum is the most common location. Patients with these tumors tend to be slightly younger than those with tumors in the appendicular skeleton. The location in the vertebrae can vary, but the tumor most commonly involves the vertebral body. The radiographic appearance of giant cell tumors is often characteristic. On radiographs, typical giant cell tumors are usually easily distinguished from other bone tumors. Giant cell tumors are lytic, subarticular, and eccentric, and they are often lacking a sclerotic rim; however, unusual variants may make the radiographic diagnosis difficult. On radiographs, the tumors may be seen in areas of destruction of the vertebral body with invasion of the posterior elements. The tumor can cause vertebral collapse and spinal cord compression, especially when it involves the posterior elements. The degree of confidence is high for radiography in the appendicular skeleton. In the spine, the degree of diagnostic confidence is not high, as giant cell tumors usually cannot be differentiated from other types of tumors. Tumors in the sacrum are recognizable, and these may be diagnosed on the basis of their appearance and location. Unusual forms of certain tumors may mimic giant cell tumors. Telangiectatic or fibrogenic variants of osteosarcoma may not produce visible ossifications or calcifications. These variants may be eccentric and may extend to the subarticular surface, mimicking a giant cell tumor. Malignant fibrous histiocytomas occur in a similar age group and can also mimic a giant cell tumor. Brown tumors of hyperparathyroidism are well known in the differential diagnosis of giant cell tumors. Chondroblastomas may be mistaken for giant cell tumors because of their subarticular location; however, careful review of the radiographs usually reveals that the epicenter lies in the epiphysis rather than in the metaphysis. The presence of chondroid calcifications further supports the diagnosis of chondroblastoma. Aneurysmal bone cysts may be only slightly expansile in the early stages, and they can extend to the subarticular cortex, mimicking a giant cell tumor. These cysts usually occur in younger patients. Approximately 29% of aneurysmal bone cysts are reported to be associated with some other solid bone lesion, 39% of which are giant cell tumors CT findings are similar to radiographic findings for giant cell tumor of bone. Marginal sclerosis, cortical destruction, and soft-tissue masses are seen more clearly on CT scans than on radiographs. Fluid-fluid levels are occasionally seen but are not specific. CT does not usually add much diagnostic information to the radiographic results. CT scans are more useful in complex-shaped bones, such as the vertebrae or pelvic bones, because the details of the lesion may not be depicted well on radiographs. CT is also useful in surgical planning. CT scans are usually less useful than are other examinations. Magnetic resonance imaging (MRI) is sensitive for the detection of soft-tissue changes, intra-articular extension, and marrow changes. MRI is the best method for assessing subchondral breakthrough and extension of tumor into an adjacent joint. On T1-weighted images, giant cell tumors may show heterogeneous or homogeneous signal intensity characteristics. The signal intensity is usually low or intermediate, but areas of high signal intensity, caused by recent hemorrhage, may be noted. On T2-weighted images, heterogeneous low to intermediate signal intensity is seen in solid areas of the tumor . Areas of low signal intensity may be exaggerated on T2-weighted, spin-echo images, and these may be even more exaggerated on gradient-echo weighted images because of the presence of hemosiderin. Hemosiderin is detected in more than 63% of giant cell tumors, and its presence is probably the result of extravasated red blood cells coupled with the phagocytic function of the tumor cells. Cystic areas are common and are seen as areas of high signal intensity on T2-weighted images. Fluid-fluid levels may be seen, as in the image below. Peritumoral edema is uncommon in the absence of a fracture. The tumor is usually heterogeneously enhancing with the intravenous administration of contrast material The degree of confidence in imaging the appendicular skeleton is high for MRI. The modality is sensitive in the detection of soft-tissue changes, intra-articular extension, and marrow changes. MRI is the best method for assessing subchondral breakthrough and the extension of tumor into an adjacent joint. Its diagnostic accuracy is high, especially when MRIs are interpreted in conjunction with plain radiographs. In the spine, tumors such as osteoblastomas and aneurysmal bone cysts, as well as metastases, may be found in the same location as giant cell tumors, and they may have overlapping MRI characteristics. The disadvantages of MRI are its relatively high cost and limited availability. In addition, some patients experience claustrophobia during the examination and may require sedation. MRI is also contraindicated in patients with cardiac pacemakers , orbital foreign bodies, and noncompatible anevrysmal clips. The diagnostic accuracy of MRI is high, especially when MRIs are interpreted in conjunction with plain radiographs. MRI ,when interpreted in conjunction with radiography enable to suggest the diagnosis of bone giant cell tumor thanks to its high diagnostic accuracy. The radiographic appearance ,although very suggestive diagnosis ,must discuss other etiologies.