GI26
advertisement

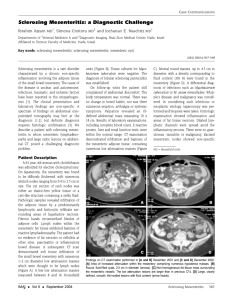
IDIOPATHIC MESENTERIC PANNICULITIS M. LIMEME, H. ZAGHOUANI BEN ALAYA, H. AMARA, D. BEKIR, CH. KRAIEM Imaging department, Farhat Hached Hospital, Sousse, Tunisia GI26 Introduction • Synonyms: retractile mesenteritis, fibrosing mesenteritis, mesenteric panniculitis, mesenteric lipodystrophy, liposclerotic mesenteritis, systemic nodular panniculitis. • Definitions: Complex mesenteric inflammatory disorder of unknown etiology Objectives To describe the imaging features of nonspecific inflammation of mesenteric fat tissue without associated pathology and to formulate differential diagnosis. Materials and Methods • Among two men and a women (mean age 45 years), 2 were paifull, • Diarrhea was noted in two cases, • And fever in one case. • An abdominal mass was found in two cases, • 3 patients had an inflammatory syndrome. Results • The diagnosis was suggested by computed tomography (CT): (single mass: 2 cases, diffuse mesenteric thickening: 1 case) and confirmed by pathology. • Two patients were treated with corticosteroids. During the follow-up (mean 56 months) the panniculitis was stable on CT in 2 cases and regressed in one case. • No associated pathology has emerged. Abdominal pain and diarrhea CT findings: fat ring sign (arrowheads) and tumoral pseudocapsule (arrow). Abdominal pain and diarrhea CT findings: Solid soft tissu mass in the root of small bowel mesentery ecasing mesenteric vessels. Abdominal mass and fever CT findings: extensive infiltration of small bowel mesentery ecasing mesenteric vessels. Discussion Clinical issues • Symptoms: Abdominal pain, fever, nausea, vomiting, weight loss, diarrhea. Palpable mass. Incidental finding in an asymptomatic patient. CT findings Findings vary depending on predominant tissue • Area of subtle increesed attenuation in mesentery (inflamed fat): solitary/multiple; well/ill defined • Calcification, enlarged mesenteric lymph nodes, • Fatty necrotic cystic mass may be seen, • Infiltration of pancreas or portahepatis, • Encasement of mesenteric vessels and collateral vessels: narrowing/occlusion on contrast study Increesed attenuation in mesentery (red arrow) with well defined outlines: pseudocapsule. Encasement of mesenteric vessels and collateral vessels (blue arrow) CT findings • « Fat ring » sign: preservation of fat arround vessels: - Hypodense fatty halo surrounding mesenteric vessels and nodules, - Predominantly seen in mesenteric panniculitis, - Differentiates scleroing mesenteritis from other mesenteric processes (lymphoma, carcinoid tumor, carcinomatosis) « Fat ring » sign: preservation of fat arround vessels Horton and al. Radiographics. 2003 ;23(6):1561-7 CT findings • Pseudocapsule: peripheral band of soft tissue attenuation that limits normal mesentery from inflammatory process: - Seen in mesenteric panniculitis phase, - Enhancement of pseudocapsule may be seen. • Thickening/infiltration/displacement/narrowing of bowel loops. Pseudocapsule: peripheral band of soft tissue attenuation that limits normal mesentery from inflammatory process CT findings • - « Misty mesentery »: nonspecific sign Increesed attenuation of mesentery, Evidence of small mesenteric nodes, No discret soft tissu mass, Seen in any pathology that infiltrates mesentery CT findings • Solid soft tissu mass usually in root of small bowel mesentery (fibroous tissue) - Single/large/lobulated/ill-defined increesed density mass with linear radiating strands (fibroma-rare) - Small mesenteric soft tissue nodules of increesed density (fibromatosis) MRI findings • Variable signal intensity due to: inflammation, fat, fibrosis, vascular and Ca++. • Mesenteric panniculitis and lipodystrophy: - T1WI: mixed signal intensity, - T2WI: mixed signal intensity. • Retractile mesenteritis: in mature fibrotic reaction - T1WI: decreesed signal intensity, - T2WI: very low signal intensity, - Gradient-écho MR image: *Narrowing/occlusion of flow in mesenteric vessels *Collateral vessels are seen Differential diagnosis • • • • • Non-Hodgkin lymphoma, Carcinoid tumor, Mesenteric edema, Desmoid tumor (Fibromatosis), Carcinomatosis (mesenteric metastasis) Differential diagnosis Non-Hodgkin lymphoma Differential diagnosis Carcinoid tumor Differential diagnosis Mesenteric edema Differential diagnosis Desmoid tumor Differential diagnosis Carcinomatosis (mesenteric metastasis) Treatment • Steroids, colchicine, immunosuppressive agents: before fibrotic changes. • Surgical excision: fibrosis and retraction with obstructive symptoms. Conclusion • Various diseases (usually malignant) can mimic the imaging features or be associated. • Pathological verification leads to affirm the idiopathic mesenteric panniculitis, a benign entity of unknown pathogenesis. • Corticosteroid therapy is reserved for symptomatic patients.