Antibiotic Review - Stoller Design Group
advertisement

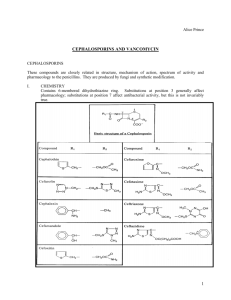
Module 2 (of 3): Antibiotic Review* Review of selected antimicrobials By Keith Teelucksingh, PharmD Infectious Disease Pharmacist, Kaiser Permanente Vallejo With contributions by Linh Van, PharmD Infectious Disease Pharmacist, Kaiser Permanente Oakland See Notes Goals Build upon pharmacists’ basic knowledge of selected broad-spectrum antibiotics Provide contemporary clinical information on appropriate use, spectrum of activity, clinical pearls and other considerations of selected antibiotics. Objectives Upon completion of this module, the participant will be able to: 1. Elaborate on the spectrum activity for the βlactam-related antibiotics, aztreonam, vancomycin, clindamycin, metronidazole and the fluoroquinolones 2. Discuss the appropriate clinical uses of the broad spectrum β-lactam-related antibiotics and vancomycin Objectives 3. 4. Describe the appropriate use of the antianaerobic agents clindamycin and metronidazole when combined with other anaerobically active antibiotics Describe the appropriate use of β-lactam agents and vancomycin agents for the treatment of certain bacteria Antibiotics to be Covered β-Lactams Penicillins Cephalosporins Carbapenems Monobactams Aztreonam Quinolones Moxifloxacin Ciprofloxacin Other Clindamycin Metronidazole Vancomycin Adapted from Brett Heintz, PharmD, BCPS β-Lactams Natural penicillins: penicillin Penicillinase-resistant penicillins: nafcillin, dicloxacillin Aminopenicillins: ampicillin, amoxicillin Extended spectrum penicillins: pipercillin, ticarcillin β-lactam/β-lactamase inhibitor combinations: Zosyn®, Unasyn®, Augmentin®, Timentin® Penicillins Penicillin G (IV) Used for treatment of Neurosyphilis, endocarditis due to susceptible pathogens Infections due to penicillin (PCN) susceptible (S) organisms: Group A & B Streptococci, Clostridium perfringes (gas gangrene) If organism is PCN S (does not produce penicillinase, e.g., Staphylococcus aureus) penicillin, amoxicillin, ampicillin can all be used Penicillins Penicillin G Side effects Allergic reactions (rash, blood dyscrasias, anaphylaxis) -> discussed in more detail in Module 3 Interstitial nephritis Hyperkalemia Phlebitis Penicillins Nafcillin Coverage: Staphylococcus aureus (MSSA) drug of choice Not as active versus other Gm + Does not cover Enterococcus, not as good as penicillin for S. pneumoniae, S. pyogenes Hepatobiliary clearance No need to adjust in renal dysfunction Note: Even though nafcillin is not renally eliminated, it still can cause interstitial nephritis Penicillins Nafcillin When interpreting susceptibilities: oxacillin = nafcillin Susceptibility to nafcillin predicts susceptibility to cefazolin/cephalexin Penicillins Nafcillin Side Effects Interstitial nephritis Neutropenia Still monitor serum creatinine if on long course Usually seen with longer courses Phlebitis Usually occurs when given peripherally Use central venous catheter or isotonic solution Penicillins Ampicillin/amoxicillin Drug of choice for Enterococcus spp. infections Amoxicillin (PO) If isolate is ampicillin/amoxicillin sensitive Higher dose used for S. pneumoniae (otitis media, pharyngitis) Enterococcal UTI Ampicillin (IV) Serious infections due to Enterococcus spp. Listeria (unpasteurized cheeses) infections typically added for coverage in meningitis Penicillins Ampicillin: clinical applications Endocarditis/bacteremia No one agent is bactericidal against Enterococcus spp. Ampicillin 2g IV q 4h Bactericidal when combined with aminoglycoside (AG) If treating endocarditis, addition of AG is strongly recommended Formal ID consult recommended Penicillins Pharmacokinetic considerations Bioavailability (oral) Amoxicillin, Dicloxacillin > Ampicillin> PCN VK High concentration in urine All need to be adjusted in renal dysfunction Exceptions: nafcillin, dicloxacillin Penicillins Ampicillin/amoxicillin Side effects (in general, similar to penicillin) Allergic reactions Rash Eosinophilia Leukopenia Extended Spectrum Penicillins * Piperacillin Good activity vs. Pseudomonas and Enterococcus Less active vs. E. coli TicarcillinNF Good activity vs. Pseudomonas (alternative to piperacillin) Less active than piperacillin vs. Enterococcus Not commercially available NF = non formulary See Notes βL/βLi* combinations Unasyn® (ampicillin/sulbactam) Augmentin® (amoxicillin/clavulanic acid) Zosyn® (piperacillin/tazobactam) Timentin® (ticarcillin/clavulanic acid) NF *βL/βLi = β-lactam/β-lactamaseinhibitor NF = non-formulary βL/βLi combinations All will cover ampicillin-sensitive Enterococci All have excellent activity vs. anaerobes B. fragilis, Prevotella spp. Unasyn® and Augmentin® do not cover Pseudomonas Addition of βLi adds activity against: Bacteroidies (anaerobes), β-lactamase producing Gm – (E. coli, Klebsiella, Serratia) & Gm + (Enterococci, MSSA) βL/βLi combinations * Unasyn® (ampicillin/sulbactam) Good for Gm + MSSA/Strep spp./Enterococcus spp. Uses: Diabetic foot ulcers, cellulitis, communityacquired pneumonia, mild community-acquired GI infections (diverticulitis) Variable Gm - coverage E. coli has high resistance Best in class for Acinetobacter (if isolate S) See Notes βL/βLi combinations Augmentin® (amoxicillin/clavulanic acid) Gram + coverage similar to Unasyn® Sometimes more active versus Gram – pathogens such as E. coli and Klebsiella spp. than Unasyn® Only PO option in class GI tolerance poor Uses: diverticulitis, cellulitis Good oral step-down therapy βL/βLi combinations Zosyn® (piperacillin/tazobactam) Expanded coverage compared to Unasyn® Similar to Timentin® may be slightly more active versus certain bacteria (E. coli) Good activity vs. Pseudomonas The addition of tazobactam to piperacillin adds NO extra activity vs. Pseudomonas For confirmed pseudomonal infections, increase dose to 4.5g IV q6h (renal function permitting) to maximize its pharmacodynamic properties vs. Pseudomonas βL/βLi combinations * Zosyn® (piperacillin/tazobactam) Clinical uses: severe intra-abdominal infections, health care-associated (HCA) infections, including pneumonia/ventilator-associated pneumonia Use should be reserved for patients with risk factors for nosocomial/drug resistant pathogens: Skilled nursing facility residents, previous antibiotics exposure, exposure to health care environment, immunocompromised patients See Notes βL/βLi combinations Timentin® (ticarcillin/clavulanicacid)NF Per previous slide, very similar coverage compared to Zosyn® May be used as alternative agent for infections due to Stenoptrophomonasmaltophilia NF = non-formulary βL/βLi combinations Side effects: overall, very similar to penicillins Zosyn® Thrombocytopenia has been seen with longer courses of therapy and higher doses (i.e., Pseudomonal dosing) Ticarcillin/Timentin® Ticarcillin has been shown to impair platelet function may prolong bleeding time but unclear whether this is clinically significant Carbapenems The most potent antibiotic in theβ-lactam class These agents should be used only when no other antibiotic options are available or appropriate Meropenem (Merrem®) Ertapenem (Invanz®) Imipenem/cilastin (Primaxin®) NF Doripenem (Doribax®) NF NF = non-formulary Carbapenems * Spectrum of activity Broadest coverage including Gm+, Gm- (especially drug resistant species -> see below and notes), anaerobic coverage All cover MSSA, Enterococcus (ampicillin sensitive)*, Streptococcus spp. Drugs of choice for ESBL* infections Good empiric coverage for Acinetobacter*, Citrobacter, Pseudomonas* *- except ertapenem See Notes Carbapenems * Differences in spectrum of activity Imipenem ≈ meropenem Meropenem usually has lower minimum inhibitory concentration (MIC) to Gm - pathogens not usually clinically significant Ertapenem Not clinically active vs. Enterococcus, Pseudomonas, Acinetobacter Not a good empiric choice for health care associated infections See Notes Carbapenems Differences in spectrum of activity: NF Doripenem Same coverage as meropenem/imipenem May be useful for highly multidrug-resistant organisms Lower MIC to certain pathogens in vitro Less likely to select for resistance in certain bacterial subpopulations At present, not much advantage over meropenem for most indications NF = non-formulary Carbapenems Clinical uses Severe intra-abdominal infections, heath careassociated infections* including pneumonia, ventilator-associated pneumonia, serious infections due to ESBL-producing organisms, meningitis** Use should be reserved for patients with risk factors for nosocomial/drug-resistant pathogens (see Zosyn® slide) * - except ertapenem; ** - meropenem only Carbapenems Side effects Hypersensitivity/allergic reactions Uncommon Low cross-reactivity in patients with penicillin allergy (see Module 3 of this series) Seizures Usually associated with imipenem and occurs in patients with poor renal function where dose not adjusted accordingly, previous seizure history may also predispose Carbapenems Drug interaction Valproic acid and meropenem decreases valproic acid levels (may apply with all carbapenems). Monitor valproic acid levels more frequently or use alternative antibiotic. Monobactams Aztreonam (only drug in class, Azactam®): Monocylic β-lactam ring (traditional β-lactams are bicyclic) i.e., structurally different Active against Gm - ONLY including Pseudomonas Gm – coverage similar to ceftazidime (they have structurally similar side chains) Side effects: rash Can be safely used in patients with Type I penicillin allergy Caution if patient has ceftazidime allergy (see Module 3) Currently on backorder; use only when no other options are available *Program Learning* 1. 2. 3. What is the drug of choice for ampicillin-sensitive Enterococcus? Besides the drug of choice, what other beta-lactam(s) would work? Which penicillins cover MRSA? What are the penicillins that would cover MSSA? *Program Learning Answers* 1. What is the drug of choice for ampicillin sensitive Enterococcus? Besides the drug of choice, what other beta-lactam(s) would work? Ampicillin is the drug of choice. Amoxicillin, penicillin, piperacillin, ticarcillin, imipenem, meropenem would also be appropriate choices. No cephalosporin covers Enterococcus. Ertapenem has variable activity. Aztreonam has no gm + coverage. *Program Learning Answers* 2. 3. Which penicillins cover MRSA? None. No β-lactam agent covers MRSA. What are the penicillins that would cover MSSA? Nafcillin, dicloxacillin, Zosyn®, Timentin®, Augmentin®, Unasyn®. If isolate is PCN-susceptible (this indicates that isolate does not produce penicillinase), then also can use penicillin, amoxicillin or ampicillin. *Program Learning Answers* A patient with resistant Pseudomonas aeruginosa wound infection has been on meropenem in-house and the MD plans to give ertapenem as a home IV infusion. His rationale is that ertapenem is a once daily medication as opposed to three times daily for meropenem. Is this appropriate? Why? *Program Learning Answers* Not appropriate because ertapenem does not cover Pseudomonas. The carbapenems with activity against Pseudomonas are imipenem, meropenem and doripenem. Cephalosporins These compounds are structurally related to the penicillins due to presence of β-lactam ring. This will only focus on cephalosporins used commonly in the inpatient setting 1st generation 2nd generation 3rd generation 4th generation Cephalosporins No cephalosporins cover Enterococcus No cephalosporins cover MRSA None are active versus ESBL-producing organisms All cephalosporins, including 3rd generation, are rendered inactive Cefepime still may be used for certain infections but should consult with ID clinician before using Cephalosporins 1st generation Cefazolin (Ancef®) Proteus, E. coli, Klebsiella (PEK), MSSA, Streptococcus spp. Better for Streptococcus spp. than nafcillin (cellulitis) Cephalexin (Keflex®), cefadroxil (Duricef®) Both with similar coverage to cefazolin Both are well absorbed orally Cefadroxil - less frequent dosing Cephalosporins 1st generation Uses Cefazolin Cellulitis, MSSA infections, surgical prophylaxis Cephalexin, cefadroxil UTI, skin/soft tissue infections due to MSSA or Strep spp. Cephalosporins 2nd generation Cefuroxime (PO/IV), cefaclor (PO) Coverage: PEK (see 1st generation slide) + Haemophilus, Neisseria = HNPEK More gram negative coverage, less Staph coverage Cephamycins (IV): cefotetan, cefoxitin Only cephalosporins that cover anaerobes Both active vs. B. fragilis be aware that resistance is increasing Used for pelvic inflammatory disease, surgical prophylaxis in ObGyn and colorectal surgery Cephalosporins * 3rd generation Ceftriaxone (Rocephin®), cefotaxime (IV only) HNPEK + Serratia = HNPEKS Not as reliable for Staph Good Pneumococcus activity, good meningeal penetration Multiple uses: UTI, SBP, meningitis, pneumonia Cefpodoxime, cefdinir, cefixime (all PO) Cefixime use should be reserved for treatment of STDs Cephalosporins 3rd generation Ceftriaxone Has numerous indications but only a few require doses higher than 1g: 2g IV q24h (endocarditis and osteomyelitis) 2g IV q12h (meningitis) No adjustment needed for renal dysfunction Cephalosporins 3rd generation Ceftazidime (Fortaz®) Coverage is broadened compared with others in 3rd generation to include Pseudomonas Only other cephalosporin which covers Pseudomonas is cefepime Not so good for Staphylococcus, Streptococcus Used for empiric treatment of febrile neutropenia, has decent meningeal penetration Cephalosporins 4th generation Cefepime (Maxipime®)NF Similar to ceftazidime, covers Pseudomonas and may be slightly more active vs. some Gm – organisms Better Gm + coverage than ceftazidime but still not as good as 1st generation cephalosporins Used in febrile neutropenia, health care-associated infections, meningitis May be used in certain infections/situations when treating ESBL infections consult ID clinician NF = non-formulary Cephalosporins Side effects Similar to penicillins Allergic reactions Blood dyscrasias Rare *Program Learning* 1. 2. Which cephalosporins do not need renal adjustment? How is ceftriaxone dosed for these disease states? 3. 4. Community-acquired pneumonia, endocarditis, osteomyelitis, meningitis Which cephalosporins have anaerobic coverage? Which cephalosporins cover Pseudomonas? *Program Learning Answers* 1. 2. Which cephalosporins do not need renal adjustment? Ceftriaxone only. All other cephalospsorins need to be adjusted for renal dysfunction. How is ceftriaxone dosed for these disease states? CAP: 1g iv q24h, Endocarditis/Osteomyelitis: 2g iv q24h, Meningitis: 2g iv q12h *Program Learning Answers* 3. 4. Which cephalosporins have anaerobic coverage? Cefoxitin and cefotetan; both are 2nd generation cephalosporins. Which cephalosporins cover Pseudomonas? Ceftazidime and cefepime. Fluoroquinolones These are potent antibiotics that have excellent oral bioavailability Ciprofloxacin Moxifloxacin LevofloxacinNF Trovafloxacin (off market - hepatotoxic) Gatifloxacin (off market - dysglycemias) NF = non-formulary Fluoroquinolones * Good options for certain disease states Used as second-line treatment for Tuberculosis (TB) Moxifloxacin in CAP If presenting with upper lobe pneumonia and TB suspected, do NOT give a quinolone Overuse has lead to increased resistance While the fluoroquinolones are potent antibiotics, bacteria have the capacity to rapidly develop resistance to these agents, especially under repeated exposure See Notes Fluoroquinolones Excellent oral bioavailability Use should be reserved for cases where other agents cannot be used i.e., patients with severe penicillin allergy If an isolate is resistant to one quinolone, consider it resistant to all quinolones Only drug in class with anaerobic activity is moxifloxacin Fluoroquinolones Ciprofloxacin Limited Gm+ activity Poor S. pneumoniae coverage Active against Enterobacteraciae, Pseudomonas Resistance rates will vary per institution, get an idea of antibiogram/susceptibilities at your area of practice Can be used for Enterococcus spp. UTIs If isolate susceptible, do not use for any other type of Enterococcus infection (i.e., bacteremia) Fluoroquinolones LevofloxacinNF S. pneumoniae coverage is better than ciprofloxacin but not as good as moxifloxacin Has activity versus Enterobacteriaciae, Pseudomonas Not much advantage over ciprofloxacin for most Gm - pathogens NF = non-formulary Fluoroquinolones Moxifloxacin Coverage: Most active fluoroquinolone for S. pneumoniae Excellent anaerobic coverage ->B. fragilis Similar Gram – activity compared to other fluoroquinolones but no activity vs. Pseudomonas Uses: Community-acquired pneumonia, intra-abdominal infections No need for renal adjustment Fluoroquinolones Drug interactions Divalent/trivalent containing products (Ca2+, Mg2+, Al3+, antacids) Can decrease oral absorption up to 90 percent, similar effect with tube feeds Concentration dependent antibiotics so need to treat interactions that bioavailability seriously Administer separately per manufacturer recommendation Fluoroquinolones Drug Interactions Warfarin Increased INR, risk of bleeding Cardiac meds Caution when used with other meds that can prolong QTc interval Consult package information for other interactions Fluoroquinolones Side effects CNS more common in elderly Interstitial nephritis Rare QTc prolongation Cartilage toxicity Precaution in very young and elderly N/V/D Most common side effect *Program Learning* 1. 2. A patient has been admitted for community-acquired pneumonia, placed on ceftriaxone and azithromycin, and is doing well. Upon discharge, which antibiotic would you recommend? A patient is admitted for suspected pneumonia from home. The chest X-ray shows right upper lobe lesion. Patient also has a three-week history of weight loss and night sweats and a history of + PPD test. What antibiotic class would you want to avoid and why? *Program Learning Answers* 1. The patient has been admitted for communityacquired pneumonia, placed on ceftriaxone and azithromycin, and is doing well. Upon discharge, which antibiotic would you recommend? Moxifloxacin. This is a recommended therapy in the CAP guidelines. *Program Learning Answers* 2. A patient is admitted for suspected pneumonia from home. The chest X-ray shows right upper lobe lesion. Patient also has a three-week history of weight loss and night sweats and a history of + PPD test. What antibiotic class would you want to avoid and why? Fluoroquinolones, especially newer generations like moxifloxacin. These have activity against TB and can potentially mask infection by partially treating it. Clindamycin Spectrum of activity S. aureus check sensitivities of isolate before using, Strep spp. Was once highly active against anaerobic gut bacteria but resistance has been increasing through the years Still has relatively good activity against oral flora anaerobic species No appreciable Gm - activity Clindamycin Role/clinical uses Used in combination with other antibiotics for necrotizing fasciitis to decrease toxin production from bacteria (Strep spp.) Ribosomal binding prevents production of destructive proteins Used in combination with other anaerobically active antibiotics for this disease state Clindamycin Role/clinical uses Still used frequently for dental infections, surgical prophylaxis Especially in patients with penicillin allergy Commonly used as prophylaxis/treatment in head and neck procedures Poorly GI tolerated, may predispose patients to C. difficile colitis Metronidazole Spectrum of activity Only covers anaerobic bacteria very little resistance, excellent activity Gram (+) and Gram (-) anaerobes Bacteriodes spp. Prevotella spp. Clostridium spp. (including C. difficile) Fusobacterium spp. Covers some parasitic organisms as well Metronidazole Used in C. difficile colitis Infections where anti-anaerobic coverage is desired or used in combination with other antibiotics which do not have anaerobic activity Surgical prophylaxis (colorectal, vaginal, abdominal) Bacterial vaginosis, trichomoniasis Metronidazole Treatment of C. difficile colitis Still first-line agent for uncomplicated, mildmoderate cases If severe case (definitions of severity may differ), PO vancomycin usually used IV metronidazole can be used to treat but not optimal (PO route will get highest concentration to area of infection) Metronidazole Drug interactions Warfarin Increased INRs, consider using PO vancomycin Lithium EtOH Disulfiram-like reaction with EtOH Side effects Metallic taste, dark urine Double Anaerobic Coverage * There is no need to add extra anaerobic coverage (in the form of clindamycin or metronidazole) to antibiotics with anaerobic coverage* There are consequences in gut colonization It is redundant and unnecessary * - Carbapenems, βL/βLi combos, moxifloxacin, tigecycline See Notes Double Anaerobic Coverage It may be appropriate to have double anaerobic coverage in these situations: Adding metronidazole to anaerobically active antibiotics for treatment of C. difficile diarrhea. Should be stopped promptly if C. difficile assay is negative Adding clindamycin to anaerobically active antibiotics for treatment of necroitzing fasciitis *Program Learning* 1. 2. 3. What is the spectrum of activity for clindamycin? A patient with Serratia bacteremia is started on clindamycin. What is wrong with this? A patient with hospital-acquired pneumonia, on Zosyn®, is started on metronidazole. Under what circumstance would this be appropriate? *Program Learning Answers* 1. 2. What is the spectrum of activity for clindamycin? Anaerobic bacteria, check sensitivities before using for either Staphylococci and Streptococci. A patient with Serratia bacteremia is started on clindamycin. What is wrong with this? Clindamycin has no appreciable Gm – activity. *Program Learning Answers* 3. A patient with hospital-acquired pneumonia, on Zosyn®, is started on metronidazole. Under what circumstance would this be appropriate? If patient has diarrhea and C. difficile is suspected (stool sample should be sent for C. difficile tests). Otherwise Zosyn® has excellent anaerobic activity. Vancomycin Inhibits cell wall synthesis, bactericidal. Crosses blood-brain barrier if inflamed. Spectrum: Gm + ONLY MRSA, Enterococcus, Coagulase Negative Staph spp., Strep spp. Clostridium difficile (when used via oral route). Vancomycin Delayed killing against S. aureus and MRSA especially with high inoculum size (in vitro). **If S. aureus isolate is β-lactam sensitive (i.e MSSA), use β-lactam antibiotic better killing, better outcomes. Vancomycin Still considered by many the drug of choice vs. MRSA but is a controversial issue. Issues with increasing Staph MICs, PK/PD issues, suboptimal clinical responses have all led to question vancomycin as first-line therapy. Newer drugs and new studies have also raised questions. Ongoing and controversial issue. Vancomycin Dosing and monitoring: Please see institutional protocol as dosing, frequency of monitoring and goal trough level ranges may differ between facilities. Review the recent consensus statement on vancomycin monitoring.* * - Rybak M, et al. 2009. Vancomycin Side effects Nephrotoxicity with other nephrotoxic drugs. Redman’s Syndrome This is an infusion-related reaction. Slow infusion rate if occurs (infuse over two hours); may use diphenhydramine for symptomatic relief. Blood dyscrasias Neutropenia, thrombocytopenia. Tend to be seen during longer treatment courses. Vancomycin Clinical uses Serious infections where MRSA is suspected. Therapy for Gm + infections in patients with serious allergic reactions to β-lactam antibiotics. Treatment for C. difficile colitis (given PO). Systemic infections cannot be treated with vancomycin PO localized to gut. Vancomycin Clinical uses If initial cultures do not show MRSA, prescriber should be contacted to review appropriateness If not indicated, vancomycin should be discontinued as quickly as possible to avoid: pressure for the development of VRE or selection of other resistance potential toxicities unnecessary use of powerful antibiotic *Program Learning* 1. 2. 3. Patient with MSSA leg infection on vancomycin IV. Patient has no allergies. Is there a better antibiotic? True/false. Vancomycin is bactericidal. An order is written to use high-dose PO vancomycin to treat a MRSA cellulitis. Is this appropriate? *Program Learning Answers* 1. 2. Patient with MSSA leg infection on vancomycin IV. Patient has no allergies. Is there a better antibiotic? Yes. The β-lactams have better killing activity vs. MSSA than vancomycin. Nafcillin, dicloxacillin and cephalexin are potential options. True/False. Vancomycin is bactericidal. TRUE *Program Learning Answers* 3. An order is written to use high-dose vancomycin given via oral route to treat a MRSA cellulitis. Is this appropriate? Vancomycin given PO is only effective against C. difficile and is localized almost exclusively to the GI tract. Conversely, IV vancomycin will not treat C. difficile. References Chambers, H. Chapter 21: Penicillins and β- Lactam Inhibitors. Mandell, G., Bennett, J., Dolin, D. Mandell, Douglas and Bennett’s Principles and Practice of Infectious Disease. 7th Edition. 2009. Andes, D., Craig, W. Chapter 22: Cephalosporins. Mandell, G., Bennett, J., Dolin, D. Mandell, Douglas and Bennett’s Principles and Practice of Infectious Disease. 7th Edition. 2009. Siu, LK. et al. Correlation of in vitro susceptibility testing results for amoxicillinclavulanate and ampicillin-sulbactam using a panel of beta-lactamase producing Enterobacteriaceae. APMIS. 1998 Sep; 106(9):917-20. Kacmaz, B., Sultan, N. In vitro susceptibilities of Escherichia coli and Klebsiella spp. to ampicillin-sulbactam and amoxicillin-clavulanic acid. Jpn J Infect Dis. 2007 Jul;60(4):227-9. Piperacillin. Drug Monograph. In: Klasco RK (Ed): DRUGDEX® System (electronic version). Thomson Micromedex, Greenwood Village, Colorado, USA. Available at: http://www.thomsonhc.com (cited:10/12/2009). Piperacillin/tazobactam (Zosyn®). Drug Monograph. In: Klasco RK (Ed): DRUGDEX® System (electronic version). Thomson Micromedex, Greenwood Village, Colorado, USA. Available at: http://www.thomsonhc.com (cited:10/12/2009). References Ticarcillin/clavulanic acid (Timentin®). Drug Monograph. In: Klasco RK (Ed): DRUGDEX® System (electronic version). Thomson Micromedex, Greenwood Village, Colorado, USA. Available at: http://www.thomsonhc.com (cited:10/12/2009). Aztreonam. Drug Monograph. In: Klasco RK (Ed): DRUGDEX® System (electronic version). Thomson Micromedex, Greenwood Village, Colorado, USA. Available at: http://www.thomsonhc.com (cited:10/12/2009). Reichardt, P. et al. Leukocytopenia, thrombocytopenia and fever related to piperacillin/tazobactam treatment—a retrospective analysis in 38 children with cystic fibrosis. Infection. 1999 Nov-Dec;27(6):355-6. Kaiser Regional Antibiogram, Northern California. 2009 American Thoracic Society; Infectious Disease Society of America. Guidelines for the management of adults with hosptial-acquired, ventilator-associated and healthcare-associated pneumonia. Am J Respir Crit Care Med. Vol 171. pp 388-416, 2005. Chambers, H. Chapter 23: Carbapenems and monobactams. Mandell, G., Bennett, J., Dolin, D. Mandell, Douglas and Bennett’s Principles and Practice of Infectious Disease. 7th Edition. 2009. References Paterson, D., Depestel D. Doripenem. Clin Infect Dis. 2009 Jul 15;49(2):291-8. Spriet, I. Interaction between valproate and meropenem: a retrospective study. Ann Pharmacother. 2007 Jul;41(7):1130-6. ASHP Drug Product Shortages Management Resource Center. www.ashp.org/drugshortages/current. Last accessed 10/12/2009. Ramphal, R., Ambrose, P. Extended-spectrum beta-lactamases and clinical outcomes: current data. Clin Infect Dis. 2006 Apr 15;42 Suppl 4:S164-72. Long, R. et al. Empirical treatment of community-acquired pneumonia and the development of fluoroquinolone-resistant tuberculosis. Clin Infect Dis. 2009; 48:1354-60. Moxfloxacin. Drug Monograph. In: Klasco RK (Ed): DRUGDEX® System (electronic version). Thomson Micromedex, Greenwood Village, Colorado, USA. Available at: http://www.thomsonhc.com (cited:10/12/2009). Clindamycin. Drug Monograph. In: Klasco RK (Ed): DRUGDEX® System (electronic version). Thomson Micromedex, Greenwood Village, Colorado, USA. Available at: http://www.thomsonhc.com (cited:10/12/2009). References Rybak, M. et al. Therapeutic monitoring of vancomycin in adult patients: A consensus review of the American Society of Health-System pharmacists, the Infectious Diseases Society of America and the Society of Infectious Diseases Pharmacists. Am J Health-System Pharm. 2009;66:82-98. Donskey, et al. Effect of antibiotic therapy on the density of vancomycin-resistant enterococci in the stool of colonized patients.NEJM. 2000 Dec 28;343(26):1925-32. Murray, B., Esteban, N. Chapter 31: Glycopeptides (Vancomycin and teicolanin), Streptogramins (Quinupristin-dalfoprsitin), and lipopeptides (daptomycin). Mandell, G., Bennett, J., Dolin, D. Mandell, Douglas and Bennett’s Principles and Practice of Infectious Disease. 7th Edition. 2009. Hooper, D., Strahilevitz, J. Chapter 35: Quinolones. Mandell, G., Bennett, J., Dolin, D. Mandell, Douglas and Bennett’s Principles and Practice of Infectious Disease. 7th Edition. 2009. Metronidazole. Drug Monograph. In: Klasco RK (Ed): DRUGDEX® System (electronic version). Thomson Micromedex, Greenwood Village, Colorado, USA. Available at: http://www.thomsonhc.com (cited:10/12/2009). Gerding, D. et al. Treatment of Clostridium difficie infection. Clin Infect Dis. 2008 Jan 15;46 Suppl1:S32-42. . This concludes Module 2: Antibiotic Review. Please proceed to Module 3: Allergy Review.