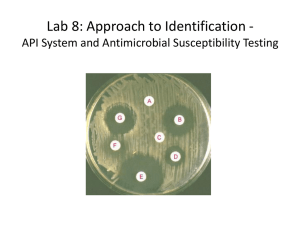
C - World Health Organization
advertisement

Antimicrobial resistance Antimicrobial resistance and susceptibility testing May 2007 P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E Learning objectives At the end of the presentation, participants should: • Identify antimicrobial susceptibility testing needs • Understand standard antimicrobial susceptibility testing • Interpret antimicrobial susceptibility testing P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E Leading global infectious diseases S. pneumonia: Up to 55% S. dyentariae: 90% resistance to cotrimoxazole S.Typhi: Outbreaks of resistance to penicillin in some regions HIV: Report of resistance to all marketed agents 4 Millions of deaths, worldwide, 1998 multi-resistant strains in 11 countries M. tuberculosis: Multi-drug resistant tuberculosis 3 P. falciparum: Chloroquine resistance in 81/92 countries 2 1 0 Respiratory infections HIV Diarrheal diseases P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists Tuberculosis A N D R E S P O N S E Malaria Antibiotic resistant infections Diseases Agent Resistances Pneumonia S pneumoniae Penicillin Dysentery S dysenteriae Multiple resistances Typhoid S typhi Multiple resistances Gonorrhea N gonorrhoeae Penicillin and tetracycline Tuberculosis M tuberculosis Rifampicine and INH Nosocomial infections S aureus Methicillin, vancomycin E species Vancomycin Klebsiella, Pseudomonas Multiple resistances P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E Antimicrobial resistance Results from misuse, overuse, under/ inadequate use of antimicrobials • Costs money, lives and undermines effectiveness of health delivery programs • Threat to global stability and national security WHO Global Strategy for Containment of Antimicrobial Resistance: • Intervention framework to slow emergence and reduce the spread of antimicrobial resistant microorganisms P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E Natural & acquired resistance Natural resistance • Chromosomic genetic support • Affect almost all species strains • Existed before antibiotic use (Enterobacter sp. - amoxicillin) Acquired resistance (mutation) • Chromosomic, plasmidic or transposon genetic support • Affects a fraction of strains • Increased with antibiotic use (extended spectrum beta-lactamase producing E. coli) P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E Different acquired resistances Acquired to a population of strains in a given species • Extremely frequent in nosocomial infections Acquired under treatment; specific strain,specific patient • Relatively uncommon except for certain species (e.g., Enterobacter, Pseudomonas, Mycobacterium) P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E Mechanisms of resistance Prevent antibiotic from reaching its target • Impaired cell membrane permeability • Efflux phenomenon Prevent the antibiotic from biding to its target • Supplementary targets • Decreased affinity by target modification Inactivation before reaching the target P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E Genetic exchange of antimicrobial resistance genes Staphylococci Pseudomonas Enterococci Enterobacteriaceae Vibrio cholerae Pneumococci Campylobacter P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists Streptococci A N D R E S P O N S E Antimicrobial susceptibility tests Minimum inhibitory concentration [MIC] • The smallest concentration of antibiotic that inhibits the growth of organism Liquid media (dilution) allows MIC estimation Solid media (diffusion) • Disk diffusion (Kirby-Bauer) • E-tests • Allows MIC estimation Beta lactamase production: quick screening method P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E Dilution in liquid broth • Tubes containing increasing antibiotic concentrations • Incubation during 18 hr at 37°C • Tedious MIC Bacterial growth 0 (Control) 0,25 0,50 1 P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists 2 A N D Inhibition 4 R E S P O N S E 8 mg/l Kirby-Bauer disc testing Antibiotic-impregnated discs placed on an agar plate at the interface between test organism and susceptible control organism Resulting zones of inhibition compared, use of controls Susceptibility is inferred (standard tables) P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E E-test Plastic strips with a predefined gradient of • One antibiotic • One antifungal Only one manufacturer One strip per antibiotic Wide range of antibiotics Easy to use Storage at -20°C Short shelf life, expensive P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E Reading E-tests Ciprofloxacin for Yersinia pestis Resistant > 4 ug/ml Intermediate 1-4 ug/ml Susceptible < 1 Upper reading P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E Antimicrobial susceptibility tests Antimicrobial susceptibility testing is expensive (costs include all supplies) Kirby-Bauer • 12 discs panel = $1.35 E-test (Performed only in certain situations) • One strip = $2.50 P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E Different standards Use standardized reference National Committee for Clinical Laboratory Standards (USA) Other norms • Canadian • Chinese • National Do not confuse the different tables Choose one for everything P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E Critical points in quality assurance 1. Culture media: Muller-Hinton 2. Reagents: disks 3. Size of the inoculums 4. Incubation condition 5. Control with reference strains 6. Reading inhibition diameters (accurate measurement) 7. Knowledge of staff P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E Standard strains for quality assurance Precision and accuracy ensured through control strains • Known susceptibility to antimicrobial agents Standard strains include • Staplylococcus aureus ATCC 25923 • Escherichia coli ATCC 25922 • Pseudomonas aeruginosa ATCC 27853 P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E Interpretation The main concept is the “clinical categorisation" • Strains are sorted according to level of Minimal Inhibitory Concentration (MIC) versus reference breakpoints • c and C are the minor and major breakpoints Susceptible MIC < Intermediate c ≤ MIC < P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D Resistant C R E S P O N S E ≤ MIC Understanding breakpoints Words of laboratory specialists • It is not possible to work alone • Breakpoints are the expression of a consensus among the scientific community at a given time in a country Breakpoints are determined using two approaches • Pharmacological concept • Epidemiological concept P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E The epidemiological concept for breakpoints Inherited resistance mechanism Wild type 60 50 40 30 20 10 0 0.01 0.03 0.06 0.12 0.25 0.5 c P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists 1 2 A N D 4 C 8 R E S P O N S E 16 32 64 128 MIC The pharmacological concept for breakpoints The concentration range tested for a drug and the interpretative criteria for various categories are based on extensive studies that correlate with • Serum achievable levels for each antimicrobial agent • Particular resistance mechanisms • Successful therapeutic outcome In practice situations the entire range may not be used for decision making and therefore the concept of breakpoint concentration P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E From breakpoints to interpretation MIC ≤ c Sensitive strain MIC > C Intermediate strain c < MIC ≤ C Resistant strain Measuring antimicrobial sensitivity of a strain isolated from a patient, to determine its status as S, I or R is an individual problem Defining the status of a bacterial species or genus is an epidemiological problem distributed across time and space that requires monitoring P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E Host factors affecting treatment Diffusion in tissues Serum protein binding Drug interactions Immune system Multiple simultaneous infections Virulence of organism Site and severity of infection P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E Interpreting intermediate resistance Sometime the agent can still be used • Higher doses required to ensure efficacy • Agent may be efficacious if concentrated in vivo in an infected body fluid (e.g., urine) Sometimes there is uncertainty • Intermediate resistance may represent a “buffer” zone that prevents strains with borderline susceptibility from being incorrectly categorized as resistant P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E Common interpretation problems Results depends on the technique used Many factors influence results • Lack of standardization of the inoculums • Thickness and quality of the culture media • Quality and conservation of the disks • Wuality control with standardized strains • Condition and duration of incubation P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E Common interpretation problems An agar gel that is too thick leads to smaller zones Source: http://www.who.int/csr/resources/publications/drugresist/WHO_CDS_CSR_RMD_2003_6/en/ P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E Common interpretation problems Problem with the size of the inoculums Solution: • Use McFarland 0.5 photometer • Scale -> same tubes P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E Common interpretation problems Contamination with another organism P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E Common interpretation problems Bad manipulation Inoculation of the Muller Hinton • Swabbing • Not by flooding P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E Common interpretation problems Problems with E-test reading P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E Cost of anti-microbial resistance Cheap antimicrobials become ineffective Individual treatment failure Prolonged illness, hospitalization Need to switch to more expensive, complex drugs that are often not even available in resource-poor settings Need to develop new antimicrobials Good antimicrobial susceptibility testing saves lives and money P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E WHO/CDS/CSR/APH/2000.4 Distr. : General English only WHO Global Principles For The Containment of Antimicrobial Resistance In Animals Intended for Food Report of a WHO Consultation with the participation of the Food and Agriulture Organization and the Office International des Epizooties Geneva, Switzerland 5 – 9 June 2000 Department for Communicable Diseases Surveillance and Response World Health Organization P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E Antimicrobial resistance Developed by the Department of Epidemic and Pandemic Alert and Response of the World Health Organization with assistance from: European Program for Intervention Epidemiology Training Canadian Field Epidemiology Program Thailand Ministry of Health Institut Pasteur P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E References • Manual for the laboratory Identification and Antimicrobial Susceptibility Testing of Bacterial Pathogens of Public Health Importance in the Developing World WHO/CDS/CSR/RMD/2003.6 http://www.who.int/csr/resources/publications/drugresi st/WHO_CDS_CSR_RMD_2003_6/en/ P I D E M I C A L E R T Laboratory Training for FieldEEpidemiologists A N D R E S P O N S E