Antiepileptic Drugs Types of Seizures Partial/Focal
advertisement

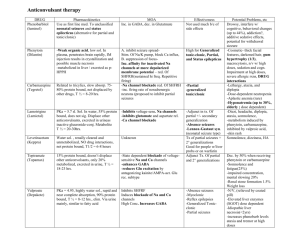
Antiepileptic Drugs Types of Seizures Generalized Seizure Partial/Focal Seizure Simple Partial Seizure – conciousness is not Absence/Petit mal Seizure impaired With motor signs With sensory symptoms With autonomic symptoms & signs With psychic symptoms Complex Partial/Temporal lobe/Psychomotor Seizure – loss of Myoclonic Seizure conciousness Simple partial onset followed concious impairment Concious impairment at the onset Partial seizures evolving to secondarily generalized seizures Simple partial seizures evolving to generalized seizures Complex partial seizures evolving to generalized seizures Simple partial seizures evolving to complex partial seizures evolving to generalized seizures Involve an interruption to consciousness where the person experiencing the seizure seems to become vacant and unresponsive for a short period of time (usually up to 30 seconds) Slight muscle twitching may occur Involve an extremely brief (< 0.1 second) muscle contraction Result in jerky movements of muscles or muscle groups Tonic Seizure Myoclonus that are regularly repeating at a rate typically of 2-3 per second In some cases, the length varies. Tonic-clonic/Gran Mal Seizure Involve an initial contraction of the muscles (tonic phase) which may involve o Tongue biting o Urinary incontinence o Absence of breathing This is followed by rhythmic muscle contractions (clonic phase) Atonic Seizures Involve the loss of muscle tone, causing the person to fall to the ground Continous Seizure Status Epilepticus Refers to continuous seizure activity with no recovery between successive seizures When the seizures are convulsive, it is a lifethreatening A tonic-clonic seizure lasting longer than 5 minutes is usually considered grounds for calling the emergency services. Epilepsia Partialis Continua Rare type of focal motor seizure (hands and face) Recurs every few seconds or minutes for extended periods (days or years) It is usually due to o Strokes in adults o Focal cortical inflammatory processes in children (Rasmussen's encephalitis) The major mechanism of actions of antiepileptic drugs are 1. Enhancement of GABAergic inhibitory transmission 2. Inhibition of excitatory (glutamatergic) transmission 3. Modification of ionic conductance Classification of Antiepileptic drugs 1. Based on Mechanism of Actions a. Drugs that inhibit Na+ influx by inhibiting Na+ voltage channels i. Phenytoin ii. Carbamazepine iii. Valproic acid iv. Lamotrigine v. Lacosamide b. Drugs that inhibit Glutamatergic receptors i. Felbamate c. Drugs that augment the GABAergic inhibitory transmission i. Phenobarbital ii. Benzodiazepine iii. Tiagabine iv. Vigabatrin d. T-type Ca2+ channels blockers i. Ethosuximide ii. Valproic acid e. Mixed group i. Levetiracetam ii. Topiramate iii. Valproic acid iv. Phenobarbital 2. Based on Clinical Usage a. Drugs used in partial seizures and tonic-clonic generalized seizures i. Older Generation 1. Cyclic Ureides a. Phenytoin b. Primidone c. Phenobarbital d. Ethosuximide 2. Carbamazepines 3. Valproic acid ii. Newer Generation 1. Lamotrigine 2. Levetiracetam 3. Gabapentin 4. Topiramate 5. Vigabatrin 6. Lacosamide b. Drugs used in generalized seizures i. Ethosuximide ii. Valproate acid Regimen of Antiepileptic Therapy 1. Partial Seizures a. Carbamazepine (OR) b. Phenytoin 2. Generalized Seizures a. Carbamazepine (OR) b. Phenytoin 3. Secondary Generalized Seizure a. Carbamazepine 4. Absence Seizures a. Ethosuximide 5. Myoclonic Seizure a. Valproate acid Drugs Phenytoin Have narrow therapeutic index Elimination Pattern Dose dependent Pattern of elimination o Very low blood level Follows first order elimination o Therapeutic blood level Max capacity of hepatic metabolism has reached o Slightly higher level than that of therapeutic’s Follows zero order elimination Slight ↑ in dose may markedly ↑phenytoin level Half life o Once followed the zero order elimination, half life is unpredictable (↑disorderly) o Leads to Steady state concentration cant be achieved in routine fashion Pts quickly develops toxicity Mechanism of Action Pharmacokinetics Absorption Readily absorp orally (depends on formulation) Absorption after IM admin is unpredictable o Accumulation of Phenytoin in skeletal muscle may occur o Therefore, this route of admin should be avoided Distribution Highly plasma protein binding Accumulate in o Brain o Liver o Muscle o Fat Metabolism Undergoes CYP450 hepatic metabolism Shows to be CYP450 inducer Excretion Excreted through urine Some in unchanged form Blocks the activated state of Na+ voltage channels o Leads to the blockade of high frequency firing of neurons ↓synaptic release of Glutamate Clinical Indication 1. Generalized tonic-clonic/ Gran mal seizure 2. Partial seizures Should not be given in Absence seizures It may exacerbate the condition Drug Interactions o o o o Adverse Effects Phenytoin is highly plasma protein binding Other highly plasma protein bound drugs may displace phenytoin Phenylbutazone Sulfonamides Displacement of phenytoin may result in ↓total plasma phenytoin level ↑free plasma phenytoin ↑toxicity ↓plasma protein binding in Hypoalbumineamia Renal failure Hepatic disease Has affinity to Thyroid Binding Globulin May interfere the reading during thyroid function test Nystagmus (involuntary movement of eyes) Diplopia (double vision) Ataxia (loss of coordination and muscle movement) Gingivial hyperplasia o Happens in poor oral hygiene Hirsutism Neuropathy Contraindication Pregnancy May lead to o Fetal Hydantoin Syndrome Spina bifida Drugs Carbamazepine Available only in oral form Contraindication Pregnancy Mechanism of Action Pharmacokinetics Absorption Readily absorp orally Complete absorption in all pts Becomes slower if taken by food o Beneficial in pts taking higher daily dose as to tolerate side effects Distribution Peak concentration achieved after 6-8 hours Low volume of distribution 70% bound to plasma protein o Other drugs do not show any displacement of carbamazepine Blocks the inactivated state of Na+ voltage channels o Leads to the blockade of high frequency firing of neurons ↓synaptic release of Glutamate Clinical Indication Generalized tonic-clonic/ Gran mal seizure Partial seizures Should not be given in Absence seizures It may exacerbate the condition Drug Interactions Carbamazepine is a CYP450 enzyme inducer Carbmazepine may induce metabolism of o Phenytoin o Ethosuximide o Valproic acid o Clonazepam Metabolism Undergoes CYP450 hepatic Metabolism of carbamazepine can be inhibited (leads to ↑serum level) if given metabolism with o Carbamazepine-10,11o Valproic acid epoxide seems to have Metabolism of carbamazepine can be anticonvulsant activity induced (leads to ↓serum level) if given Shows to be CYP450 inducer with o Phenobarbital Excretion o Phenytoin Excreted through urine Adverse Effects Diplopia Ataxia GIT upsets Hyponatreamia Water intoxification Aplastic anemia Agranulocytosis Drugs Valproic Acid Contraindication Pregnancy May cause o Spina bifida o Cardiovascular anomalies o Orofacial anomalies o Digital anomalies Mechanism of Action Pharmacokinetics Absorption Readily absorp orally Bioavailibility up to 80% Will be ionized upon entering the blood circulation Distribution Highly plasma protein binding of up to 90% Accumulate in o Extracellular water cause couldn’t pass the plasma membrane Metabolism Undergoes CYP450 hepatic metabolism Excretion Excreted through urine Some in unchanged form Blocks the inactivated state of Na+ voltage channels o Leads to the blockade of high frequency firing of neurons Blocks the NMDA receptors ↑GABA level in the brain o ↑activity of Glutamic Acid Decarboxylase (GAD) o ↑GABAergic inhibitory transmission Clinical Indication Generalized tonic-clonic/ Gran mal seizure Partial seizures Generalized seizures Absence seizures Myoclonic seizures Drugs Interaction Displace phenytoin from plasma protein Inhibits metabolism of o Phenobarbital o Phenytoin o Carbamazepine Adverse Effects GIT upset Fine tremor Weight gain Alopecia Increase in appetite Hepatotoxicity Thrombocytopenia Drugs Felbamate Ethoxusimide Phenobarbital Mechanism of Action Pharmacokinetics Absorption Readily absorp orally Metabolism Undergoes CYP450 hepatic metabolism Excretion Excreted through urine Absorption Complete absorption following oral admin Distribution Does not bound to plasma protein Metabolism Metabolizes through hydroxylation Long half life of 40hours Excretion Excreted through urine Absorption Complete absorption following oral admin Distribution Does not bound to plasma protein Metabolism Metabolize though liver No active metabolite Excretion Excreted through urine Clinical Indication Block of NMDA receptors ↑GABAA receptor responses ↓the lowthreshold current of Ca2+ T-type channels This channels are located at the Thalamus o Responsible for generation of rhythmic cortical discharge in absence seizure ↑phasic GABAA phasic receptor responses ↓excitatory synaptic responses Adverse Effects Partial seizures Generalized seizures associated with LennoxGastaut syndrome in children Absence seizures o o o Aplastic anemia Severe hepatitis Generalized tonic-clonic/ Gran mal seizure Partial seizures Generalized seizures Neonatal seizures Status epilepticus Sedation Cognitive problems Ataxia Hyperactivity Gastric distress Pain Nausea Vomitting Fatigue Headache Dizziness Hiccup Euphoria Drugs Diazepam Benzodiazepine Mechanism of Action Pharmacokinetics Absorption Readily absorp orally Rectal admin gives peak concentration within 1hour Distribution 90% of bioavailibilty Metabolism Metabolize though liver Produce numerous active metabolites Excretion Excreted through urine Absorption Readily absorp orally Distribution 80% bioavailibility Metabolism Metabolize though Clonazepam liver extensively No active metabolite Excretion Excreted through urine ↑phasic GABAA phasic receptor responses Clinical Indication Status epilepticus Absence seizures Myoclonic seizure Infantile spasm Adverse Effects Sedation Drugs Topiramate Lamotrigine Mechanism of Action Pharmacokinetics Absorption Readily absorp orally Distribution Not bound to plasma protein Metabolism Metabolize though liver extensively No active metabolite Excretion Excreted through urine 40% excreted unchanged Absorption Readily absorp orally Distribution Not bound to plasma protein Metabolism Metabolize though liver extensively No active metabolite Excretion Excreted through urine Clinical Indication Blocks the activated state of Na+ voltage channels o Leads to the blockade of high frequency firing of neurons ↑GABAA receptor responses ↓excitatory synaptic responses Prolong inactivation of Na+ voltage channels Blocks presynaptic Ca2+ voltage channels ↓release of Glutamate Adverse Effects Generalized tonicclonic/ Gran mal seizure Partial seizures Generalized seizures Absence seizures Migraine Sedation Cognitive slowing Confusion Paraesthesia Generalized tonicclonic/ Gran mal seizure Partial seizures Generalized seizures Absence seizures Myoclonic seizures Dizziness Headache Diplopia Rash