Mechanical
Ventilation
Alfred E. Baylor, III, MD
Critical Care Fellow
March 18, 2015
Objectives
• To review the indications for standard
mechanical ventilation
• To evaluate the need to escalate therapy to
rescue modes
• To identify the importance of PEEP and prone
position.
• To describe newer modes of ventilation
Indications for MV
• Failure- to adequately oxygenate, ventilate or
meet the metabolic demands of a
physiologically stressed patient.
Physiologic Mechanism
Clinical Assessment Normal Range
Need for MV
Hypoxemia
P(A-a) O2 (mm Hg)
PaO2/FiO2 ratio
SaO2
25-65
425-475
98%
>350
<300
< 90% despite O2
Hypercarbia/inadequate
alveolar ventilation
PaCO2
35-45 mmHg
Acute increase from
pt’s baseline
pH < 7.20
Δ Mental status
Oxygen delivery/oxygen
consumption imbalance
Elevated lactate
≤2.2 mg/dl
Decreased mixed
venous oxygen sat
70%
≥4 mg/dl despite
adequate resus
<70% despite
adequate resus
Increased work of breathing Minute ventilation
(WOB)
Dead space
5-10 L/min
0.15-0.30
>15-20 L/min
≥0.5 (acute)
Inspiratory muscle
weakness
NIP
VC
80-100 cm H2O
60-75 ml/kg
< 20-30
<15-20 ml/kg
Acute decompensated
heart failure
JVD, Pulm edema,
Decreased EF
Inadequate lung expansion
VT (ml/kg)
VC (ml/kg)
RR
Clinical judgement
5-8
60-75
12-20
<4-5
<10-15
≥35
Ventilator Mode
Trigger
Control
Cycling
Inspiratory flow
Continuous
Mandatory
Ventilation
(CMV)
Patient
or time
Flow or pressure
Volume or time
Selected or
decelerating
Volume
control/assist
control (VC/AC)
Patient
or time
Flow
Volume
Square,
decelerating, or
sinusoidal
Pressure
control/assist
control (PC/AC)
Patient
or time
Pressure
Time
Decelerating
Synchronized
intermittent
mandatory
ventilation
(SIMV)
Patient
or time
Pressure for
patient breaths
Flow(VC) or
pressure (PC) for
ventilator
breaths
Flow
(spontaneous)
Volume
(ventilator)
Decelerating
(spontaneous)
Square (VC),
decelerating (VC
or PC), sinusoidal
(spontaneous)
Stand-alone
pressure-support
ventilation (PSV)
Patient
None
Flow
Decelerating
Initial Ventilator Modes
• Volume-cycled breath- preset tidal volume
(VT), excessive airway pressures
• Time-cycled breath- pressure-controlled (PC)
breath, constant pressure for preset time,
minute ventilation not guaranteed b/c fxn of
compliance/resistance
• Flow-cycled breath- pressure support (PS)
breath, constant pressure during inspiration
Spontaneous
breath
Assist volume
control
Assist pressure control
and pressure-regulated
volume control
Pressure
Flow
Volume
Joseph Parrillo and R. Phillip Dellinger CCM 4th Edition 2014: 138- 177
Pressure
support
ventilation
Joseph Parrillo and R. Phillip Dellinger CCM 4th Edition 2014: 138- 177
Requirements
•
•
•
•
•
CXR
Vitals
SpO2
Patient-vent synchrony
ABG
• Inspiratory pressures
(Ppeak, Pplateau)
• Inspiratory:Expiratory
ratio (1:2)
• Auto-PEEP
• Vent alarms
• End tidal CO2
(EtCO2/PaCO2, ≤
5mmHg)
Inspiratory Pressures
• Ppeak- Peak Inspiratory pressure (Airway
resistance + Elastic recoil of lungs + chest wall)
• Pplat- Inspiratory plateau pressure (≤ 30 cm H20)
(Elastic recoil of lungs + chest wall)
• I/E ratio- I time with volume ventilation
-VT( Larger VT, longer time)-Inadequate E
-Inspiratory flow rate
-Incomplete
exhalation
-Inspiratory waveform
-Breath stacking
Auto-PEEP
Joseph Parrillo and R. Phillip Dellinger CCM 4th Edition 2014: 138- 177
Mode
Advantage(s)
Disadvantage(s)
Continuous
Mandatory
Ventilation (CMV
Rests muscles of
respiration
Requires use of heavy
sedation/neuromuscular
blockade
Assist volume control (AVC)
Reduced work of breathing
Guarantees delivery of set
tidal volume (unless peak
pressure limit alarms)
Potential adverse HD
effects
May lead to inappropriate
hyperventilation and
excessive inspiration
pressures
Assist pressure control (APC)
Allows limitation of Pp
Same as above
Potential hyperventilation
or hypoventilation with
lung resistance/compliance
changes
Synchronized intermittent
mandatory ventilation (SIMV)
Less interference with
normal cardiovascular fxn
Increased work of
breathing vs. AC
Synchrony issues
Stand-alone pressure-support
ventilation (PSV)
Patient comfort
Improved patientventilator interaction
Joseph Parrillo and R. Phillip Dellinger CCM 4th Edition 2014: 138- 177
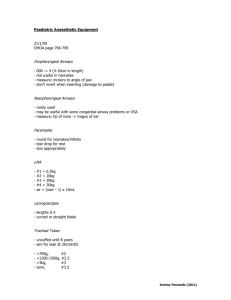
Pressure-volume curves comparing ventilation regions with high-frequency oscillatory
ventilation (HFOV) and airway pressure-release ventilation (APRV).
Stephen R Collins, and Randal S Blank Respir Care
2011;56:1573-1582
(c) 2012 by Daedalus Enterprises, Inc.
Volume Controlled Versus Pressure Controlled Ventilation.
Dean R Hess Respir Care 2011;56:1555-1572
(c) 2012 by Daedalus Enterprises, Inc.
From: Acute Respiratory Distress Syndrome: The Berlin Definition
JAMA. 2012;307(23):2526-2533. doi:10.1001/jama.2012.5669
Date of download: 3/10/2015
Copyright © 2015 American Medical
Association. All rights reserved.
From: Acute Respiratory Distress Syndrome: The Berlin Definition
JAMA. 2012;307(23):2526-2533. doi:10.1001/jama.2012.5669
Date of download: 3/10/2015
Copyright © 2015 American Medical
Association. All rights reserved.
From: Acute Respiratory Distress Syndrome: The Berlin Definition
JAMA. 2012;307(23):2526-2533. doi:10.1001/jama.2012.5669
Date of download: 3/10/2015
Copyright © 2015 American Medical
Association. All rights reserved.
From: Acute Respiratory Distress Syndrome: The Berlin Definition
JAMA. 2012;307(23):2526-2533. doi:10.1001/jama.2012.5669
Date of download: 3/10/2015
Copyright © 2015 American Medical
Association. All rights reserved.
ECMO
Inhaled NO
HFOV
Increasing Intensity of Intervention
Prone Positioning
Lower Tidal Volume/Pplat +ECCO2R
Neuromuscular Blockade
Higher PEEP
Low-Moderate PEEP
Low Tidal Volume Ventilation
Mild ARDS
300
250
Moderate ARDS
200
The ARDS Definition Taskforce. JAMA 2012;307:2526-2533
150
PaO2/FiO2
Severe ARDS
100
50
0
Ventilator Settings for ALI/ARDS.
(c) 2012 by Daedalus Enterprises, Inc.
Dean R Hess Respir Care 2011;56:1555-1572
Stress and strain
• Stress – transpulmonary pressure (Δ PL=ΔPaw x
EL/Etot or when the force that distends the
lung is the pressure difference between alveoli
and pleural cavity. (want ≤20 cmH2O)
• Strain – linear deformation of material or
ΔV/V0 (volume change or VT/lung resting vol or
FRC at atm pressure no PEEP (want ≤ 1.5-2)
• PL (stress)=Espec(lung elastance) x ΔV/V0(strain)
Effect of a stiff chest wall on transpulmonary pressure.
Dean R Hess Respir Care 2011;56:1555-1572
(c) 2012 by Daedalus Enterprises, Inc.
Methods for Selecting PEEP.
Dean R Hess Respir Care 2011;56:1555-1572
(c) 2012 by Daedalus Enterprises, Inc.
Meta-analyses of Studies That Compared Higher Versus Lower PEEP.
Dean R Hess Respir Care 2011;56:1555-1572
(c) 2012 by Daedalus Enterprises, Inc.
Potential effects of an increase in PEEP. If the potential for recruitment is low, an increase in
PEEP results in a large increase in plateau pressure (Pplat) (increased driving pressure), to
an unsafe level.
Dean R Hess Respir Care 2011;56:1555-1572
(c) 2012 by Daedalus Enterprises, Inc.
Recruitment measures
• Varies (30-40 cmH2O for 30-40 sec, 5-20 cm H2O
up to 20 min)
• Sedation, +/- paralysis required
• At each PEEP level maintain VT, RR, FiO2, I:E ratio
• measure ABG( improve 2/3)
1. arterial oxygenation
2. Resp. system compliance
3. Alveolar Dead Space
Approaches to Patient-Ventilator Asynchrony.
(c) 2012 by Daedalus Enterprises, Inc.
Dean R Hess Respir Care 2011;56:1555-1572
Comparison of Conventional Ventilation, Inverse Ratio Ventilation, Biphasic Positive Airway
Pressure, Airway Pressure Release Ventilation, and High-Frequency Oscillatory Ventilation.
Daoud, E. G. et al. Respir Care 2012;57:282-292
(c) 2012 by Daedalus Enterprises, Inc.
ECMO
Inhaled NO
HFOV
Increasing Intensity of Intervention
Prone Positioning
Lower Tidal Volume/Pplat +ECCO2R
Neuromuscular Blockade
Higher PEEP
Low-Moderate PEEP
Low Tidal Volume Ventilation
Mild ARDS
300
250
Moderate ARDS
200
The ARDS Definition Taskforce. JAMA 2012;307:2526-2533
150
PaO2/FiO2
Severe ARDS
100
50
0
Neuromuscular blockade
• Cisatracurium besylate mc used
• Minimizes WOB and improves oxygenation
• Decreases inflammatory biomarkers in both
blood and BAL fluid
• Problem with progressive atelectasis due to
diaphragmatic tone (hypoxemia) and ICU
acquired weakness
• 3 Trials- 431 pts; 20 centers, France)
• Cisatracurium besylate (given x 48h, fixed high dose
(15mg bolus then 37.5mg continuous)
• Improved oxygenation(24-72h) and less barotrauma
• Risk of death @ 28d(RR, 0.66; 95% CI, 0.500.87;p=0.003)
• ICU mortality (RR, 0.7; 95% CI, .55-.89; p=0.004)
• Hospital mortality (RR, 0.7; 95% CI, .58-.91;
p=0.005)
• No change in duration of MV , even among survivors,
ICU weakness
ECMO
Inhaled NO
HFOV
Increasing Intensity of Intervention
Prone Positioning
Lower Tidal Volume/Pplat +ECCO2R
Neuromuscular Blockade
Higher PEEP
Low-Moderate PEEP
Low Tidal Volume Ventilation
Mild ARDS
300
250
Moderate ARDS
200
The ARDS Definition Taskforce. JAMA 2012;307:2526-2533
150
PaO2/FiO2
Severe ARDS
100
50
0
• Meta-analysis of randomized controlled trials on proning in
ARDS and ALI
• 1675 pts, 862 ventilated prone
• Overall no reduction in ICU mortality(OR=0.91, 95% CI = 0.751.2, p=0.39)
• Four latest with ARDS showed decreased ICU mortality
(OR=0.71; 95% CI = 05-0.99; p= 0.048)
• No associated increased major airway complications.
• HFOV is an alternative/rescue strategy ventilation that
delivers very small tidal volumes at high frequencies (3-15 Hz)
using a oscillating pump.
• To avoid overdistention of alveoli
• Prevent end-expiratory alveolar collapse
• Maintain alveolar recruitment by applying a constant airway
pressure
• All goals of lung-protective ventilation
Ventilator Protocols.
Ferguson ND et al. N Engl J Med 2013;368:795-805.
Baseline Characteristics of the Patients.
Ferguson ND et al. N Engl J Med 2013;368:795-805.
Outcomes.
Ferguson ND et al. N Engl J Med 2013;368:795-805.
Probability of Survival from the Day of Randomization to Day 60 in the HFOV and Control Groups.
Ferguson ND et al. N Engl J Med 2013;368:795-805.
Baseline Characteristics of the Patients.
Young D et al. N Engl J Med 2013;368:806-813.
Proportions of Patients Undergoing High-Frequency Oscillatory Ventilation (HFOV) during the First 30 Days,
According to Study Group.
Young D et al. N Engl J Med 2013;368:806-813.
Ventilatory Variables during the First 3 Study Days.
Young D et al. N Engl J Med 2013;368:806-813.
Kaplan–Meier Survival Estimates during the First 30 Study Days.
Young D et al. N Engl J Med 2013;368:806-813.
• 6 RCTs, 1608 pts with ARDS
• Compare CMV to HFOV no significant reduction in 28 or 30 d
mortality (pooled RR=1.051, 95% CI 0.813-1.358)
• No reduction in ICU mortality(RR=1.218, 95% CI 0.925-1.604)
• HFOV showed improved effect for oxygenation but no effect
on ventilation failure and duration of mechanical ventilation.
• The risk of barotrauma and hypotension were similar (CMV
and HFOV).
ECMO
Inhaled NO
HFOV
Increasing Intensity of Intervention
Prone Positioning
Lower Tidal Volume/Pplat +ECCO2R
Neuromuscular Blockade
Higher PEEP
Low-Moderate PEEP
Low Tidal Volume Ventilation
Mild ARDS
300
250
Moderate ARDS
200
The ARDS Definition Taskforce. JAMA 2012;307:2526-2533
150
PaO2/FiO2
Severe ARDS
100
50
0
Griffiths MJ, Evans TW. N Engl J Med 2005;353:2683-2695.
Griffiths MJ, Evans TW. N Engl J Med 2005;353:2683-2695.
Regulation of the Relaxation of Vascular Smooth Muscle by Nitric Oxide.
Griffiths MJ, Evans TW. N Engl J Med 2005;353:2683-2695.
Inhaled nitric oxide (NO) reaches only the ventilated alveoli and thus vasodilates only the
ventilated pulmonary vessels, which improves ventilation-perfusion matching (V̇/Q̇).
Stephen R Collins, and Randal S Blank Respir Care
2011;56:1573-1582
(c) 2012 by Daedalus Enterprises, Inc.
ECMO
Inhaled NO
HFOV
Increasing Intensity of Intervention
Prone Positioning
Lower Tidal Volume/Pplat +ECCO2R
Neuromuscular Blockade
Higher PEEP
Low-Moderate PEEP
Low Tidal Volume Ventilation
Mild ARDS
300
250
Moderate ARDS
200
The ARDS Definition Taskforce. JAMA 2012;307:2526-2533
150
PaO2/FiO2
Severe ARDS
100
50
0
Extracorporeal membrane oxygenation.
Stephen R Collins, and Randal S Blank Respir Care
2011;56:1573-1582
(c) 2012 by Daedalus Enterprises, Inc.
Diagram of a typical veno-venous extracorporeal membrane oxygenation system.
David A Turner, and Ira M Cheifetz Respir Care
2013;58:1038-1052
(c) 2012 by Daedalus Enterprises, Inc.
Diagram of a typical veno-arterial extracorporeal membrane oxygenation system.
David A Turner, and Ira M Cheifetz Respir Care
2013;58:1038-1052
(c) 2012 by Daedalus Enterprises, Inc.
Diagram of an appropriately positioned Avalon double-lumen VV ECMO cannula.
David A Turner, and Ira M Cheifetz Respir Care
2013;58:1038-1052
(c) 2012 by Daedalus Enterprises, Inc.
Adult Respiratory ECMO Complications Reported to the Extracorporeal Life Support
Organization.
David A Turner, and Ira M Cheifetz Respir Care
2013;58:1038-1052
(c) 2012 by Daedalus Enterprises, Inc.
Configuration-related mortality.
Frederik Stöhr et al. Interact CardioVasc Thorac Surg
2011;12:676-680
Published by European Association for Cardio-Thoracic Surgery. All rights reserved.
Effort-Adapted Modes
• Proportional Assist Ventilation (PAV): partial
support (vent assist α pt effort) which relieves
resistive and elastic burden. Volume to
overcome elastance or flow to overcome
resistance
• NAVA: same as PAV but responds to neural input
from electrical activity of diaphragm (Edi).
Pressure applied linear α Edi, req. esophageal
electrode (like NGT), vent trigger is Edi or
conventional signals whichever is first.
Effort-Adapted Modes
• Adaptive Support Ventilation(ASV): set target
minute ventilation (RR X VT) based on pt’s E
time constant and dynamic compliance with
preset PBW, min. MV limit, and pressure limit.
Combine the most effective RR and VT, with
limited pressure support, to WOB.
Mode
Pro
Con
Outcome
PAV
Improved synchrony,
better physiologic
breathing, and sleep
Relies on mechanical
effort of pt. Needs
continuous data for
elastic and resistive
Can over assist and
delay inspiration
(“runaway
phenomenon”)
None
NAVA
Improved synchrony,
preserved breathing
variability
High NAVA and high
Edi leads to high
inspiratory pressure
and VT( unstable or
high resp drive)
None
ASV
wob, improved ptvent interaction
Not for HD unstable or None
severely hypoxemic