Brain & Cranial Nerves
advertisement

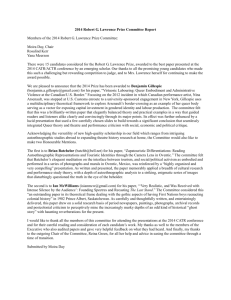
Dr. Michael P. Gillespie Between the brain and spinal cord. 3 regions. Medulla oblongata. Pons. Midbrain. Dr. Michael P. Gillespie 2 A continuation of the spinal cord. Sensory (ascending) tracts and motor (descending) tracts travel through the white matter of the medulla. Many nerves decussate (cross over) in the medulla. Dr. Michael P. Gillespie 3 Cardiovascular center regulates the heartbeat and the diameter of the blood vessels. Dr. Michael P. Gillespie 4 The medullary rhythmicity area adjusts the rhythm of the breathing and controls reflexes for vomiting, coughing, and sneezing. Dr. Michael P. Gillespie 5 The nuclei for the following cranial nerves reside in the medulla: VIII (vestibulocochlear). IX (glossopharyngeal). X (vagus). XI (accessory). XII (hypoglossal). Dr. Michael P. Gillespie 6 Pneumotaxic area and apneustic area regulate breathing. Nuclei for cranial nerves V (trigeminal), VI (abducens), and VII (facial). Dr. Michael P. Gillespie 7 The midbrain or mesencephalon contains the superior colliculi (visual actvities) and inferior colliculi (auditory pathways). The midbrain contains the substantia nigra which release dopamine to help control subconscious muscle activities. Loss of these neurons results in Parkinson disease. Cranial nerves III (oculomotor) and IV (trochlear) originate here. Dr. Michael P. Gillespie 8 Dr. Michael P. Gillespie 9 Dr. Michael P. Gillespie 10 Dr. Michael P. Gillespie 11 Dr. Michael P. Gillespie 12 Dr. Michael P. Gillespie 13 Type: sensory. Function: smell. Anosmia – loss of sense of smell. Does not connect with the brainstem. Dr. Michael P. Gillespie 14 Dr. Michael P. Gillespie 15 Type: sensory. Function: vision. Anopia – blindness in one or both eyes. Dr. Michael P. Gillespie 16 Type: mixed (mainly motor). Function: movement of the upper eyelid and eyeball. Accomodation of the lens for near vision and constriction of the pupil. Strabismus – deviation of the eye in which both eyes don’t focus on the same object. Ptosis – drooping of the upper eyelid. Diploia – double vision. Dr. Michael P. Gillespie 17 Type: mixed (mainly motor). Function: movement of the eyeball. Diplopia and strabismus occur with trochlear nerve damage. Dr. Michael P. Gillespie 18 Dr. Michael P. Gillespie 19 Type: mixed. Function: conveys impulses for touch, pain, temperature and proprioception. Chewing. Trigeminal neuralgia (tic douloureux) – pain to branches of the trigeminal nerve. Dentists apply anesthetic to branches of this nerve. Dr. Michael P. Gillespie 20 Dr. Michael P. Gillespie 21 Type: mixed (mainly motor). Function: movement of the eyeball. With damage to this nerve the eye cannot move laterally beyond the midpoint and usually points medially. Dr. Michael P. Gillespie 22 Dr. Michael P. Gillespie 23 Type: mixed. Function: Propriception and taste. Facial expression. Secretion of saliva and tears. Injury produces bell’s palsy (paralysis of facial muscles). Dr. Michael P. Gillespie 24 Dr. Michael P. Gillespie 25 Type: mixed (mainly sensory). Function: conveys impulses for equilibrium and hearing. Injury can cause vertigo, ataxia (muscular incoordination), nystagmus (rapid movement of the eyeball), and tinnitus. Dr. Michael P. Gillespie 26 Type: mixed. Function: taste and somatic sensations from the posterior 1/3 of the tongue. Elevates the pharynx during swallowing and speech. Stimulates the secretion of saliva. Injury causes decreased salivary secretion, loss of taste, and difficulty swallowing. Dr. Michael P. Gillespie 27 Dr. Michael P. Gillespie 28 Type: mixed. Function: taste and somatic sensations. Swallowing, coughing, and voice production. Regulates GI tract and heart rate. Injury interferes with swallowing, paralyzes vocal cords, and causes the heart rate to increase. Dr. Michael P. Gillespie 29 Dr. Michael P. Gillespie 30 Type: mixed (mainly motor). Function: Proprioception. Swallowing, movement of head and shoulders. If the nerves are damaged the SCM and Trapezius become paralyzed. Dr. Michael P. Gillespie 31 Dr. Michael P. Gillespie 32 Type: mixed (mainly motor). Function: Proprioception. Movement of the tongue during speech and swallowing. Injury results in difficulty in chewing, speaking, and swallowing. When protruded, the tongue curls towards the affected side and atrophies on the affected side. Dr. Michael P. Gillespie 33 Dr. Michael P. Gillespie 34 I – Olfactory VII – Facial II – Optic VIII – Auditory III – Oculomotor IV – Trochlear V – Trigeminal VI – Abducens (Vestibulocochlear) IX – Glossopharyngeal X – Vagus XI – Spinal accessory XII - Hypoglossal Dr. Michael P. Gillespie 35 On Old Olympus’ Towering Tops A Fin And German Viewed Some Hops. This mnemonic device helps you memorize the names of the cranial nerves. The first letter from each word corresponds to the first letter of each cranial nerve. Dr. Michael P. Gillespie 36 Some Say Marry Money, But My Brother Says Big Brains Matter Most. This mnemonic device helps you memorize the sensory / motor distribution of the cranial nerves. S = sensory M = Motor B = Both Dr. Michael P. Gillespie 37 Twelve pairs of cranial nerves exit from the brain and brainstem. These nerves innervate the face, head, and neck. They control all sensory and motor functions in these areas including the special senses of vision, hearing, smell, and taste. Cranial trauma, infections, aneurysm, stroke, degenerative diseases (i.e. multiple sclerosis), upper motor neuron lesions, lower motor neuron lesions, increased intracranial pressure, and abnormal masses or tumors can all affect the cranial nerves. Dr. Michael P. Gillespie 38 Some facial movements are performed in bilateral synchrony such as swallowing and moving the forehead and are thus innervated bilaterally. Fine movements of the face are unilateral. The contralateral hemisphere innervates the affected area. Dr. Michael P. Gillespie 39