June 2007
advertisement

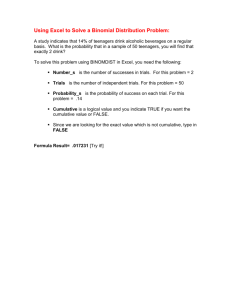
Bench to Bedside A Curious Tail of Elephants, Rodents and other Primates or Bedside to Bench? Michael Goodyear Department of Medicine, Queen Elizabeth II Health Sciences Centre, Dalhousie University, Halifax, Nova Scotia, Canada MSMR Waltham MA, June 2007 “If you have cancer and you're a mouse, we can take good care of you" Judah Folkman NY Times May 1988 Animal Welfare better than People’s? “The current situation in which national oversight of research involving animals is far more effective and independent than that for research involving humans would we believe be profoundly upsetting to the Canadian people”. The Governance of Health Research Involving Human Subjects. Law Commission of Canada, 2000. Learning Objectives • I: The Bad News: The corruption of science • II: Learning from disasters: The story of TGN1412 • III: The Good News: Approaching transparency Summary Part I The Bad News: The corruption of science The Collapse of Scientific Integrity • • • The ongoing crisis in public confidence and trust The corrosion of the evidence base in EBM Ongoing concerns Declaration of Helsinki WORLD MEDICAL ASSOCIATION DECLARATION OF HELSINKI Ethical Principles for Medical Research Involving Human Subjects 1964 16. Every medical research project involving human subjects should be preceded by careful assessment of predictable risks and burdens in comparison with foreseeable benefits to the subject or to others 18. Medical research involving human subjects should only be conducted if the importance of the objective outweighs the inherent risks and burdens to the subject Vera Hassner Sharav, M.L.S. Rosiglitazone Class: Thiazolidinedione May 21, 2007 Rosiglitazone and Cardiovascular Risk Bruce M. Psaty, M.D., Ph.D., and Curt D. Furberg, M.D., Ph.D. Cardiovascular Health Research Unit, Departments of Medicine, Epidemiology, and Health Services, University of Washington, and the Center for Health Studies, Group Health, Seattle; and the Division of Public Health Sciences, Wake Forest University, WinstonSalem, NC Rosiglitazone The possibility of cardiovascular benefit associated with the use of rosiglitazone seems remote. In view of the potential cardiovascular risks and in the absence of evidence of other health advantages, except for laboratory measures of glycemic control, the rationale for prescribing rosiglitazone at this time is unclear. Unless new data provide a different picture of the risk–benefit profile, regulatory action by the Food and Drug Administration (FDA) is now warranted. Rosiglitazone During the market life of rosiglitazone, tens of millions of prescriptions for the drug have been written for patients with type 2 diabetes. Rosiglitazone represents a major failure of the drug-use and drug-approval processes in the United States. Rosiglitazone Physicians who chose to prescribe rosiglitazone focused on the single dimension of glycemic control. The underlying assumption represents a kind of linear "physiological" argument: high levels of glycated hemoglobin increase risk, so a reduction in glycated hemoglobin will automatically translate into improved health outcomes for patients. Many physicians did not require proof of health benefits as a criterion for selecting rosiglitazone as a therapy for type 2 diabetes. Rosiglitazone Had practicing physicians required this higher standard, they would have been at a loss for evidence from large, long-term trials. Rosiglitazone was approved on the basis of short-term studies of the surrogate end point of glycemic control. The use of surrogate end points in the drug-approval process has been problematic Rosiglitazone Rofecoxib, whose biologic actions early on suggested the possibility of both gastrointestinal benefit and cardiovascular harm, represented a similar regulatory failure to insist on large trials of public health importance in a timely fashion. Rofecoxib Class: COX-2 Inhibitor Pharmacoeconomics After Sanctions, Doctors Get Drug Company Pay Gardiner Harris and Janet Roberts June 3, 2007 A decade ago the Miinesota Board of Medical Practice accused Dr. Faruk Abuzzahab of a “reckless, if not willful, disregard” for the welfare of 46 patients, 5 of whom died in his care or shortly afterward. The board suspended his license for seven months and restricted it for two years after that. But Dr. Abuzzahab, a Minneapolis psychiatrist, is still overseeing the testing of drugs on patients and is being paid by pharmaceutical companies for the work. At least a dozen have paid him for research or marketing since he was disciplined. One of Dr. Abuzzahab’s patients was David Olson, whom the psychiatrist tried repeatedly to recruit for clinical trials. Drug makers paid Dr. Abuzzahab thousands of dollars for every patient he recruited. In July 1997, when Mr. Olson again refused to be a test subject, Dr. Abuzzahab discharged him from the hospital even though he was suicidal, records show. Mr Olson committed suicide two weeks later. From 1997 to 2005, at least 103 doctors who had been disciplined or criticized by the state medical board received a total of $1.7 million from drug makers. The median payment over that period was $1,250; the largest was $479,000. Part II Learning from disasters: The story of TGN1412 Is animal testing still relevant? Pharmacological Evolution • Switching from classic chemical pharmacology to biological – Loss of classic dose-response paradigms • Humanisation of antibodies – Intra-species variation – Immunogenicity in animals, neutralisation and masking of toxicity • Increasing uncertainty Safety in Phase I First-in-Man Trials • Repeated reassurances – Orme M et al. Br J Clin Pharmacol 1989 27: 125 • Mild 6.9% • Moderate 0.55% • Serious 0.04% – Sibille M et al. Eur J Clin Pharmacol 1986 20: 243 – Lutfullin AJ et al. Int J Clin Pharmacol Ther 2005 43: 217 • Severe 0.2% – BUT: None were biological trials Learning Opportunities • TGN1412 and Cytokine Release Syndrome • Natalizumab and Progressive Multifocal Leukoencephalopathy (PML) TGN1412 “A Watershed Incident” Fiona Godlee, Editor BMJ A line in the sand? A cautionary tale from Waltham MA VOLUME 332 25 MARCH 2006 677-8 Learning from the TGN1412 trial This experience should foster an open culture in medical research Michael Goodyear Department of Medicine, Dalhousie University, Halifax, Nova Scotia, Canada Hell of human guinea pigs How the drug trial horror unfolded By MICHAEL SEAMARK 17th March 2006 We saw human guinea pigs explode Victims tearing at shirts By NICK PARKER, EMMA MORTON and JACQUI THORNTON 16th March 2006 Myfanwy Marshall, 35, whose boyfriend is critically ill, said the normally healthy 28year-old barman's face was so puffed, he "looks like the Elephant Man ". He looks like a monster. One victim was named as Ryan Flanagan, 21, a student from Highbury, north London. His family was told that he could not breathe and that his head had swollen to three times its normal size. 17 March 2007 334: 566-7 “We Saw human guinea pigs explode”: Newspaper coverage of adverse events in the TGN14412 trial Stobbart L, Murtagh MJ, Rapley T et al. Institute of Health and Society, Newcastle University, Newcastle upon Tyne Peer Review • Wood AJ, Darbyshire J. Injury to research volunteers--the clinicalresearch nightmare. N Engl J Med. 2006 May 4;354(18):1869-71 • Ho MW, Cummins J. London Drug Trial Catastrophe – Collapse of Science and Ethics: Postmortem on the TGN1412 disaster Science in Society. 2006 Summer 30: 44-5 • Liedert B, Bassus S, Schneider U et al. Safety of phase I clinical trials with monoclonal antibodies in Germany – the regulatory requirements viewed in the aftermath of the TGN1412 disaster International Journal of Clinical Pharmacology and Therapeutics 2007 45(1) 1-9 The Elephant in the Room Editorial 14 December 2006 Less satisfactory is the Government’s failure so far to hold anybody accountable for the Northwick Park incident. The MHRA exonerated both itself and Parexel. Loxodonta africana SUN: A VOLUNTEER who escaped the drug test disaster told last night how he saw six healthy young men turn into wailing wrecks within minutes. Human guinea pig Raste Khan — who did not know he had been given a harmless placebo in the test — said it was like a horror film unfolding before his eyes. Cavia porcellus Homo sapiens RASTE KHAN “The test ward turned into a living hell minutes after we were injected. The men went down like dominoes. First they began tearing their shirts off complaining of fever, then some screamed out that their heads felt like they were about to explode” “After that they started fainting, vomiting and writhing around in their beds” “It was terrifying because I kept expecting it to happen to me at any moment. But I felt fine and didn’t know why. An Asian guy next to me started screaming and his breathing went haywire as though he was having a terrible panic attack” RASTE KHAN “They put an oxygen mask on him but he kept tearing it off, shouting ‘Doctor, doctor, please help me!’ He started convulsing, shouting that he was getting shooting pains in his back.” TGN1412 TGN 1412 CD28 T Cell Receptor SuperAgonist CD28 Humanised IgG4 Mouse anti-Human CD28 Monoclonal Antibody TGN 1412 • CD28 – – Costimulatory receptor on CD4+ and CD8+ T Cells • Requires costimulation from T cell antigen receptor (TCR) to activate T helper cells • TGN1412 bypasses TCR and activates T cells irrespective of TCR specificity TGN 1412 • By-passes Costimulation by Antigen Presenting Cell TGN 1412 Phase I First Time in Man • $4,000 Incentive • March 13 2006 08.00 • 8 Subjects in first dose level cohort – Healthy Male Volunteers, Age 26 (19-34) • 2 Placebo – hidden allocation • 6 Active • All 8 treated in rapid succession – 3-6 min ivi • Dose based on NOAEL TGN 1412 NOAEL: No Observed Adverse Effect Level • Primates tested up to 50mg/kg – (NOAEL) • Clinical testing started at 1/500 NOAEL – 0.1mg/kg TGN 1412 • BUT: NOAEL ≠ Pharmacological effect (NOEL) (0.3 – 5.0mg/kg) • Therefore: – Treated close to Effect Level (0.1mg/kg) TGN 1412 Effects • Rapid onset – Cytokine Release Syndrome – Angioedema Testing continued • Multiple Organ Failure • All subjects admitted to ICU • Prolonged immunosuppression TGN 1412 Treatment • Life support • High dose steroids • Daclizumab (anti-IL2 receptor antagonist) TGN 1412 Amputations for dry gangrene TGN 1412 Currently • Loss of memory • Inability to concentrate • Headaches • Ulcers TGN 1412 Medicines and Healthcare Products Agency (MHRA) • Suspended CTA • Immediate Inquiry • Released – protocol, review and inquiry • Reports April 5, May 25 • FIM Immunomodulation trials on indefinite hold UK Government announced independent expert inquiry No review of ethical review TGN 1412 Expert Inquiry (Terms of Reference) • What may be necessary in transition from preclinical to first-in-man Phase 1 studies, specifically: – Biological molecules with novel mechanisms of action – New agents with highly species-specific action – New drugs for immune system targets • Interim report within 3 months, final in 6 • Minutes of meetings and interim findings to be made public TGN 1412 Expert Scientific Group Inquiry Chair Professor Sir Gordon Duff Florey Professor of Molecular Medicine University of Sheffield Expert Scientific Group Phase One Clinical Trials Interim Report 25th July 2006 Final Report 30th November 2006 VOLUME 333 5 AUGUST 2006 270-1 Further lessons from the TGN1412 tragedy New guidelines call for a change in the culture of research Michael Goodyear Department of Medicine, Dalhousie University, Halifax, Nova Scotia, Canada Further Lessons • Common sense, avoiding blame • A retreat from blind process to judiciousness – Stopping the clock • Recognises the problem of increasing commercialisation, • • • • • and lack of experience and planning Places onus on sponsor to demonstrate need Places openness above proprietary interests While constrained by narrow remit, needs to draw attention to broader issues Failed to identify the elephant in the room Why are we asking these questions now? Testing Antibody Therapies: Position Paper April 2006 Had previously warned of possibility in November 2005 - Early Stage Clinical Trial Taskforce July 2006 Volume 355:1018-1028 September 61, 2006 Number 10 Cytokine Storm in a Phase 1 Trial of the Anti-CD28 Monoclonal Antibody TGN1412 Ganesh Suntharalingam, F.R.C.A., Meghan R. Perry, M.R.C.P., Stephen Ward, F.R.C.A., Stephen J. Brett, M.D., Andrew Castello-Cortes, F.R.C.A., Michael D. Brunner, F.R.C.A., and Nicki Panoskaltsis, M.D., Ph.D. Department of Intensive Care Medicine, Northwick Park and St. Mark's Hospital, Watford Rd., Harrow, London HA1 3UJ, United Kingdom 1. On-line August 14 Event times for 8 healthy volunteers in TGN1412 study 13 March 2006 Volunteer Allocation Time of i.v. Time to ICU A B C D E F G H TG 8.4mg Placebo TG 6.8mg TG 8.8mg TG 8.2mg TG 7.2mg TG 8.2mg Placebo 08:00 08:10 08:20 08:30 08:40 08.50 09:00 09:10 16 hrs 15.5hrs 16hrs 12hrs 16hrs 16hrs ICU Cytokine Release D1-5 Report of the Working Party on Statistical Issues in First-in-Man studies Royal Statistical Society March 2007 Central Committee on Research inv. Human Subjects • FIM trials with high risk agents will require input from an Expert Advisory Group prior to CTA application Feb 7 2007 • Convened “Lessons from TGN-1412” Conference, and Implementation Committee • Developing accreditation of investigators and sites • Developed guidance through EMEA GUIDELINE ON REQUIREMENTS FOR FIRST-IN-MAN CLINICAL TRIALS FOR POTENTIAL HIGH-RISK MEDICINAL PRODUCTS London, March 2007 Recommendations (1) Expert Group: 22 Recommendations - Safety and Good Science - 1. Preclinical and early clinical development 2. Preparation and review of clinical trials 3. 4. 5. applications Determining and administering the initial dose in humans The clinical environment for first-in-man studies Developing expertise Recommendations (2) 1. Preclinical and early clinical development • • • • Development must be on case by case basis, and risk based Regulatory process to be reviewed regularly All preclinical and Phase I data must be available and shared Presubmission should include expert consultation Recommendations (3) 2. Preparation and review of clinical trials applications • Timelines must be flexible Recommendations (4) 3. Determining and administering the initial dose in humans • Dose selection must go beyond NOEL and NOAEL Minimal Anticipated Biological Effect Level (MABEL) If preclinical models provide little information – err on side of caution Use Slow infusions Design must be justified scientifically and statistically • • • • Recommendations (5) 3. (Cont’d.) • Agents should not be administered to more than • one subject simultaneously Choice of healthy volunteers must be justified Recommendations (6) 4. The clinical environment for first-in-man studies • • • PIs must be highly qualified Contingency plans for SAEs must be in place FIM studies should take place in specialised centres Recommendations (7) 5. Developing expertise • Specialised training of investigators is needed together with development of specialist centres Recommendations (8) • Many issues were raised that were outside the remit of the committee – Consent – Communication – Insurance – Research Ethics Committees – Follow up of subjects • Recommend these be investigated Recommendations • Statistical expertise must be available • All parties must be adequately insured • There should be agreed guides for • • • classifying risk In vitro studies with human tissue should be part of preclinical development Risk should be numerical not verbal No healthy volunteers in high risk trials Draft Guideline Consultation to May 23 • Attempt to implement recommendations • Relevance of animal models must be justified • IDMSC Criticised as weak Vol 25(5) May 2007 485 Critics pan timid European response to TeGenero disaster “EMEA’s record on enforcement is tenuous” EMEA ‘passing the buck’ with clinical trial guideline DrugResearcher.com March 29 2007 An exercise in regulatory face-saving or a genuine attempt to improve safety? Pharmaceutical Executive Europe May 1 2007 “At stake is the credibility of the healthcare sector” The American Journal of Bioethics, Volume 7 Issue 2 2007 76-81 Money and Distorted Ethical Judgments about Research: Ethical Assessment of the TeGenero TGN1412 Trial Ezekiel J. Emanuel; Franklin G. Miller Department of Clinical Bioethics, National Institutes of Health, Bethesda Responses • Risk, Judgment and Fairness in Research Incentives 82 – 83 • • • • • Benjamin Hale Evaluation of Research Design by Research Ethics Committees: Misleading Reassurance and the Need for Substantive Reforms 84 – 86 Howard Mann Money Matters 86 – 88 Toby Schonfeld; Bruce Gordon; Jean Amoura; Joseph Spencer Brown Money, Advertising and Seduction in Human Subjects Research 88 – 90 Trisha B. Phillips Ethical Flaws in the TeGenero Trial 90 – 92 Adil Shamoo; Elizabeth Woeckner Faulty Premise, Premature Conclusion: That Money Was Extraneous to the Research Ethics of the TGN1412 Study 93 – 94 Bethany Spielman Allied Research International is always recruiting for normal healthy study participants for our phase I and bioequivalence studies. We conduct our studies in a cheerful, safe, and respectful environment. Our meals are second to none and …now with 100% more pool tables! $950 Swiss Cheese Model of Patient Safety (Reason) Lessons to be learnt from TGN 1412 (1) • Recruitment – Financial Incentives • Adequacy of Information • Choice of Subject in Phase I • Number of Subjects • Timing of Administration Lessons to be learnt from TGN 1412 (1) • Recruitment • Adequacy of Information – Consent • Choice of Subject in Phase I – Healthy volunteers • Number of Subjects • Timing of Administration Lessons to be learnt from TGN 1412 (2) • Sources of Information Reviewed – Regulatory Review – Ethical Review • Place of Independent Expert Review • Relevance of Preclinical Testing – Interspecies difference (Macaca) • Transparency in Development – Publishing preclinical work • Transparency of Reviews • Response to Disasters Lessons to be learnt from TGN 1412 (3) • Caution in – developing immunomodulators – agonists – bypassing regulatory mechanisms (super) • Assumptions about Dose-Response – non-linear – bell shaped • (optimum dose in Macaca was 5mg/kg) Lessons to be learnt from TGN 1412 (4) • Homology may not mean affinity • Affinity may not translate downstream • Even monoclonals are not specific • Standards for preclinical testing • Avoid check-box mentality Lessons to be learnt from TGN 1412 (4) The Immune System is a Capricious Pandora’s Box! Pandora 1898. John William Waterhouse British Pre-Raphaelite (1849-1917) Private collection, Oil on canvas Lessons to be learnt from TGN 1412 (5) • Relationships with industry • Adequacy of training of staff • Adequacy of facilities • Adequacy of liability insurance Plan for the worst, hope for the best The Relevance of Animal Testing Altern Lab Anim. 2006 May;34(2):225-3 TGN1412: time to change the paradigm for the testing of new pharmaceuticals Bhogal N, Combes R Focus On Alternatives Fund for the Replacement of Animals in Medical Experiments The Relevance of Animal Testing Toxicology in Vitro 2007 Mar 1 Immunostimulatory antibodies: Challenging the drug testing paradigm Bhogal N, Combes R Information provided to regulatory authorities on epitope homology differs substantially from what is known a) The normal co-stimulatory mechanism of T-cell activation b) TGN1412 recognises single CD28 on receptor Bhogal, Combes 2006 CD28 Receptor a) CD28 monomer and corresponding TGN1412 binding epitope b) 3-D model of CD28 extracellular domain TGN1412 binding epitope ( C’’D loop ) circled – 6 AAs Bhogal, Combes 2006 Rattus rattus Sylvilagus audubonii Mus musculus Macaca mulatta (Rhesus) Macaca fasicularis (Cynomulgus) Conservation of amino acid sequences of CD28. Substitution of Glutamate (E) in Macaca mulatta (Rhesus) for Glycine (G) in human, could have profound conformal implications, and hence affect affinity binding and downstream effects. Bhogal, Combes 2006 2007 Apr 1;109(7):2968-77 Physiologic and aberrant regulation of memory T-cell trafficking by the costimulatory molecule CD28 Mirenda V, Jarmin SJ, David R, Dyson J, Scott D, Gu Y, Lechler RI, Okkenhaug K, Marelli-Berg Federica M. Department of Immunology, Division of Medicine, Imperial College London, Hammersmith Campus, London, United Kingdom How Clean is Your Lab? • Memory helper T cells react differently to TGN1412 than do Ag naïve T cells • Humans have up to 50% T cells activated (memory) • Laboratory animals have few memory T cells due to rearing conditions • CD28 activated memory T cells migrate into extra-lymphoid tissues causing damage, naïve T cells do not Why use inbred pathogen free animals to test drugs to be used on outbred pathogen exposed people? Activated T cells susceptible to over stimulation if isolated from costimulatory requirements of antigen specificity Sharpe AH, Abbas AK NEJM 2006 Sep 7;355(10):973-5. National Institute for Biological Standards and Control NIBSC scientists replicate trial results: In vitro tests with human immune cells and TGN1412 produced polyclonal expansion and cytokine release Higher doses, as used in the preclinical studies did not produce this response. The dose given to the volunteers was the maximum immunostimulatory dose. Non-human primate cells did not show a similar effect, nor were there any adverse effects in-vivo Inglis S. December 2007 ESG Final Report TGN1412 TGN1412 Evoked Evoked Activation Proliferation ______________________________________ Human ++++ ++++ PBMC ______________________________________ Macaca ++ PBMC ______________________________________ PBMC: Peripheral Blood Mononuclear Cells Mehrishi J, Szabo M, Bakacs T. Vaccine 2007 25(18) 3517 The Relevance of Animal Testing "The relevance of animal testing, whether artificially created disease models or healthy animals for toxicology, has to be very seriously questioned for testing of human-specific biologic drugs. That's one of the key lessons of TGN1412." Dr David Glover Nature Biotechnology Vol 25(5) May 2007 485 The Relevance of Animal Testing All reports were highly critical of limitations of animal tests in predicting biological and pharmacological effects in humans The Relevance of Animal Testing Academy of Medical Sciences/ Medical Research Council/ Royal Society/ Wellcome Trust Study into the use of Non-human Primates (NHP) in Research 12 December 2006 Chair Sir David Weatherall Regius Professor of Medicine, Oxford University Director, Institute of Molecular Medicine “To examine the scientific basis for recent, current and future use of non-human primates within biological and medical research” Non-human Primates • Keep to a minimum • Only where absolutely necessary • Optimise care • Only in centres of excellence • Details on welfare should be in publications • Encourage alternatives Learning from Mistakes • We have been assured repeatedly that proper procedures were followed, when the real question is whether they were the right procedures. Goodyear M. BMJ March 25th 2006 • Nor will a collective claim of ‘not-guilty’ likely lead to understanding and correction Goodyear M. 2006 Potentially Incompatible Goals at F.D.A. GARDINER HARRIS June 11, 2007 Safety and speed are the yin and yang of drug regulation. Patients want immediate access to breakthrough medicines but also want to believe the drugs are safe. These goals can be incompatible. Race a drug to market and much is likely to remain unknown when patients take it. Test a drug thoroughly to assess all possible risks and its release may be delayed by years. Health Research buckles under burden of red tape Tony Tysome 5 May 2007 Academics have called for urgent action to end the "bureaucratic nightmare" that is currently stifling vital health-related research across the UK. Thousands of researchers who are conducting studies involving the National Health Service are struggling to cope with red tape designed to regulate the quality of their work and protect hospital patients. Research proposals are being held up or dropped altogether because of the time and costs involved in gaining approval from the governance and ethics committees The Fall Out • Virtual shut down of phase I testing in UK • Migration to less regulated environments (US) "Is there any point to which you would wish to draw my attention?" "To the curious incident of the dog in the night-time." "The dog did nothing in the night-time." "That was the curious incident," remarked Sherlock Holmes. Conan-Doyle A. Silver Blaze 1892 Part III The Good News: Approaching transparency Moving Forward • Response to TGN1412 – This tragedy creates one more imperative for an open culture in medical research, a culture that many fear is increasingly losing its way Goodyear M. BMJ March 25th 2006 His call for a culture of greater openness in medical research is, I think, both powerful and timely Gunn A USA TODAY March 27th 2006 – Maximum transparency to reaffirm trust in clinical trials and their regulation. Commercial confidentiality should not obstruct independent scrutiny Lancet March 25th 2006 Moving Forward • There is focus on sharing of information relevant to safety… regulatory authorities should expedite the collection of information from unpublished pre-clinical studies…in the interests of safety, we believe that the ultimate goal should be an open access database Expert Scientific Group Dec 2006 Clinical trial registration: Transparency is the watchword Sim I et al. May 20th 2006 Opening Address to World Health Assembly, May 2005 "We are ready forward with to move an International Clinical Trials Dr Jong-wook Lee WHO Director-General (died May 22 2006) Registry. This will do much to strengthen the research process and its ability to win public trust" I Sim January 2, 2007; 176 (1). Free access to medical information: A moral right? Michael Goodyear Department of Medicine, Dalhousie University, Halifax, NS May 2007 54: 331-335 Reporting research results: A moral obligation for all researchers David Moher Department of Pediatrics, Epidemiology & Community Medicine, University of Ottawa, Children's Hospital Eastern Ontario Research Institute, Ottawa, Ontario, Canada May 2007 54: 380-388 Publication bias in the medical literature: A review by a Canadian Research Ethics Board Hall R, de Antueno C, Webber A Dalhousie University and the Capital District Health Authority, Halifax, Nova Scotia, Canada •44% Publication rate •Phase III/IV >I/II •Pharmaceutical Industry<Grant •Significant >Insignificant WHO http://www.who.int/ictrp/en/ May 4 2007 Results reporting Once a trial is registered, full transparency and accountability requires that all of the trial's results be made available to the public in a timely manner. The ICMJE recognizes the potential benefit of having information about preliminary trials in the public domain, because these studies can guide future research or signal safety concerns. The ICMJE is expanding the definition of the types of trials that must be registered to include these preliminary trials and adopts the WHO’s definition of clinical trial: “any research study that prospectively assigns human participants or groups of humans to one or more healthrelated interventions to evaluate the effects on health outcomes” June 2007 The ICMJE will not consider results posted in the register as previous publication if the results are presented in the form of a brief, structured abstract or table. The ICMJE favors a standard abstract format for results reporting, and the CONSORT group’s guidelines for abstracts related to trials may be one such option. The ICMJE believes that parties should consider requiring the deposition of such an abstract in the registry 24 months after closure of data collection if results are not published in a peer-reviewed venue by that time. June 2007 BMJ 2007;334:1080 Copyright ©2007 BMJ Publishing Group Ltd. Summary (1) • Left to its own devices research will not advance • • • • the welfare of people Blind repetition of worn ways of doing things inevitably invites disaster What we have learnt is the need for collaboration and sharing Registration represents one way of creating openness in science Responsible research is a collective culture Summary (2) • Ethics and regulations always lag behind technology • Biological agents and in particular humanised agents require a new paradigm for testing • Animal testing may be limited in value Thank you!