UNICEF- Update on key activities
advertisement

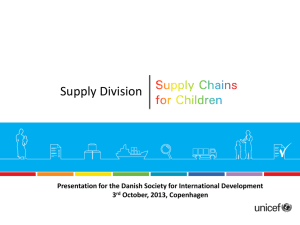
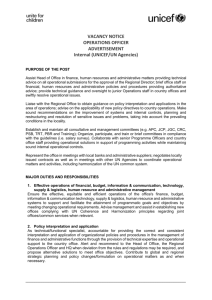
UNICEF- Update on key activities IPC Meeting Geneva, 10-11 December 2015 • • Technical report providing most recent country, regional and global estimates on child mortality United Nations Inter-agency Group for Child Mortality Estimation • • • • • 4th annual report Includes more in-depth analysis on mortality Includes coverage of interventions Projections to 2030 UNICEF Where under-five deaths are occurring: The highest under-five mortality rates are in sub-Saharan Africa • In Sub-Saharan Africa 1 in 12 die before age 5, in high income countries 1 in 147 die before age 5; Sub-Saharan Africa and South Asia account for more than 80% global under-five deaths Under-five mortality rate and under-five deaths by country, 2015 Source: UN Inter-agency Group for Child Mortality Estimation (UN IGME) 2015 Who is most at risk Children from poor, rural or low-maternal-education households are much more likely die before age five • Mothers with no education vs secondary education: 2.8 times • Poorest vs richest: 1.9 times as likely to die before the age of 5 as richest • Rural vs urban: 1.7 times Under-five mortality rate by mother's education, wealth and residence, 2005-2010 Source: UNICEF analysis based on Demographic and Health Surveys, Multiple Indicator Cluster Surveys and other nationally representative sources Why and when under-five deaths occur Most under-five deaths are still caused by diseases that are preventable or treatable Pneumonia, diarrhoea and malaria are main killers of children under age 5; preterm birth and intrapartum-related complications are responsible for the majority of neonatal deaths Global distribution of deaths among children under age 5 and among newborns, by cause, 2015 Source: WHO and maternal and Child Epidemiology Estimation Group (MCEE) provisional estimates 2015 • The world has achieved tremendous progress in reducing child mortality • Promisingly, progress has accelerated in recent years, especially in some of the most challenging contexts • However, progress is not enough to meet the MDG 4 target of a two-third reduction in the under-five mortality rate between 1990 and 2015 • Most under-five deaths are still caused by diseases that are readily preventable or treatable with proven, cost-effective interventions • The remaining burden of child mortality is not evenly shared among or within countries • Addressing the sources of inequity that persist in many contexts will be key to achieve further progress • We know what needs to be done to address under-five mortality. Millions of lives can be saved if we all work together. • As we look ahead to the SDGs, and the roll-out of the SG’s Global Strategy 2.0, the lessons of successes and shortcomings send a clear message: we can shape the future we want for the world’s children. UNICEF Health Strategy 2015-2030 Convention on the Rights of the Child (CRC) Convention on the Elimination of all Forms of Discrimination against Women (CEDAW) Sustainable Development Goals (SDGs or “global goals”) Every Woman Every Child Global Strategy (EWEC or Global Strategy 2.0) 2015-2030 Strategy Approaches to be included in UNICEF program areas Approaches Equity in health outcomes Definition • Identifying marginalized groups in all contexts who may have below-average outcomes by looking at disaggregated country data • Identifying and removing bottlenecks that prevent equitable outcomes • Enhancing Policies, Strategies, Plans, Financing and Budgets (Focus on equity using evidence) Health system strengthening • Improving Decentralized Management Capacity including emergency (Evidence-based planning, budgeting and monitoring) preparedness and resilience • Strengthening Community Platform (Demand generation, Social Accountability, Service delivery, Social inclusion and reduction of financing barriers) Integrated, multisectoral policies and programs • Developing shared goals / targets / planning across program areas and within program areas internally to health section, as well as with other sectors within UNICEF • Promoting health as a platform for delivery of multi-sector packages of interventions and services • Chlorhexidine: utilization expanding Over 28 countries in various stages of engagement in Africa and Asia Focus on promotion of introduction in practice and support scale up (formative research, regulation, demand, local manufacturing) Credit: Chlorhexidine Working Group 2015 10 Challenges in access of chlorhexidine Solution and gel available – Markets for each formulation is evolving Limited sources – But manufacturing base increasing (Nepal, India, Bangladesh, Nigeria, Ethiopia, Kenya…) New products under development (sachets) Require appropriate messaging to mothers and other caregivers to ensure proper product use through: ─ ─ ─ Appropriate product labeling, Context appropriate product presentation Proper messaging to mothers and other caregivers to ensure proper product use. 11 Credit: Chlorhexidine Working Group 2015 (please confirm) • Chlorhexidine Working Group An international collaboration of organizations committed to advancing the use of 7.1% chlorhexidine digluconate for umbilical cord care – Advocacy – Technical assistance Supports activities in over 25 countries and coordinates global efforts including development of evidence and guidance to programmes and industry Active participation of industry More info: www.healthynewbornnetwork.org/topic/chlorhexidine-umbilical-cord-care Copenhagen, Denmark 23-26 November 2015 12 PNEUMONIA • Currently, ~3 in 4 childhood pneumonia cases around the world do not receive treatment……and ~80% of this need occurs in just 10 countries 55M untreated pneumonia cases in children under five occur… 100% 27M cases 80% 60% 99M cases 55M cases 40% 20% 16M cases 0% Cases in top 50 countries Treated cases … in these 10 countries (in order of untreated cases) 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. India Nigeria Pakistan Bangladesh DRC Ethiopia Tanzania Afghanistan Uganda, and Kenya Untreated cases in top Untreated cases in 10 countries remaining 40 countries Source: BMGF, R4D and USAID. “The Growing Market for Amoxicillin Dispersible Tablets: Opportunity Assessment for Potential Manufacturers.” September 2014. Copenhagen, Denmark 23-26 November 2015 13 • Use of amoxicillin DT for pneumonia is growing Annual orders for Amoxicillin DT through UNICEF have grown 13x since 2011 Need for scale-up supply of quality assured amoxicillin DT to meet demand arising from new guidance for managing pneumonia UNICEF started procuring amoxicillin DT in 2011. Activities under the work UNCLSC encouraged engagement of new manufactures and increase in availability. An ERP was established in 2013: 11 Manufacturers engaged in the ERP Need more suppliers Copenhagen, Denmark 23-26 November 2015 14 • Potential global demand is expected to continue to grow, with up to ~4.1B amox DT needed over the next 5 years Global annual amox DT demand could grow from ~300M tablets in 2015 to ~1.2B in 2020 Amox DT (M) 1200 1,162 High Medium 1000 937 800 740 718 570 600 594 425 484 400 293 200 387 303 247 0 2015 2016 2017 2018 2019 2020 Note: R4D analysis based on 50 country childhood pneumonia antibiotic forecast prepared by John Snow, Inc; includes public and private sectors Copenhagen, Denmark 23-26 November 2015 15 • Country-level product registration is important as regulatory conditions in key growth markets are increasingly enabling amox DT scale-up Source: Diarrhea and Pneumonia Working Group. “Country Update Summary.” May 2015. Copenhagen, Denmark 23-26 November 2015 16 SCALE-UP IS LINKED TO APPROPRIATE DIAGNOSIS ARIDA (Acute Respiratory Infection Diagnostic Aid) Project: • Launched by UNICEF, multistakeholder project to develop a respiratory rate measuring device for diagnosis of pneumonia by health workers. www.unicef.org/innovation Pneumonia Diagnostics Project • Malaria Consortium. Multi-country field trial of several new diagnostic tools Copenhagen, Denmark 26 November 2015 23- 17 … AND APPROPRIATE USE PATH and UNICEF piloting use of dispensing aids Aimed at dispensing by community health workers (CHW) and primary health settings. 18 COLLABORATION WITH WHO ON ANTIHELMINTICS Changes in target for albendazole and mebendazole WHO: Donation programme with GSK and J&J for LF and deworming in school age children UNICEF and INGO: Procurement for deworming in pre-school age children Coverage for school age children to increase from 250M (40%) in 2013 to 550M (75%) in 2020 Coverage for pre-school age children (PSAC) expected to increase from 130M children (49%) in 2013 to 270M children (75%) n 2020 Copenhagen, Denmark 23-26 November 2015 19 Preventive chemoprophylaxis of soil-transmitted helminthiasis : Challenges Many products in the market and varied standards of quality Included in the WHO prequalification programme under the EOI for Neglected Tropical Diseases Single ingredient medicines to treat lymphatic filariasis, soil-transmitted helminthiasis (STH), and schistosomiasis - Diethylcarbamazine citrate 100mg tablet (scored) - Mebendazole 500mg tablet (chewable*) - Albendazole 400mg tablet (chewable*, preferably scored) - Praziquantel 600mg tablet (scored) - Ivermectin 3mg tablet (unscored) Limited number of dossiers submitted for PQ – Expert Review Process established to provide interim assessment of quality. * can be chewed or swallowed whole 20 Preventive chemoprophylaxis of soil-transmitted helminthiasis: Progress In 2015, WHO and UNICEF reaffirmed commitment to procure quality products and called on manufacturers to submit dossiers for ERP and international buyers to use results for qualification: – Albendazole- 11 manufacturers engaged – Mebendazole- 2 manufacturers engaged Significant efforts from manufacturers to complete requirements for dossier evaluation Concurrent review of Pharmacopoeia Monographs – Albendazole: revised monograph in IP 5th Edition (2015) to include dissolution criteria and labelling – Mebendazole: under review Copenhagen, Denmark 23-26 November 2015 21 Supply Constrains Case Study – IPV • • • • • • Ambitious agenda to introduce IPV in 126 OPV-using countries within 1.5 years in time for the global OPV2 withdrawal At time of IPV planning, about 68 high and middle-income countries were using IPV 2014 UNICEF issued a tender for stand-alone IPV in line with Endgame Strategy Procurement objective to ensure sufficient supply for 1 dose of IPV at an affordable price to meet demand 2 manufacturers awarded, 1 pipeline Awarded quantities and near term bulk and filled product manufacturing capacity anticipated to be sufficient to meet planned and some unplanned demand • Demand for India and 20 L/MICs included Case Study – IPV (2) • Expected scale up of IPV unprecedented compared to other new vaccine introduction programs • Since awards major changes in supply availability • 2014-2015 supply reduced from 129 mds to 63 mds • 2016 supply reduced from awarded 121 mds to expected 77 mds • At same time, significant increases in demand • India requiring 28 million doses for 12 month catalytic support from GPEI • Catalytic support to 25 countries as approved by Polio Oversight Board (POB) • Increased demand for routine immunization (to date 1.2 million doses – more required?) • SIA requirements of 8.7 million doses of IPV delivered, global stocks of 1.2 million doses set aside for SIAs - more required for post switch outbreak response Case Study – IPV (3) Mitigation actions • Consultations to establish criteria for allocation of constrained supply • No other suppliers in pipeline in near term, therefore, mitigating actions focused on managing supply that was available in line with programmatic priorities • Close and ongoing coordination with WHO and GPEI partners to establish supply prioritization criteria • Depending on prioritization of country, a number of countries required to delay introductions • Effort by WHO and PQT to approve MDVP to IPV to increase doses available • Tight management of supply including delivery of buffer stocks, daily monitoring of stock levels and preparation of supply and demand scenarios Supply Constrains- Other products? AQ+SP for Seasonal Malaria Chemoprophylaxis • • • • Plans in 2015 disrupted due to quality issues Plans for 2016 total so far around 60M treatments. Capacity can only fulfill by August- too late for campaigns Need to monitor availability and coordinate delivery with countries through Malaria Consortium, CAMEG (WB), UNICEF, USAID, GF and MSF. A role for WHO GMP? Work in Emergencies Participation in WHO-WFP Global Supply Chain For Pandemic Preparedness & Response project UNICEF is including Health Emergencies in its programme: • Define disease specific contingency items, stock quantities and procurement approach • Update ESL/CCCs/SSOPs • Support Country office preparedness • Incorporate health emergency/IPC expertise in surge rosters • Develop communication materials for effective knowledge management • Financing mechanisms for Supply component of response IEHK update of Malaria and PEP modules- Consultancy to develop guidance on selection and procurement of supplies for sexual assault (PEP kit, additional modules) Financing A look back… 4 – 5 years ago, we began a body of work in financing, initially focusing on transactional activities: - Delayed funds which prevented supply transactions moving forward - Financial backing for special contracts to generate exceptional savings But it’s organically grown to adjacent activities and has become quite robust. Here are some highlights: 2010 • Inaugural formalized pre-financing transactions • Sierra Leone $6.7m LLINs thru 7% set-aside fund: Zambia: $4.4m LLINs (delayed WB loan) thru LoC; 2011 • Novartis OPV Firm Contract – Kept a supplier in a constrained market for 2 extra years • Rotavirus special contracting with partners $650m of savings over 5 years 2012 • First U.S. Fund’s Bridge Fund transactions ($500k RUTF Burkina Faso) • First ‘partial firm’ transaction (Sanofi OPV); high returns / efficient capital 2013 • $54m worth of pre-financings for COs and Countries, including polio transactions for Nigeria and Pakistan • Special contracting to secure IPV supply via VII; special contracting for penta via GAVI/BMGF 2014 • ~$30m of pre-financings for COs and Countries, including Ebola-related; VII transition to SD • UNICEF-led penta special contracting, novel option + commercial financing design $57m in savings 2015 • VII Expansion ExB Approval; ~$50m worth of pre-financings YTD; Nigeria RI credit line • Launch of domestic supplier base expansion / financing activities Current Scope: 2014-2017 To respond to these needs, we‘ve conducted activities through 4 workstreams: Impact on Countries Pre-Financing Delayed Grants and MoH Budgets • ~$50m worth of transactions pre-financed in 2015YTD • VII Expansion & USF’s Bridge Fund related to PS • Nigeria $21m credit line for Routine Immunization Increasing Gov’t Fiscal Space • Support country-owned budgeting and sustainability initiatives • Facilitate implementation of local public-private trust funds; access to commercial markets Country Financing Special Contracting • Penta Special Contracting $57m+ savings over 2 years (MICs-GAVI price parity) • Additional models to achieve “firm” contracts including multiple partial-firm models, optionbased models Local Supplier Base Development • Support access of new suppliers in programme countries to financing via leveraging UNICEF’s network, convening ability and credit profile Supply Financing Addressing cash flow timing gaps Increasing availability of funds / budgets Lower prices, secured quantities, etc. Lower prices + domestic economic development Current Trends in Supply Financing Pre-financing need for delayed grants and government disbursements • $100m annual supply pre-financing requests (all commodities); $225m+ by 2020 Expanding pre-financing activities –2015YTD (July) ~$50M worth of pre-financings (~½ through VII) / Worth noting that since its inception the US Fund’s Bridge Fund in 2012 has supported $100M of pre-financings and government related PS activities. Vaccine Independence Initiative– expanding scope and capital base per Executive Board approval in 2015 • Active: Kenya, Chad, Niger, Capo Verde, PICs, Nigeria: Soon active: Lao PDR, Cameroon, Ghana • By end 2015, capital fund’s effective base will increase from $10M to $30M (including most recently $5m from GAVI). Target is $100M by 2020. Special contracting to achieve improved pricing for countries • MICs-GAVI penta pricing parity + $57m savings • Improved pricing increased fiscal space for other interventions Cost-effective / less capital-intensive special contracting mechanisms Sourcing of supplies from programme countries • Domestic suppliers’ poor access to affordable financing • RMNCAH-commodities to be locally sourced by Countries Support domestic supplier growth while respecting FRRs and public procurement principles The HUB “Strengthening in-county immunization supply chains for all” Three strategic pillars New cEVM Expanding the EVM to a fully revamped process and comprehensive toolkit for countries to diagnose, prioritize, plan and implement change for their immunization supply chain improvements, aligned with priorities from GAVI Strategy iSCL focus topics Take the lead on developing new evidence, tools and guidance on a selected number of high-priority iSCL topics – starting with cold chain management as the first priority topic Community of practitioners Strengthen coordination and build a community of skilled practitioners at the global, regional and country level Center of excellence for iSCL iSCL Hub Coordinator of technical assistance to countries Immunization: Data for Management Toolkit • Guidance on Dashboards for Immunization Supply Chain (DISC) – Advocacy piece: describes dashboards and benefits – Planning and using dashboards: suggests steps in planning & implementation, suggests continuous improvement activities • Standardized primary key indicators: detailed reference sheets including visualization and action examples • Case studies around use of dashboards: – Nigeria – Mozambique – India • Material to support country-level policy advocacy • ViVa GF-UNICEF Coorperation: Country level implementation • • Country dialogue led by GFATM Fund Portfolio Managers (FPMs) and Country Co-ordinating Mechanisms (CCMs) 19 concept notes have been submitted where RMNCH has been integrated to varying degrees, and these countries are now moving into the grant making phase iCCM/Malaria(Child Health) MNCH/HIV (Maternal Health) Burkina Faso (Malaria and HSS) Nigeria Chad Comoros Rwanda DRC Cote d’ivoire South Sudan Tanzania DRC Uganda (Malaria) Uganda Ethiopia Zambia Zambia Ghana Senegal Mozambique Sudan Concept note phase • Quantification of both GF and non GF commodities • Gap analysis to identify funding gaps for iCCM commodities • High level SC activities Grant making phase • Supply planning • SC capacity assessment • SC implementation mapping • Supply chain (PSM) plan At each point there a requirement for joint planning for all the commodities – responsibilities and accountabilities for implementation and monitoring need to be agreed at country level Nutrition supply chain strengthening HERA report Food for Peace Supporting governments in optimization and/or integration of the RUTF into national Supply Chain Management. • End-to-end nSC health checks / assessments to identify performance gaps/bottlenecks. • Development of supply chain improvement plans and support in implementing those plans. • Development of guidelines and tools for nutrition supply chain performance monitoring for governments. • Development and dissemination of simple nutrition commodities quality guidelines along the supply chain. Technical Assistance to governments in strengthening nutrition supply chains, end to end (planning, forecasting, pipeline management, warehousing, distribution, end use monitoring and visibility) UNICEF Strategic Framework on Environmental Sustainability for Children 2016 - 2017 Priority 1. Strengthen UNICEF policy and guidance on environmental sustainability as a cross-cutting issue. Priority 2. Strengthen the inclusion of environmental sustainability in UNICEF programmes. Priority 3. Advocate for full recognition and inclusion of children in the policy discourse on environmental sustainability. Priority 4. Strengthen opportunities for children’s development and wellbeing to benefit from environmental sustainability related public and private finance. Priority 5. Incorporating environmental sustainability management (ESM) in the organization