Retinopathy of Premarurity
advertisement

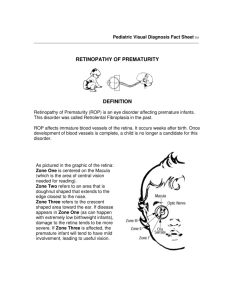
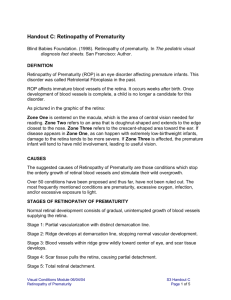
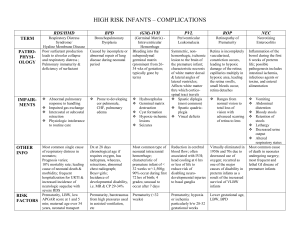
Retinopathy of Prematurity Region 2 Michelle Kirby, Tracie Jenness, Debbie Minshew What is Retinopathy of Prematurity? Retinopathy of Prematurity is an eye disorder that primarily effects premature infants of low birth weight and is the leading cause of vision loss in children. Laura Maikata What parts of the eye are effected? ROP causes unnatural growth and development of the veins in the retina. In advanced stages, a ridge is formed on the retina where the veins can spread and begin to grow into the vitreous humor. This abnormal growth can eventually detach the retina, causing partial and even full vision loss. geteyesmart.org What Causes ROP? The reason why retinal vessels begin to grow abnormally in preterm babies is still largely unknown. In the 1950’s it was discovered that an increase in oxygen levels used to incubate preterm babies played a major factor in developing ROP. Some modern research has been done that suggest the lack of certain growth hormones that were being received in utero might also be one of the leading factors. Typical eye development and preterm ROP development What Causes ROP? The blood vessels in a baby’s eyes begin developing at 3 months gestation. Blood vessels begin to develop in the macula of the retina. If born during vascularization, a demarcation line typically occurs and the vessels may stop growing. Between 28-40 weeks there is rapid vascularization of the retina. The blood vessels in the retina grow rapidly, branching out toward the periphery. The blood vessels in the retina are extremely sensitive and fragile, abnormal growth may occur. Blood vessels in the retina may begin to grow into the vitreous humor, pulling the retina inward which could cause retinal detachment. Vascularization is completely developed Normal visual function develops and acuity strengthens. ROP becomes more stable, but is still monitored annually for complications. Risk Factors • Any baby born before 30 weeks gestation • Low birth weight • Any other symptoms that can cause low birth weight or premature births such as: • • • Anemia Blood transfusions Respiratory disease • In the past, too much oxygen was used in incubation of preterm babies and caused the vessels of the retina to grow abnormally. • Today, oxygen levels are better monitored and all baby born before 30 weeks or under 3 pounds are screened for ROP. Stages and Classification of ROP ROP has five stages of development with 1 being the least effected, to 5 being the most severely effected. The area of the retina that is effected is also classified into three zones which measures how far the disease is progressing into the retina. Stage 1 In stage 1 ROP, there is a line or demarcation between the vascularized portion of the retina. This is the mildest form of ROP and will usually spontaneously begin to develop normally, needing no treatment. Stage 2 In stage 2, the demarcation line develops a ridge of tissue. This is considered a moderate form of ROP and will be monitored closely. At this stage, normal develop can still occur, or there may be a worsening of the condition. Stage 3 • In the third stage of ROP, the veins begin to pile up on the ridge created on the retina and begin to branch out into the vitreous humor. Stage 3 is classified further as mild, moderate to sever depending on the amount of scar tissue developed at the ridge. Earl Palmer, M.D., Oregon Health Sciences University Stage 4 4A In stage 4, the scar tissue that developed in the previous stages is now pulling the retina and causing detachment. Stage 4 is classified as 4A and 4B. In stage 4A, the retina has begun to detach in zones 2 and 3, causing peripheral vision loss. In stage 4B, the detachment has entered into the macula causing more severe central vision loss. Cybersight 4B Stage 5 Stage 5 is a complete detachment of the retina. The retina takes on a funnel shape connecting from the optic nerve to the front of the eye. At this stage, vision cannot be restored and blindness occurs. Cybersight Plus Disease Plus disease is a more aggressive form of ROP and a sign of rapid development of the disease. Plus disease can become present at any stage of ROP. In plus disease, the blood vessels are growing at a rate that they become engorged and twisted. Infants with plus disease will most likely need treatment. Oculist Stages Stages Eye Condition Prognosis 1 Blood vessel growth is mildly abnormal No treatment, normal vision will develop 2 Moderately abnormal blood vessel growth Most children will need no treatment and normal vision will develop 3 Severely abnormal growth of blood vessels mostly toward the center of the retina, some vessels becoming enlarged and twisted In some children, vision will resolve with no treatment, with more severe vessel abnormalities, called “plus disease,” treatment can prevent retinal detachment, but there is a loss of peripheral vision. 4 Partially detached retina If no treatment, partial vision loss 5 Fully detached retina If there is no treatment, can lead to blindness Effects on the visual system Most children diagnosed with ROP begin to have normal vascular growth and typical vision develops. However, children with Retinopathy of Prematurity will more than likely develop acuity problems and in advanced cases, ROP can also cause partial field loss to a total loss of functional vision. http://www.cs.utah.edu/research/groups/percept/ DEVA/images/vissim-lab-central-field-loss.jpg Treatments In majority of babies diagnosed with ROP, the blood vessels will heal within the first 4 months of life and no treatment will be needed. However, more advanced stages of ROP will require treatment to halt the growth of the destructive blood vessel growth, partial or full reattachment of the retina, and remove scar tissue. serviceartist.net The most common treatment for ROP is laser therapy or cryotherapy. Photocoagulation, or laser therapy, uses a diode laser mounted on an ophthalmoscope to create tiny laser burns in the periphery of the retina to prevent further abnormal vessel growth. AAPOS Cryotherapy Cryotherapy, uses a pen-like instrument called a cryroprobe to freeze the periphery of the retina through the eyes outer wall. Cryotherapy has been largely replaced by laser therapy. However, it is still used if retina cannot be fully seen. http://salemretina.com/info/treatment/las er_and_cryotherapy/ Both of these treatments cause field vision loss because it destroys parts of the retina. The main goal in treatment is to preserve the macula and the central portion of the retina for optimal functional vision. If the child’s retina become severely detached, surgery might also be recommended. Scleral buckling is sometimes used to help push the retina into the back of the eye. This is done by placing a silicone band around the eye. Jimpitch.com Vitrectomy Vitrectomy is another surgery that can be done in which the vitreus is removed in order to remove scar tissue, The eye is then filled vith saline so the retina can flatten back out against the wall of the eye. http://www.oneclearvision.org/treat ment-for-eye-floaters/surgicalvitrectomy/ Outcomes Retinopathy of Prematurity can be extremely progressive during the 28-40 weeks of vascularization. After the blood vessels are fully formed, the disease becomes more stable. There is however a risk of further complications developing later in life such as glaucoma and cataracts. There is also an increased risk of developing strabismus and amblyopia along with acuity issues, especially myopia. Epidemiology There are approximately 3.9 million infants born in the U.S. each year. About 14,000 are affected by ROP and 90% of those affected have only mild disease. About 1,100- 1,500 develop disease severe enough to require medical treatment and 400-600 infants each year in the U.S. become legally blind from ROP. (AAPOS, 2013) Preformingsongwriter.com Resources • American Association for Pediatric Ophthalmology and Strabismus (July 2013). Retinopathy of Prematurity. Retrieved from http://www.aapos.org/terms/conditions/94 • Griggs, Paul B. MD. (July 2013). Retinopathy of Prematurity. National Library of Medicine. MedlinePlus. Retrieved from http://www.nlm.nih.gov/medlineplus/ency/article/001618.htm • Hartnet, M. Elizabeth MD(November, December 2004). Managing Retinopathy of Prematurity. American Academy of Ophthomology. EyeNet Magazine. Retrieved from http://www.aao.org/publications/eyenet/200411/pearls.cfm • Hartree, Niomi MD, Scott, Oliver MD (17/09/10). Retinopathy of Prematurity. Patient.co.uk. Retrieved from http://www.patient.co.uk/doctor/Retinopathy-of-Prematurity-(Retrolental-Fibroplasia).htm • Johnston, Suzan MD (2011). Retinopathy of Prematurity (ROP). Boston Children’s Hospital. Kids MD Health Topics: Our Health Topics. Retrieved from http://www.childrenshospital.org/health-topics/conditions/retinopathy-of-prematurity-rop • National Eye Institute (June 2014) Facts about Retinopathy of Prematurity (ROP). Retrieved from http://www.nei.nih.gov/health/rop/rop.asp Case Study Click here to open Fact Sheet Additional Resources click here to open