4_Immune-response-disorders
advertisement

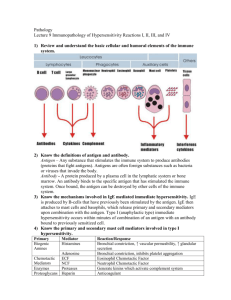
Disorders of the Immune System Four Major Categories of Immune Mechanisms • Humoral or antibody-mediated immunity • (B lymphocytes) • Cell-mediated immunity • (T lymphocytes) • Complement system • Phagocytosis • (neutrophils and macrophages) Types of immune defenses – Innate, or nonspecific immunity: the natural resistance with which a person is born – Adaptive, or specific immunity: the second line of defense, responding less rapidly than innate immunity but more effectively Innate Immunity • Components – Epithelial barriers – Phagocytic cells • Neutrophils and macrophages – Natural killer cells – Plasma proteins – Opsonins, cytokines, and acute-phase proteins • Induction of inflammatory response • Red, Heat, Edema, Pain, Pus Adaptive Immunity • Able to recognize and react to a large number of microbes and non-microbial substances • Ability to distinguish among different, even closely related, microbes and molecules and to “remember” the pathogen by quickly producing a heightened immune response on subsequent encounters • Lymphocytes and their products • Antigenic identification Types of Adaptive Immune Responses • Humoral immunity – Mediated by molecules in the blood – B Cells secrete antibodies – The principal defense against extracellular microbes and toxins • Cell-mediated immunity, or cellular immunity – Mediated by specific T lymphocytes – Defends against intracellular microbes such as viruses Histocompatibility Complex • Major histocompatibility complex (MHC) – Set of molecules displayed on cell surfaces • Lymphocyte recognition • Antigen presentation – Control the immune response through recognition of self and nonself Properties of MHC Molecules • HLA antigens – Class I: HLA-A, HLA-B, HLA-C – Class II: HLA-DR, HLA-DP, HLA-DQ • Distribution – Class I: virtually all nucleated cells – Class II: restricted to immune cells, antigenpresenting cells, B cells, and macrophages Properties of MHC Molecules (cont.) • Functions – Class I: present processed antigen to cytotoxic CD8+ T cells – Class II: present processed antigenic fragments to CD4+ T cells; necessary for effective interaction among immune cells Antigen Presentation • Macrophages and dendritic cells process and present antigen peptides to CD4+ helper T cells • Capture antigens and then enable their recognition by T cells • Initiation of adaptive immunity Immunodeficiency States Immunodeficiency Disorders • Abnormality in the immune system that renders a person susceptible to diseases Classifications of Immunodeficiency States Primary (congenital or inherited) Secondary (acquired later in life) Malnutrition Infection (e.g., AIDS) Neoplastic disease (e.g., lymphoma) Immunosuppressive therapy (e.g., corticosteroids or transplant rejection medications) Results of Alterations of the Immune System • Immunodeficiency states • Allergic or hypersensitivity reactions • Transplantation rejection • Autoimmune disorders Deficiencies of Antibody (B Cell) Immunity • B-cell function and immunoglobulin or antibody production are involved. • Defects in humoral immunity increase the risk of recurrent pyogenic (bacterial infections that make pus) infections. • Humoral immunity usually is not as important in defending against intracellular bacteria (mycobacteria), fungi, and protozoa. • Viruses usually handled normally, except for the enteroviruses that cause gastrointestinal infections Deficiencies of Antibody (B Cell) Immunity • Genetic disorders of the B lymphocytes • Approximately 70% of primary immunodeficiencies • Immunoglobulin production depends on – The differentiation of stem cells to mature B lymphocytes – The generation of immunoglobulin-producing plasma cells • Can interrupt the production of one or all of the immunoglobulins Deficiencies of Antibody (B Cell) Immunity X-Linked Agammaglobulinemia • • • • Recessive trait that affects only boys No immunoglobulins Susceptible to many diseases Gene necessary for pre-B-cell expansion is missing • Become symptomatic around 6-9 months of age Symptoms include Frequent episodes of • Chronic Diarrhea • Conjuctivits • Chronic Otitis Media • Pneumonia • Bronchitis • Upper Respiratory Tract Infections Deficiencies of Antibody (B Cell) Immunity Selective Immunoglobulin A Deficiency • Most common type – Affects 1 in 400 persons • Moderate reduction of IgA levels – Found in mucous, tears, saliva • In both men and women Deficiencies of Antibody (B Cell) Immunity Selective Immunoglobulin A Deficiency • Less harmful than many other immunodeficiency diseases • 2/3rd have no symptoms • Symptoms include frequent episodes of: Bronchitis, chronic diarrhea, conjuctivis, otitis media, pneumonia, upper respiratory tract infections • No treatment Deficiencies of Cell-Mediated (T-cell) Immunodeficiency DiGeorge Syndrome • 22q11.2 deletion syndrome • Partial or complete failure to develop the thymus and parathyroid glands • Many different problems can occur from this due to lack of T-cell production • Outward appearance changed – Low-set ears, hypoplastic mandible bowing upward lip 22q11.2 deletion syndrome Signs and symptoms may include some combination of the following: • • • • • • • Bluish skin due to poor circulation of oxygen-rich blood (cyanosis) Weakness or tiring easily Failure to thrive Failure to gain weight Poor muscle tone Shortness of breath Delayed development, such as delays in rolling over, sitting up or other infant milestones • Delayed speech developmentLearning delays or difficulties • A gap in the roof of the mouth (cleft palate) or other problems with the palate • Certain facial features, such as low-set ears, wide-set eyes or a narrow groove in the upper lip 22q11.2 deletion syndrome Combined T-Cell and B-Cell Immunodeficiencies • Severe combined immunodeficiency (SCID) – X-linked SCID • Absence of all T and B-cell function (maybe NK cells as well) • Disease resembles AIDS in infants – Bubble boy disease David Vetter -Lived in a Bubble up to the age of 12yrs. -Was given a bone marrow transplant from his sister -She had EpsteinBarr virus dormant in her bone marrow -He contracted Burkitt’s Lymphoma and died in two weeks Wiskott-Aldrich Syndrome • Rare X-linked disorder • Both B and T cell immunity is impaired • Complete failure to produce antibodies to an entire class of antigens, namely polysaccharides – Recurrent infections – Hemorrhages secondary to thrombocytopenia – Eczema – Petechiae – Infections (otitis media) Wiskott-Aldrich Syndrome • Clinical Features – Infections from opportunistic organisms • Pneumocystitis carnii and Candida albicans – Some die from disseminated herpes simplex and varicella • Bone transplants seem to be very effective in this syndrome Complement System • The following are the basic functions of the complement: • Opsonization - enhancing phagocytosis of antigens • Chemotaxis - attracting macrophages and neutrophils • Lysis - rupturing membranes of foreign cells • Clumping of antigen-bearing agents Disorders of the Complement System • Primary – Mostly transmitted as autosomal-recessive traits and can involve one or more complement components • Secondary – Can occur in persons with functionally normal complement – Caused by • Diabetes mellitus • Leukemia • Immunosuppressive drugs Hereditary angioedema Inhibition of C1 protein in the complement system Autosomal Dominant http://www.youtube.c om/watch?v=ualR2rCZ -J8 The Phagocytic System • Definition: Composed primarily of polymorphonuclear leukocytes and mononuclear phagocytes • Action of these cells – – – – Migrate to the site of infection Aggregate around the affected tissue Envelope invading microorganisms Generate microbicidal substances to kill the ingested pathogens http://www.youtube.com/watch? v=KxTYyNEbVU4&feature=related Dysfunction of the Phagocytic System • A defect in phagocytic functions or a reduction in the absolute number of available cells disrupt the system • Susceptible to: – Candida species – Filamentous (thread-like) fungi • Chronic granulomatous disease (CGD) – Symptoms are: • Impetigo • Recurrent Pneumonia • Skin and rectal abscesses Impetigo http://www.youtube.com/watch?v=mUcE1Y_bOQE&featu re=related Stem Cell Transplantation • Many primary immunodeficiency disorders traced to deficient stem cells can be cured with allogeneic stem cell transplantation from an unaffected donor. – SCID, Wiskott-Aldrich syndrome, and chronic granulomatous disease • Stem cells can repopulate the bone marrow and re-establish hematopoiesis. – Taken from bone marrow, blood or umbilical cord of donor • To be effective, the bone marrow cells of the host are destroyed by myeloablative doses of chemotherapy. Introduction • Normal immune reactions do their job without hurting the host. • Sometimes, immune reactions can be excessive, resulting in disease. • People who mount normal immune responses are sensitized to that antigen. • People who have excessive responses are hypersensitive. What happens in these reactions? • The immune response is triggered and maintained inappropriately. • Hard to eliminate stimulus! • Hard to stop response once it starts! • …so hypersensitivity diseases are often chronic, debilitating, hard to treat. Hypersensitivity Reactions Outline • Introduction • Type I Hypersensitivity Type I Hypersensitivity Disorder • Also known as Immediate Hypersensitivity • First Exposure – Antigen is presented to B and T cells – IgE antibodies are produced and bind to Mast Cells – Mast cells are primed for the second exposure – Upon second exposure mast cells degranulate – End result: vessels dilate, smooth muscle contracts, inflammation persists What do mast cells release upon Second Exposure? • Granule contents • Histamine • Some chemotactic factors • Membrane phospholipid metabolites • Prostaglandin D2 • Leukotrienes • Cytokines • TNF • Interleukins • IL-13 Mast cells: Normal (left) and degranulated (right) What do these substances do? • Act on blood vessels, smooth muscle, and WBCs. • Immediate response (minutes) • vasodilation, vascular leakage, smooth muscle spasm • granule contents, prostaglandin, leukotrienes • Late phase reaction (hours) • inflammation, tissue destruction • cytokines What happens to the patient? • Local reactions • Skin: itching, hives • GI: diarrhea • Lung: bronchoconstriction • Anaphylaxis – Wide spread edema due to Histamine » Vascular leakage • Itching, hives, erythema • Constriction of bronchioles, wheezing • Laryngeal edema, hoarseness, obstruction • Shock • DEATH Hypersensitivity Disorders • Type I – Allergies – Asthma – Hay Fever Hypersensitivity Reactions Outline • Introduction • Type I Hypersensitivity • Type II Hypersensitivity Type II • Cytotoxic Hypersensitivity • Action – An antibody attaches directly to an antigen in the target tissue, usually a cell membrane – Mediated by IgG or IgM antibodies Type II Hypersensitivity • ANTIBODIES • “Antibody-mediated” hypersensitivity • Antibodies bind to antigens on cell surface • Macrophages eat up cells, complement gets activated, inflammation comes in • End result: cells die, inflammation harms tissue Which diseases involve type II hypersensitivity? Disease Antigen Symptoms Autoimmune hemolytic anemia RBC antigens, drugs Hemolysis Pemphigus vulgaris Goodpasture syndrome Myasthenia gravis Graves disease Proteins between epithelial cells Proteins in glomeruli and alveoli Acetylcholine receptor TSH receptor Bullae Nephritis, lung hemorrhage Muscle weakness Hyperthyroidism Sequence of Events • Antibodies bind to cell-surface antigens • One of three things happens: • Opsonization and phagocytosis • Inflammation • Cellular dysfunction Opsonization and Phagocytosis Inflammation Cellular Dysfunction Graves disease Myasthenia gravis Type II • Two Types of cytotoxic reactions occur – Direct • The target cell is coated by antibodies and macrophage destroy it. • Complement can be used to destroy the cell • Lysis is mediated by complement by opsonization • An example is autoimmune hemolytic anemia Type II • Indirect – IgG antibodies bind to target-cell membrane receptors and block receptor function • An example is myasthenia gravis Type II – Cytotoxic Hypersentivity • Other Examples – Graves’ Disease – Erythroblastosis Fetalis – Idiopathic Thrombocytopenic Purpura Mechanisms of Autoimmune Disease • Heredity and gender specific • Failure of self-tolerance – Disorders in MHC–antigen complex/receptor interactions – Molecular mimicry – Super-antigens Heredity • Certain HLA types seem to inherit certain autoimmune diseases – 90% of patients with ankylosing spondilitis have HLA-B27 antigen • Only 7% without the disease have the antigen • May be a “trigger event” that precipitates the altered immune state – Like stress Mechanisms Postulated to Explain Immunologic Tolerance • Self-tolerance: Differentiate self from non-self –HLA antigens encoded by MHC genes are used as markers Failure of Self-Tolerance • Breakdown in T-cell Anergy – Anergy is the unresponsiveness of the immune system to an antigen • Infections , tissue necrosis or inflammation may cause breakdown in Anergy Failure of Self Tolerance • Molecular Mimicry – Many autoimmune diseases are associated with infections • Microbes share an immunologic epitope (part of an antigen molecule to which an antibody attaches itself) with the host • One HLA may bind self-mimicry molecules for presentation to T cells and another’s HLA type may not Failure of Self Tolerance • Superantigens – A family of related substances that can shortcircuit the normal sequence of events in an immune response • Interact with T-cell receptors • Binds to MHC class II molecules leading to activation of T cells – Found in food poisoning, toxic shock syndrome, Streptococcal and Staphylococcal infections Criteria for Determining an Autoimmune Disorder 1.Evidence of an autoimmune reaction 2.Determination that the immunologic findings are not secondary to another condition 3.Lack of other identified causes for the disorder Rheumatoid Arthritis • Autoimmune disease affecting the synovium that lines joints • May begin with low-grade fever, malaise and early morning joint pain and stiffness • Detection of rheumatoid factor in blood test • HLA-B27 Rheumatoid Arthritis Ankylosing Spondylitis • A severe vertebral arthritis – Associated with inflammatory bowel disease and psoriasis – Causes the vertebrae to fuse together • May not even be able to lift your head – Effects men more often than women Scleroderma – Systemic Sclerosis • Connective tissue autoimmune disease – Excessive collagen deposition in the skin and internal organs • ScL-70 antibodies – Includes • Blood vessels • Kidneys • Lungs • Heart • Gastrointestinal tract Other Autoimmune Diseases • Raynaud Phenomenon – Resulting from spasm of small blood vessels that cause coldness, blanching, numbness and pain in finger and toes – Can also occur in internal organs • Polyarteritis Nodosa – Generalized blood vessel inflammation (systemic vasculitis) • 1/3 caused by hepatitis B infection • Associated with inflammation in the vascular wall owing to deposition of immune complexes (type 3 hypersensitivity) • Inflammatory Myopathies – Autoimmune skeletal muscle injury – Occurs alone of in conjunction with other autoimmune diseases such as SLE or RA • Muscle weakness, fatigues, lymphocytic inflammation Hypersensitivity Reactions Outline • Introduction • Type I Hypersensitivity • Type II Hypersensitivity • Type III Hypersensitivity Type III – Immune Complex Hypersensitivity • Immune Complexes – Normal Response – Aggregations of antigen and their corresponding antibodies – Large complexes are formed in a person who has an infection – Carried in the bloodstream • Quickly removed by the liver and spleen • Infection is neutralized or else --• End result: bad inflammation, necrotizing vasculitis Which diseases involve type III hypersensitivity? Disease Systemic lupus erythematosus Post-streptococcal glomerulonephritis Antigen Symptoms Nuclear antigens Nephritis, skin lesions, arthritis… Streptococcal antigen Nephritis Polyarteritis nodosa Hepatitis B antigen Systemic vasculitis Serum sickness Foreign proteins Arthritis, vasculitis, nephritis Arthus reaction Foreign proteins Cutaneous vasculitis Two Kinds of Type III Hypersensitivity Reactions • Systemic immune complex disease • Complexes formed in circulation • Deposited in several organs • Example: serum sickness • Local immune complex disease • Complexes formed at site of antigen injection • Precipitated at injection site • Example: Arthus reaction Serum sickness • In olden days: used horse serum for immunization • Inject foreign protein (antigen) • Antibodies are made; they form complexes with antigens • Complexes lodge in kidney, joints, small vessels • Inflammation causes fever, joint pain, proteinuria Serum sickness – Symptoms: rash, uticaria, exensive edema, and fever – Treatment: corticosteroids and remove allergen Serum sickness Type III – Immune Complex Mediated Hypersensitivity Localized immune complex reactions • Arthus reaction – Localized tissue necrosis by immune complexes – Caused by injecting an antigen into the skin • Usually from a drug Systemic Lupus Erythematosus • Chronic, multi-systemic, inflammatory disease • Involves almost any organ – Characteristically the kidneys, joints, serous membranes and skin SLE • Auto-antibodies are formed against self-antigens – Plasma proteins • Complement, clotting factors – Cell surface antigens • Lymphocytes, platelets, RBCs – Intracellular cytoplasmic components • Microfilaments and microtubules, lysosomes, ribosomes, RNA – Nuclear DNA SLE • May be a Type III Hypersensitivity disorder • Involves – Skin – Joints – Kidneys – Heart – Serous membranes • May be drug induced • Rashes: Butterfly-shaped rash over the cheeks — referred to as malar rash red rash with raised round or oval patches — known as discoid rashrash on skin exposed to the sun • Mouth sores: sores in the mouth or nose lasting from a few days to more than a month • Arthritis: tenderness and swelling lasting for a few weeks in two or more joints • Lung or heart inflammation: swelling of the tissue lining the lungs (referred to as pleurisy or pleuritis) or the heart (pericarditis), which can cause chest pain when breathing deeply • Kidney problem: blood or protein in the urine, or tests that suggest poor kidney function • Neurologic problem: seizures, strokes or psychosis (a mental health problem) • Abnormal blood tests:low blood cell counts: anemia, low white blood cells or low platelets • Positive ANA : antinuclear antibodies Discoid Rash from SLE How do the complexes cause inflammation? • Immune complexes activate complement, which: • attracts and activates neutrophils and monocytes • makes vessels leaky • Neutrophils and monocytes release bad stuff (PG, tissue-dissolving enzymes, etc.) • Immune complexes also activate clotting, causing microthrombi • Outcomes: vasculitis, glomerulonephritis, arthritis, other -itises Type III Immune Complex Allergic Disorders • Mediated by the formation of insoluble antigen– antibody complexes that activate complement – Activation of complement by the immune complex generates chemotactic and vasoactive mediators that cause tissue damage by • Alterations in blood flow • Increased vascular permeability • Destructive action of inflammatory cells Type III Immune Complex Allergic Disorders (cont.) • Immune complexes formed in the circulation produce damage when in contact with the vessel lining or when deposited in tissues – Elicit an inflammatory response by activating complement – This leads to chemotactic recruitment of neutrophils and other inflammatory cells. • Responsible for the vasculitis seen in certain autoimmune diseases like SLE Immune-complex-mediated vasculitis What complement fractions are important to know? • C3b: promotes phagocytosis of complexes (and bugs!) • C3a, C5a (anaphylatoxins): increases permeability • C5a: chemotactic for neutrophils, monocytes • C5-9: membrane damage or cytolysis Question Is the following statement true or false? • The difference between alloimmune reactions and autoimmune reactions lies in the hypersensitivity reaction. A. True B. False Answer • False: Alloimmunity refers to reaction to tissue from a donor, whereas autoimmune reactions occur against the host tissue. Hypersensitivity Reactions Outline • Introduction • Type I Hypersensitivity • Type II Hypersensitivity • Type III Hypersensitivity • Type IV Hypersensitivity TYPE IV Delayed Hypersensitivity • TYPE IV is very different from the other types of hypersensitivities 1. It is a T-lymphocyte reaction (the others are B-lymphocyte reactions) 2. It does not depend on the development of antibodies 3. The clinical appearance of the reaction is delayed a few days after antigen contact 4. The reaction is a slower process and is known as delayed hypersensitivity TYPE IV Delayed Type Hypersensitivity • Antigen are captured by macrophages for presentation to T-Lymphocytes. • T-lymphocytes react only to the antigen presented by macrophages that are sensitized to become cytotoxic T cells and memory T cells • Cytotoxic T cells attach antigen and cause either – Inflammation or – Direct cell death (cytotoxic reaction) Type IV Delayed Type Hypersensitivity • Helper T cells orchestrate the attack against • Intracellular bacterium in tuberculosis and leprosy • Persistent immune complex in contact dermatitis • Or against foreign tissue in transplantation Type IV – DTH • Type IV reactions are characterized by accumulations of macrophage around the antigen to form a nodule of lymphocytes and macrophage – The large cells surrounding a central area of tissue necrosis = Granulomas • Seen in TB Bacillus • Also seen in the Mantoux (TB) test • Cytotoxicity is the mode of type IV hypersensitivity Tcell reaction that is important in tissue transplant rejection • The most common Type IV reaction is contact dematitis Type IV – DTH • Principle mechanism of damage in: – Contact dermatitis – Tuberculosis – Transplant rejection Contact Dermatitis Delayed-Type Hypersensitivity (DTH) Perivascular cuffing by CD4+ cells Delayed-Type Hypersensitivity • Good example of DTH: positive Mantoux test • Patient previously exposed to TB • Inject (inactive) TB antigen into skin • See reddening, induration. Peaks in 1-3 days Delayed-Type Hypersensitivity • Prolonged DTH can lead to granulomatous inflammation • Perivascular CD4+ T cells replaced by macrophages • Macrophages are activated, look “epithelioid” • Macrophages sometimes fuse into “giant cells” • Granuloma = collection of epithelioid macrophages Summary Type I • Allergy • TH2 cells, IgE on mast cells, nasty mediators Type II • Antibodies • Opsonization, complement activation, or cell dysfunction Type III • Immune complexes • Lodge, cause inflammation, tissue injury Type IV • CD4+ or CD8+ T cells • DTH or T-cell-mediated cytotoxicity Granuloma DTH sounds a lot like cell-mediated immunity! • The same mechanisms underlie both. • Cell-mediated immunity is the major defense we have against intracellular bugs (like TB and fungi). • Cell-mediated immunity (good) can coexist with DTH (bad)! • Patients with AIDS: • Lack CD4+ cells • So have poor cell-mediated immune response! • Macrophages sit there unactivated; can’t kill bugs. T-Cell Mediated Cytotoxcity • CD8+ T cells recognize antigens on the surface of cells • T cells differentiate into cytotoxic T lymphocytes (CTLs) which kill antigen-bearing cells • CTLs normally kill viruses and tumor cells • In T-cell mediated cytotoxicity, CTLs kill other things: • Transplanted organ cells • Pancreatic islet cells (Type I diabetes) T-Cell-Mediated Cytotoxicity Routes of Exposure to Latex • Cutaneous • Mucous membrane – Most severe reactions result from contact with the mouth, vagina, urethra, or rectum • Inhalation • Internal tissue • Intravascular routes • Reaction types – Type I vs. type IV Delayed-Type Hypersensitivity Disorder • Cytokines are secreted causing an inflammatory response – Ie. Tuberculin skin test • Can be involved in transplant rejection and autoimmune disorders Categories of Transplanted Tissue • Allogeneic – The donor and recipient are related or unrelated but share similar HLA types. • Syngeneic – The donor and recipient are identical twins. • Autologous – The donor and recipient are the same person. Basic Patterns of Transplant Rejection • Hyperacute reaction – Occurs almost immediately after transplantation – Produced by existing recipient antibodies to graft antigens initiating a type III • Acute rejection – Occurs within first few months after transplantation with signs of organ failure; may occur months or years after immunosuppression has been terminated – T lymphocytes respond to antigens in the graft tissue. Basic Patterns of Transplant Rejection (cont.) • Chronic host-versus-graft rejection – Immunocompetent cells are transplanted into immunologically compromised recipients (TH) – Close MHC matching and selective T-cell depletion of donor are often effective in preventing this major problem Basic Requirements for Graftversus-Host Disease 1. The transplant must have a functional cellular immune component. 2. The recipient tissue must bear antigens foreign to the donor tissue. 3. The recipient immunity must be compromised to the point that it cannot destroy the transplanted cells. Question Is the following statement true or false? • Immunodeficiency disorders arise only later in life and are associated with viral infections. A. True B. False Answer • False: Many immunodeficiency disorders are congenital. Question Is the following statement true or false? • The function of MHC molecules is to mark foreign proteins, rendering them antigenic. A. True B. False Answer • False: The MHC molecules are used by the immune cells to differentiate host tissue from foreign tissue. They are found on all host tissues. Question • Which of the following hypersensitivity reactions can be treated with the administration of epinephrine? a. b. c. d. Type I Type II Type III Type IV Answer a. Type I: Type I reactions are anaphylactic; thus airway constriction is a major concern. Epinephrine stimulates airway relaxation. b. Type II c. Type III d. Type IV Hypersensitivity Disorders • Definition – Excessive or inappropriate activation of the immune system • Types – Type I, Ig-E–mediated disorders – Type II, antibody-mediated disorders – Type III, complement-mediated immune disorders – Type IV, T-cell–mediated disorders THE END Type I • Primary or initial-phase response – Vasodilation – Vascular leakage – Smooth muscle contraction • Secondary or late-phase response – More intense infiltration of tissues with eosinophils and other acute and chronic inflammatory cells – Tissue destruction in the form of epithelial cell damage Type I • Two types of cells used: – Type 2 helper T-cell – Mast cells or Basophils • Type 2 helper T-cell – CD4+ • Responds to microbes – Tβ2 • Respnds to allergens or helminths (intestinal parasites) Type I • Mast Cell – Allergen-specific IgE-antibodies attach to receptors on the surface of mast cells and basophils – The sensitizing allergen binds to the cell-associated IgE • Triggers a series of events that ultimately lead to degranulation and the Primary Early Response – The Secondary or late Response occurs 2 to 8 hours • Lasts for several days Types of IgE-Mediated Allergic Reactions • Atopic disorders – Hereditary predisposition and production of a local reaction to IgE antibodies produced in response to common environmental agents • Urticaria (hives), allergic rhinitis (hay fever), atopic dermatitis, food allergies, some forms of asthma • Non-atopic disorders – Lack the genetic component and organ specificity of the atopic disorders Type II (Antibody Mediated) Hypersensitivity Reactions • Examples – Mismatched blood transfusion reactions – Hemolytic disease of the newborn – Certain drug reactions Type IV (Cell Mediated) Delayed Type Hypersensitivity • Cell-mediated immune response • Mediated by sensitized T lymphocytes – The principal mechanism of response to a variety of microorganisms including intracellular pathogens and extracellular agents – Can lead to cell death and tissue injury in response to chemical antigens or self-antigens • Basic types – Direct cell-mediated cytoxicity • Hepatitis – Delayed-type hypersensitivity • Allergic contact dermatitis • Hypersensitivity pneumonitis Type III – Immune Complex Hypersensitivity • Abnormal Response – Too much antigen (dust in the lungs) – Too many antibodies (autoimmune disease) • Small Antigen-antibody complexes are formed in the circulation and deposited mainly in the tissues –microthrombi • These complexes induce a localized inflammatory response by activating the complement system