Effect of pH upon skin permeation of ionizable and non
advertisement

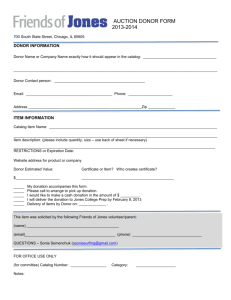
Effect of pH upon skin permeation of ionizable and non-ionizable drugs for topical delivery Siriwan Chootanasoontorn1,2,*, Jiraphong Suksiriworapong2,3, Doungdaw Chantasart2,3,# 1 Master of Science in Pharmacy Programme in Pharmaceutics (International Programme), 2 Department of Pharmacy, Faculty of Pharmacy, Mahidol University, Bangkok, Thailand 3 Center of Excellent in Innovative Drug Delivery and Nanomedicine, Faculty of Pharmacy, Mahidol University, Bangkok, Thailand *e-mail: kae_jung2@hotmail.com, #doungdaw.cha@mahidol.ac.th Abstract Topical drug delivery is a common approach for local therapy of skin disease to reduce systemic side effects. Drug permeation across stratum corneum, the main skin barrier is required for the topical skin treatment. It is affected by several factors such as the physicochemical properties of drugs and vehicles of the drug administration. The objective of this study was to determine the effect of pH upon skin permeation of ionizable and non-ionizable drugs for topical delivery. Naproxen sodium (NX), betaxolol hydrochloride (BX), and corticosterone (CS) were selected as model drugs for acidic ionizable, basic ionizable, and non-ionizable drugs, respectively. The permeability experiments were carried out in side-by-side diffusion cells with human epidermal membrane (HEM) in vitro. The permeability coefficients of the model drugs across HEM were evaluated under two pH donor solutions (pH 5.8 and 7.4) while the receiver solution was maintained at pH 7.4. The apparent permeability coefficients of NX across HEM increased as the pH of the donor decreased while their BX incremented with the pH of donor solution. Unlike to NX and BX, no significant change of apparent permeability coefficients of CS was observed when the pH of the donor solution altered. The results suggested that the pH of the donor solution is a major factor influencing HEM permeation of ionizable drugs due to the high fraction of non-ionized species of drugs. Keywords: ionizable drug, non-ionizable drug, skin permeation, pH, topical drug delivery Introduction Topical drug delivery is a common noninvasive approach for local therapy of skin disease to reduce systemic side effects. It also provided several advantages such as controlling the constant amount of drug delivery during a long period of time, increasing the patient’s compliance and reducing the dose of drug administration (1). Stratum corneum (SC) is an outer part of epidermis and consisted of highly lipid lamella structure. There are three essential pathways for drug permeation across the SC: intercellular lipid domain; transcellular route; and the appendages (1, 2). The physicochemical properties of drugs and vehicles could affect the drug permeation process. A number of active pharmaceutical agents can be used topically to treat skin diseases. For example; non-steroidal anti-inflammatory drugs (NSAIDs) (e.g., naproxen, diclofenac) are used to inhibit inflammation of local and deep tissues (muscle, fascia, joint, synovial fluid) (3, 4). Topical -blockers (e.g., betaxolol, propranolol) are used to treat infantile hemangiomas, the common benign tumors in infancy (5). Topical steroids (e.g., corticosterone, triamcinolone) are used for anti-inflammation in cutaneous disease (6). The aforementioned NSAIDs and -blockers are acidic and basic ionizable drugs whereas steroids are non-ionizable drugs. Due to the lipophilic nature of SC barrier, an ionization fraction of 1 ionizable drugs, a function of pKa and the pH of dosage form could significantly affect the drug permeation across the SC barrier. This study aimed to investigate the pH effect upon skin permeation of ionizable and nonionizable drugs for topical delivery. Naproxen sodium (NX), betaxolol hydrochloride (BX) and corticosterone (CS) were selected as model drugs for acidic ionizable, basic ionizable and nonionizable drugs, respectively. The physicochemical properties of the investigated drugs are shown in Table 1. Table 1 The physicochemical properties of naproxen sodium (NX), betaxolol hydrochloride (BX) and corticosterone (CS) Molecular weight (g/mol) pKa log KO/W Acidic ionizable drug: NX 252.2a 3.2a 4.15b Basic ionizable drug: BX 307.4c 9.4c 3.50c Neutral non-ionizable drug: CS 346.5d - 1.94d Type of drug Structure a Value from the literature (7) Value from the literature (8) c Value from the literature (9) d Value from the literature (10) b Methodology Materials Naproxen sodium (Zhejiang Tianxin Pharmaceutical Co., Ltd., Tiantai, China) was donated from Siam Pharmaceutical Co., Ltd (Bangkok, Thailand). Betaxolol hydrochloride was purchased from Sigma-Aldrich (Missouri, USA). Betaxolol hydrochloride ophthalmic solution 0.5% was purchased from Falcon Pharmaceuticals, Ltd. (Fort Worth, USA). Corticosterone and sodium azide (NaN3) were purchased from Fluka (Steinheim, Switzerland). Sodium dihydrogen orthophosphate and disodium hydrogen orthophosphate were purchased from Ajax Finechem (New South Wales, Australia). Sodium chloride (NaCl) was purchased from Carlo Erba reagent (Milan, Italy). High performance liquid chromatography (HPLC) grade methanol and acetonitrile were purchased from Honeywell Burdick & Jackson (Ulsan, Korea). Glacial acetic acid and sodium hydroxide were purchased from RCI Labscan Co., Ltd. (Bangkok, Thailand). Isotonic phosphate buffered saline (PBS) pH 5.8 (comprising 0.01 M phosphate buffer and 0.145 M NaCl) and pH 7.4 (comprising 0.01 M phosphate buffer and 0.142 NaCl) were prepared and 2 preserved by 0.02% NaN3 (13). A pH meter (Inlab®, Mettler-Toledo International Inc, Ohio, USA) was used for measuring pH values of buffer and drug solution. Deionized water was used entirely throughout this work. Preparation of HEM Abdominal human skin from plastic surgical operations of female aged between 30 and 60 years was supplied by the Department of Surgery, Yanhee General Hospital, Thailand. The skin sample was obtained within a few hours after operation. HEM, consisting of the SC and viable epidermis, was separated from the dermis by immersing the skin samples the fatty tissuefree fatty tissue in PBS pH 7.4 at 60C for 90 s (11). After heat treatment, HEM sheet was separated from the dermis by roll-peeling using plastic forceps and immersed in freshly PBS pH 7.4. The HEM was then patted dry with tissue paper, wrapped in an aluminum foil sheet, and kept in a -20°C freezer for later use. The experimental protocol was approved by the Committee on Human Right Related to Human Experimentation, Mahidol University, Bangkok, Thailand. HEM Permeability Experiments The frozen HEM samples were cut into the required size ( 2 cm × 2 cm), defrosted at room temperature and hydrated in PBS pH 7.4 overnight. The hydrated HEM was placed between the two diffusion half-cells with a cellulose membrane (Spectra/Por® MWCO 12,00014,000, Spectrum Laboratories, Inc., Rancho Dominguez, California, USA) as a support membrane between the viable epidermis side and receiver chamber side. The cellulose membrane was immersed in PBS pH 7.4 overnight before using. Two milliliters of PBS pH 7.4 was pipetted into both chamber and equilibrated in a circulating water bath at 37±1ºC for ~ 12 h before the permeability experiments (12). Skin permeability experiments were conducted in the two-chamber side-by side diffusion cells with the HEM for the three model drugs (namely, NX, BX, and CS). Each chamber of the diffusion cell had a 2-mL volume and an effective diffusion area of ~1.10 cm2. The experiments were conducted under 2 different conditions of donor solution pH 5.8 and 7.4 while receiver solution was kept at pH 7.4. Each drug solution in PBS pH 5.8 and 7.4 were prepared. Approximately 100 -1000 µg/mL of NX, BX and CS were added in each PBS. The pH of each solution was adjusted with 1 N NaOH solution to obtain the required pH. Two milliliters of each drug solution (pH 5.8 and 7.4) were added in the donor chamber and 2 mL PBS pH 7.4 was added in the receiver chamber. Since the apparent pH of the SC is 4.0-6.0 (13, 14) and the physiological pH is 7.4, the drug solutions at pH 5.8 and 7.4 were used to study the drug permeability under the pH range mimicking the SC and the physiological conditions, respectively. The diffusion cells were placed in a circulating water bath at 37±1ºC with continuously stirring. At predetermined time intervals, 10 µL and 500 µL samples were taken from the donor and receiver chambers, respectively. The same volume of fresh PBS pH 7.4 was replaced in the receiver chamber after each sampling. The total duration of each permeability experiment was around 18 h. Because of the laboriousness of HEM preparation, the electrical resistance of HEM was used to check the integrity of the skin membrane at the beginning and the end of each permeability experiment. The HEM with electrical resistance ≥ 15-20 kΩ cm2 can be indicative of good intact HEM barrier (15). Analytical method The quantification of model drugs was determined by HPLC method. The HPLC system composed of a LC-20AD pump, DGU-20A5 degasser, SIL-10AF autosampler, SPD-20A UV/VIS detector (Shimadzu Corporation, Kyoto, Japan) and Zorbax® SB-C18 column with a guard column (5 µm particle size, 150 × 4.6 mm, Agilent Technologies Inc., California, USA). 3 The mobile phases, flow rates, detector wavelengths, and retention times for NX, BX, and CS were: acetonitrile/water/glacial acetic acid (45:55:2.5 V/V), 1 mL/min, 280 nm, 7 min; methanol/water/glacial acetic acid/triethylamine (500:500:3.5:1 V/V), 1 mL/min, 273 nm, 7.4 min and methanol/water (65:35 V/V), 0.8 mL/min, 248 nm, 7.4 min, respectively. The injection volume was 50 µL for all systems. The standard solution of each drug was prepared in a mobile phase and used to construct a calibration curve based on the peak area measurement. The samples were appropriately diluted in a mobile phase for subsequent analysis. Data Analysis The apparent permeability coefficient (Papp) was calculated by 1 dQ (1) Papp ( ).( ) AC D dt where (dQ/dt) denotes the slope of the steady-state region of cumulative amount of drug permeated across the skin into the receiver chamber, A is an effective area of diffusion cell and CD is a concentration of drug in the donor chamber. For data analysis, the student’s t-test was employed to determine the statistical differences in the experiment using SPSS. Significantly differences are considered at p< 0.05. The means standard deviations (SD) of the data are presented. Results Figure 1 presents the apparent permeability coefficients of NX, BX and CS across the HEM under different pHs of the donor solution (pH 5.8 and 7.4) while the receiver solution was maintained at pH 7.4. When the pH of the donor solution increased from 5.8 to 7.4, the apparent permeability coefficients of NX decreased, whereas those of BX increased. Unlike to BX and NX, no significant change of apparent permeability coefficients of CS in donor solution pH 5.8 and 7.4 was observed. 7 P (cm/s) x10-7 6 5 4 pH 5.8 3 pH 7.4 2 1 0 NX BX CS Model drug Figure 1 Permeability coefficients of three model drugs (i.e., NX, BX and CS) across the HEM under different pHs of the donor solution (pH 5.8 and 7.4) when the receiver solution was maintained at pH 7.4. Mean ±SD (n ≥ 4). 4 For acidic and basic ionizable drugs, the fraction of non-ionized species (fnon-ion) was calculated using Eq. 2 and 3, respectively 1 f non-ion (acidic drug) (2) 1 10 pH pKa 1 (3) f non-ion (basic drug) 1 10 pKa pH Table 2 The fraction of non-ionized species (fnon-ion) and the apparent permeability coefficients (P app) of naproxen sodium (NX) and betaxolol hydrochloride (BX) across the HEM under the donor solution pH 5.8 and 7.4 a pH of donor solution NX BX fnon-ion Pappa (cm/s) ×10-7 fnon-ion Pappa (cm/s) × 10-7 5.8 2.19 3.83±1.50 0.03 0.95 ± 0.43 7.4 0.06 0.53±0.084 1.14 5.10 ± 1.25 Mean SD, n≥ 4 The apparent permeability coefficients of NX and BX across the HEM under the donor solutions pH 5.8 and 7.4, along with the calculated non-ionized fraction, are summarized in Table 2. The permeability coefficient of NX increased 7-fold when the non-ionized fraction increased from 0.06 (at pH 7.4) to 2.19 (at pH 5.8). For BX, the permeability coefficient increased 5-fold when the non-ionized fraction increased from 0.03 (at pH 5.8) to 1.14 (at pH 7.4). Discussion and Conclusion In a previous HEM study , it was indicated that CS, a non-ionizable steroidal drug, is a good model drug which permeates across the SC via the lipoidal pathway. Taken together with the results in Figure 1 and Table 2, it can be summarized as follows. First, no significant change of apparent permeability coefficients of CS was observed when the pH of the donor solution increased or decreased because there is no change of the non-ionized species of CS. Second, the apparent permeability coefficients of NX and BX decreased significantly because of the decreasing non-ionized species of the drugs which was affected by the change of pH of donor solution. Following the Fick’s first law of drug permeation across the skin (2): dQ DC 0 K (4) dt h where D is the diffusion coefficient or diffusivity of drug molecules, C0 is the drug concentration in the donor chamber under sink condition, K is the partition coefficient of the drug between skin and donor solution, and h is the thickness of the SC. From the equation, dQ/dt is directly proportion to D, C0 and K. When the fraction of non-ionized moieties of ionizable acidic or basic drugs is increased by increasing or decreasing pH of vehicle, respectively, the partition coefficient increase. It can be pointed out that the pH change of donor 5 solution affects the increasing non-ionized species and the apparent permeability coefficients of ionizable drugs. Third, the drug permeation across the SC, the main skin barrier, would be dominated by the non-ionized species of drugs. Finally, it can be concluded that the pH of the donor solution is a major factor influencing HEM permeation for topical ionizable drugs due to the high fraction of non-ionized species of drugs. References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. Morrow DIJ, McCarron PA, Woolfson AD, Donnelly RF. Innovative strategies for enhancing topical and transdermal Drug Delivery. The Open Drug Delivery Journal. 2007;1:36-59. Williams AC. Transdermal and topical drug delivery. London: Pharmaceutical Press 2003. Van den Ouwelan dF, Enhroon P, Tan Y, Gribnau F. Transcutaneous absorption of naproxen gel. Eur J Clin Pharmacol. 1986;36:209-11. Singh P, Roberts MS. Skin Permeability and Local Tissue Concentrations of Nonsteroidal Anti-Inflammatory Drugs after Topical Application. J Pharmacol Exp Ther. 1993;268(1):255-162. Khunger N, Pahwa M. Dramatic response to topical lotion of a large hemifacial infantile haemangioma associated with PHACE syndrome. Br J Dermatol. 2011;164:886-8 Mark E, Johnson M, Blankschteinl D, Robert Langer R. Permeation of Steroids through Human Skin. Journal Pharmaceutical Scienece. 1995;84(9):1144-6. Mofatt AC. Clarke Analysis of drugs and Poison 3rd ed. London: The Pharmaceutical Press; 1980. p. 1319. Mart´ınez-Pla JJ, Mart´ın-Biosca Y, Sagrado S, nas RMV-C, andez MJM-H. Evaluation of the pH effect of formulations on the skin permeability of drugs by biopartitioning micellar chromatography. J Chromatogr. 2004;1047:255-62. Scidi S, Yamini Y, Rczazadch M. Electrically enhanced microextraction for highly selective transport of three β-blocker. J Pharm Biomed Anal. 2011;56:859-66. Chantasart D, Sa-Nguandeekul P, Prakongpan S, Li SK, Higuchi WI. Comparison of the effects of chemical permeation enhancers on the lipoidal pathways of human epidermal membrane and hairless mouse skin and the mechanism of enhancer action. J Pharm Sci. 2007;96(9):2310-26. Kligman AM, Christophers E. Preparation of isolated sheets of human stratum corneum. Arch Dermatol. 1963;88:702-5. Peck KD, Ghanem AH, Higuchi WI, Srinivasan V. Improved stability of the human epidermal membrane during successive permeability experiments. Int J Pharm. 1993;98:141-7. Ohman H, Vahlquist A. In vivo studies concerning a pH gradient in human stratum corneum and upper epidermis. Acta Derm Venereol. 1994;74(5):375-9. Fluhr JW, Elias PM. Stratum corneum pH: formation and function of the ‘Acid Mantle’. Exog Dermatol. 2002;1:163-75. Kasting GB, Bowman LA. DC electrical properties of frozen excised human skin. Pharm Res. 1990;7:134-43. Acknowledgements The authors thank Yanhee General Hospital for kindly supplying the human skin samples. 6