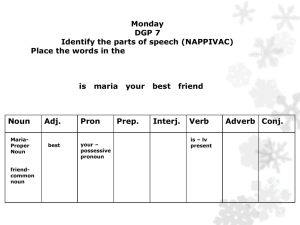
EMCaseLearnerGuideVaginitisCervicitisPID
advertisement

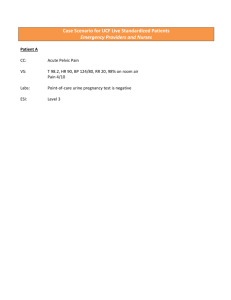
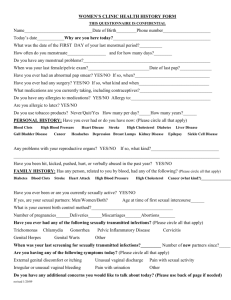
CASE: VAGINITIS, CERVICITIS, PID Maria is a 35yo Latino female walking into the ED alone. She presents to triage complaining of vaginal discharge for 1 week and lower abdominal pain for past 2 days. It is a weekend evening, and you are at a moderate-sized ED facility where there is GYN on-call consultation, limited after-hours radiology, and 24-hour onsite laboratory services. ABCs are intact. Maria reports heavy yellow “fishy smelling” vaginal discharge for the past week with worsening lower abdominal pain for 2 days. She denies any bleeding or lightheadedness. She’s felt feverish, a little nauseous and overall “crummy”. Her LMP was 3 weeks ago and was normal. She is sexually active, and when asked if she could be pregnant, she says “No.” Maria screens negative for violence or trauma, but reports military sexual trauma (MST) when she was active duty. VS: T 99, HR 101, BP 124/72, RR 16, 96% on room air Pain: 6/10, generalized lower abdomen, constant ache with intermittent shooting pains, non-radiating Maria was brought back alone to a private treatment room and gets changed into a gown. On your initial nurse assessment, you note a middle-aged woman, sitting on the exam table in mild-to-moderate discomfort. On your questioning you find she is G1P0 (miscarriage 7yrs ago). She’s sexually active and doesn’t use any method of contraception. She denies any recent exposure to STI, but says she had trichomonas in her teens. She denies dysuria, hematuria or increased urinary frequency. Maria used an other-the-counter treatment for yeast 5 days ago because she thought that’s what the discharge was from, but it didn't help. She also took a few doses of acetaminophen and ibuprofen for the pain with little relief. Medication reconciliation confirms she is on fluoxetine; she is allergic to sulfa. Maria appreciated being given choices is it relates the pelvic exam and her history of MST. She prefers a female provider, and one is available. She also finds it helpful to sit more upright to be able to see the provider during the exam and prefers being talked through the steps of the exam. VS reassessment reveals T 99.1, HR 108, BP 135/82, RR 16 Pain 9/10 The provider walks into the treatment room and finds a woman sitting, hunched over, holding her abdomen and tearful. VS are T 99.1, HR 108, BP 135/82, RR 16; Pain 9/10 1 Appropriate questions to ask for vaginal discharge and abdominal/pelvic pain history: 1. LMP? Was it normal? Are periods regular? 2. Quantity & characteristics of discharge – amount, odor, consistency, color, itching? 3. Use of douching, sex toys, creams/lotions/sprays/lubricants, foreign bodies (pessary, female condom, contraceptive ring, tampon)? 4. Are you sexually active? With men, women or both? When were you last sexually active? Number of sexual partners? 5. Method of contraception? Consistent use? Consistent barrier method use? 6. History of sexually transmitted infections? 7. Recent GYN procedures? 8. N/V? Urinary symptoms? 9. Vaginal, rectal or urinary tract bleeding? 10. Last bowel movement? 11. Last meal? 12. Allergies? 13. Medications? (specifically OTC medications or self-remedies) The nurse provides Maria with 4mg morphine IV push and 1L NS IVF per provider orders. While the provider is assessing Maria, the nurse is gathering supplies for the pelvic exam (detailed above). Maria tells the provider she’s been having large amounts of yellow frothy “fishy” smelling vaginal discharge. She denies douching, but admits to using sex toys with lubrication; no other topicals apart from the recent antifungal cream. She is sexually active with 1 female partner only for the past 10 years. No known exposure to STIs, but confirms the remote history of trichomonas. Past medical history is significant for PTSD, MST. She has no surgical history, nor recent GYN procedures. She’s allergic to sulfa. She takes only fluoxetine. She last ate 10 hours ago. She is a smoker, but denies alcohol or drug use. The nurse relays negative pregnancy test results. The female nurse serves as the chaperone, supplies are ready, exam steps have been described and Maria has given verbal consent for pelvic exam. Her privacy has been attended to. Maria sits as upright as possible during the pelvic exam and is talked through each step of the exam, per her stated preference. Physical exam GEN: mild distress, A&O HEENT: normal PULM: CTAB CV: mild tachycardia, regular rhythm ABD: soft, non-distended, left lower abdominal tenderness with voluntary guarding, no rebound, no CVAT PELVIC: External inspection: normal external genitalia, no lesions, no signs of trauma Speculum: moderate yellow watery discharge at introitus and pooled in vaginal vault, no discharge from closed cervical os Bimanual: moderate-severe CMT, normal uterus, left adnexal tenderness with questionable fullness SKIN: normal NEURO: non-focal, GCS-15 2 Maria is ready to be transported to radiology. The initial morphine improved her pain a bit, but after the pelvic exam, she is still in moderate pain. VS reassessment reveals HR 92, BP 122/72 Pain 5/10 The nurse provides Maria with an additional 4mg morphine IV push as ordered before she goes to radiology. Labs show: WBC 15,000 Hgb 14.1 Hct 42.2 Platelets 350,000 INR 1 Na 136 Cl 97 HCO3 24 K 3.8 BUN/Cr 10/0.5 Glucose 97 LFTs normal Clean catch UA: 15-20 squamous epithelial cells, 6-10 WBCs, negative LE/nitrites, RBCs, and bacteria Wet mount: pH 5.5, WBCs 20/hpf, >20% clue cells, no trichomonads, no hyphae/budding yeast GC/Ch probe: pending The radiologist calls with the TVUS results: ill-defined heterogenous, complex left adnexal mass associated with fluid-filled tubular structure and peri-tubular stranding consistent with inflammation; small amount of free fluid is seen in the cul-de-sac. Maria has received a total of 8mg morphine IV and 1L NS has infused. VS reassessment reveals T 100.9, HR 101, BP 130/82, RR 16 Pain 2/10 Maria continues to report feeling better. Blood cultures were drawn prior to antibiotic initiation of cefoxitin, doxycycline (IV because of desire to keep NPO), metronidazole. VS reassessment reveals T 99.2, HR 90, BP 128/72, RR 16 Pain 2/10 GYN consult – agree with IV antibiotic choice, keep NPO in the event of surgical indication (i.e. TOA rupture or failure to improve), GYN will be in to evaluate and repeat pelvic exam. Plan for admission. Private, female inpatient accommodations are made for Maria and bed availability is confirmed. 3 Maria defervesced the next day and remained afebrile for 48 hours. She was converted to oral doxycycline and oral metronidazole to complete a 14-day course of both and discharged to home. She was followed-up as an outpatient with GYN where a repeat TVUS showed complete resolution in her TOA. KEY LEARNING POINTS – VAGINITIS, CERVICITIS, PID All female patients with abdominal pain, pelvic pain and/or vaginal complaints who are <52 years of age should have pregnancy assessed at triage Life and fertility threatening conditions must be recognized All female patients with abdominal pain, pelvic pain or vaginal discharge require pelvic exam with adequate pelvic exam set-up prior to specialty consultation When performing a pelvic exam, adhering to patient dignity, privacy and appropriate female chaperone requirements are crucial Emergency providers should be able to differentiate upper from lower genital tract infections based on the presence of pelvic organ tenderness Females in same-sex relationships can be at risk for polymicrobial infection of PID and develop TOA Indications for emergent TVUS when PID is suspected include: hospitalization requiring inpatient treatment, clinical suspicion of pelvic abscess/TOA, and identification of pelvic mass on exam or inability to adequately assess the adnexa Emergency providers should be familiar with appropriate CDC-recommended antibiotic regimens for TOA and start IV antibiotics in the ED Frequent communication between nurses and providers, noting changes in assessment and plan of care, is crucial The plan of care should be effectively communicated to patients throughout the encounter 4