Program - Boston Scientific")
How to Setup a Successful Left
Atrial Appendage Closure (LAAC)
Program
INTRODUCING
WATCHMAN
SH-303719-AB June 2015
Program Agenda
A) Institution Evaluation
B) Key Players in LAAC Team
C) Hospital Support
D) Patient Flow
E) Patient Selection
F) Identify and Educate the Internal and External Referral Pathways
G) Market Yourself as a Center of Excellence
Backup Tools & Materials
SH-303719-AB June 2015
A) Institution Evaluation
SH-303719-AB June 2015
A) Institution Evaluation
Academic
or
Private
Understanding Site
-
-
-
-
-
Academic or Private: how to will a
LAA program successfully work
(similar goals vs. competing
goals)
Clinical or Commercial: starting
from the ground floor vs. making
changes to the existing clinical
structure
EP, IC or Both: What specialty is
leading the therapy will be key to
understanding program
administration
Structural Heart Program: Will
have a program to learn from
(positive & negatives)
Existing AFIB / complex EP
program: Understanding of
current AFIB patients and their
flow
SH-303719-AB June 2015
Afib or
Complex EP
Program
Structural
Heart
Program
Your
Site
LAA Clinical
or
Commercial
EP, IC or
Both
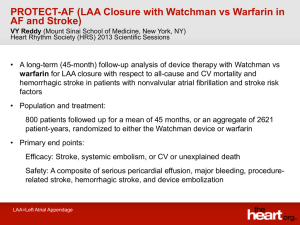
A) Institution Evaluation
Institutional Qualifications:
• Minimum requirements (i.e. transseptal experience, TEE, surgical back-up)
• Access to AF patients/referral network (ability to maintain case volume)
• EP/IC collaboration (Heart Team): clinical experience demonstrates more
successful adoption in accounts
Clinical/Implanter Qualifications:
• Physician skills/experience - transseptal experience, AF ablations, structural
heart procedures
• Transseptal experience - 25 punctures in career, 10 within last 12 months
(ASD/PFO not applicable)
• TEE echocardiography experience / skills
• Commitment to complete the required WATCHMAN training program
Business Qualifications:
• Ability to commit to initial order – No consignment or rep trunk stock
• Boston Scientific partnership / collaboration
SH-303719-AB June 2015
B) Key Players in LAAC Program
SH-303719-AB June 2015
B) LAAC Team
Hospital Admin
Operators
(EP/IC/Echo)
(Marketing, Coding,
Finance, data support)
Referral
Community
LAA
Coordinator
Left Atrial
Appendage
Team
Surgery
Imaging
Anesthesiologist
Dedicated Lab
Staff
Success Factors in Building a LAAC Team
-
Collaboration & coordination is key
Coordinator who understands therapy, program and patient flow
Block WATCHMAN Days (anesthesia set time, imaging set time & consistent lab staff)
Hospital and administration support
Education of referral community to understand procedure as well as ensure appropriate patients
Identification of a viable referral base who believes in LAA closure therapy
SH-303719-AB June 2015
B) LAA Program Key Players
-
-
-
-
Operator:
- Based on operator (EP / IC / Both) will change techniques through out case
LAA Coordinator:
- Identify the LAAC Coordinator / Champion that understands the clinical pathway, process
and the procedure
Imaging:
- Small group of physicians that are trained on views. Consistent measuring pre, during and
post. Understand needs for trans septal puncture, standardized protocols, sonographer
competency with check off to ensure imaging quality
Anesthesia:
- Ability to understand LAA vs TAVR, block time with anesthesia will ensure on time cases
LAAC Lab Staff:
- Educated staff on patient needs, procedure and flow will help with outcomes
Surgery:
- Establish relationship and understanding of possible back up needs and alt therapies
Referrals Community:
- Educated and bought in community that will identify optimal patients for left atrial
appendage procedure
Hospital Admin:
- Ensure buy in at all administrative levels of the procedure value for patients and hospital /
Marketing / PR
SH-303719-AB June 2015
B) Program Structure Options
Operators: IC and EP with the support of Echo
Coordinator: Supports operators in all program structures
Structural Heart
• Complement to
existing structural
heart program
• LAAC can
complement
current structural
program including
TAVR, Mitral,
ASD/PFO
SH-303719-AB June 2015
Complex EP /
Arrhythmia
• Complement to
existing complex
left sided EP
procedures
• LAA can
complement
current complex
EP program
including
extractions, afib
and VT ablations
Afib Center
LAA Program
• Complement or
new to afib center
which manages
afib patients and
offers all medical
and device option
to patients
• LAAC can be
another offering to
your afib patients
that suffer from a
variety of oral
anticoagulation
side effects
• Offer a full suite of
LAA closure
options which
include surgical
and noninvasive
• LAAC can be
another offering to
current surgery
options offered to
patients
C) Hospital Support
SH-303719-AB June 2015
C) Hospital Support
Additional Key Players in Hospital Administration
• Administration:
CEO, Directors, Department Chair
• Economics:
Finance-Billing/Coding Team
• Lab Leaders:
CV Service Line Directors
• Material Mgt:
Purchasing, Inventory, etc
• Marketing Team:
Strategic Planning and Marketing
SH-303719-AB June 2015
C) Hospital Support
1st Step to Building Successful LAAC Program
• Gain hospital support on all levels
• Establish and educate on clinical need for program
• Discuss patient benefit
– Improve patient outcomes compared to oral anticoagulation
– Reduce oral anticoagulation burden on your patients’ QOL
• Discuss Hospital and Program Advantage
– Marketing differentiator
– Physician retention and recruitment
– Comprehensive AF/Stroke treatment program
• Hospital Opportunity
– Incremental patient growth
SH-303719-AB June 2015
C) Hospital Support
“Reimbursement” = Coding + Coverage + Payment Rates
Upon FDA approval, we will have Coding and Payment Rates established.
Will apply for Coverage when eligible… immediately after approval.
Key Points
• Coverage gaps are routine for new novel technologies (e.g., SAPIEN,
MitraClip)
•
•
•
BSC is proactively working with CMS and FDA with the goal of facilitating
Medicare coverage as soon as possible after FDA approval
If coverage is not in place upon FDA approval, it will be necessary for
clinicians/hospitals to seek coverage on a case-by-case basis by appealing
denials if they occur
IN-PATIENT ONLY procedure and anticipate patient population to be primarily
Medicare. Not subject to the two midnight rule.
SH-303719-AB June 2015
Hospital Reimbursement: Will I get paid?
SH-303719-AB June 2015
Implanting Physician Reimbursement: Will I get
paid?
SH-303719-AB June 2015
C) Hospital Support
Tools Available
Download Central (click above)
• WATCHMAN Comprehensive Reimbursement (coding, coverage, and payment) Guide
• WATCHMAN Prior Authorization template
• WATCHMAN Appeals template
• WATCHMAN Economic Value Presentation (via Economic Navigator web tool)
• Physician Category III Code Guide
• Documentation & MS-DRG Guide
• Hospital Appropriateness of Charging Guide
• WATCHMAN Value Toolkit
Health economic and reimbursement information provided by Boston Scientific Corporation is gathered from third-party sources and is subject to
change without notice as a result of complex and frequently changing laws, regulations, rules and policies. This information is presented for illustrative
purposes only and does not constitute reimbursement or legal advice. Boston Scientific encourages providers to submit accurate and appropriate
claims for services. It is always the provider’s responsibility to determine medical necessity, the proper site for delivery of any services and to submit
appropriate codes, charges and modifiers for services that are rendered. Boston Scientific recommends that you consult with your payers,
reimbursement specialists and/or legal counsel regarding coding, coverage and reimbursement matters. Boston Scientific does not promote the use of
its products outside their FDA-approved labeling.
Payer policies will vary and should be verified prior to treatment for limitations on diagnosis, coding or site of service requirements. The coding options
listed within this guide are commonly used codes and are not intended to be an all-inclusive list. Providers are responsible for making appropriate
decisions related to coding and reimbursement submissions. We recommend consulting your relevant manuals for appropriate coding options.
Payer policies will vary and should be verified prior to treatment for limitations on diagnosis, coding or site of service requirements. The coding options
listed within this guide are commonly used codes and are not intended to be an all-inclusive list. We recommend consulting your relevant manuals for
appropriate coding options.
SH-303719-AB June 2015
C) Hospital Support
Other Efforts to be Coordinated (if applicable):
• Quality Team
– Ensure understanding of WATCHMAN product and support from quality
team
• Value Analysis Team Meeting
– Secure date and meeting time for WATCHMAN product
• LAAC Credentials
– Define credentials are in place at time of launch
• Reimbursement & Economics
– Support of WATCHMAN procedure reimbursement process (resources
available)
• Data Support
– Ability to support tracking and collecting data for study, registry and
additional procedures performed on LAAC patients
SH-303719-AB June 2015
D) Patient Flow through LAAC
Procedure
SH-303719-AB June 2015
D) Patient Flow through LAAC Procedure
Education
•
•
•
•
Educate patients and families about disease and treatment options
Educate on the LAAC procedure
Explanation of risks and benefits of procedure
Explanation of the process from screening >> procedure >> follow up
• Secure insurance pre-authorization for procedure
• Ensure patient is appropriate candidate for LAAC procedure (indication)/supporting documentation
• Review previous TEE (if available) or schedule new TEE to ensure patient in a good candidate (size,
Screening
thrombus, etc.)
• Schedule pre-procedure diagnostic studies, labs, echo, etc.
• Schedule procedure date for lab time, implanter, anesthesia, TEE physician, patient, company
representative (LAAC team)
Scheduling • Schedule post-procedure follow-up office visit, labs and TEE @ time of discharge (if registry req)
• Ensure patient has followed pre procedure instructions
• Ensure all key players in the LAAC team are present for procedure
• Post procedure ensure that patient and family understand post procedure instructions (medication,
Procedure
follow up TEE date, etc.)
SH-303719-AB June 2015
D) Patient Flow through LAAC Procedure
Patient Education
1)
2)
3)
4)
5)
Disease State
Disease Treatment (drug vs. device)
Procedure
Risks & Benefits
Procedure Process
Tools Available
Download Central (click above)
Patient Material
Patient Brochure
Patient video / animation
Device example
Additional Materials
WATCHMAN Patient Website click
Post Implant FAQ
Pre and Post Procedure samples
Website(s)
StopAfib.org click
SH-303719-AB June 2015
D) Patient Flow through LAAC Procedure
Patient Screening
1)
2)
3)
Ensure patient is appropriate candidate for LAAC procedure
Secure insurance pre-authorization for procedure
Review previous TEE (if available) OR schedule new TEE (Views, size, thrombus)
Screening Tools Available
-
Download Central (click above)
Indication Material
Echo protocols (view, size, thrombus)
Patient Identification Tools
Left Atrial Appendage Closure Evaluation
Tools to Save, Print & PDF
- EMR queries / workflow
- Patient database / worksheet
- LAAC Patient Sources (Coumadin clinics, GI clinic, ER)
Update List of LAA Patients
Demographics:
Name:
DOB:
Phone:
SS/Chart #:
Address:
Afib History
No
Ablation:
CAD:
Afib:
Type
Modera te/Severe
Rheuma tic Mi tra l
Stenos i s
Mecha ni ca l hea rt va l ve
Previ ous Mi tra l Va l ve
Surgi ca l Repa i r
No AFIB
Pervious CABG
No
No
Cardioversion:
TEE:
No
Date of TEE:
CT:
Date of CT:
Previous Echo:
Date of Echo:
No
Referring 1:
Referring 2:
Create PDF File
Where Patient Heard About Procedure:
Chf:
Htn:
Physical History (CHADS Vasc / HASBLED)
No
Htn:
No
Bleed:
No
No
No
No
Age:
Diabetes:
0
No
No
No
No
Stroke/TIA:
Vascular dz:
Sex/Gender:
No
No
No
No
No
Male
CHADS2 Score:
CHADS2 annual risk:
CHADS2 VASC2 Score:
CHADS2 VASC2 annual risk:
Labile INR:
Drugs:
0
1.9%
0
0.0%
Renal:
Liver:
Stroke/Tia:
Alcohol:
Email Report
0
0
0
0
No
0
No
0
No
0
No
0
Hasbled score: 0
Annual Bleed risk: 1.1%
Current Meds
1
2
3
4
5
Screening appointment:
Coordinator meeting:
Referring Physician Follow-up:
SH-303719-AB June 2015
6
7
Comments:
8
9
Misc Notes:
10
Warafin Eligible:
NOT LEFT ATRIAL APPENDAGE CANIDATE
Action & Next Steps
Insurance:
Pre-auth:
Surgical date:
No
Clear Form
C) Patient Flow through LAAC Procedure
Pre-procedural Instructions (found in DFU)
A baseline TEE should be performed to verify that a patient’s anatomy is appropriate for a WATCHMAN®
Device to be implanted.
1. Assess the following through multiple imaging planes (0°, 45°, 90° and 135° sweep):
- LAA size/shape, number of lobes in LAA, and location of lobes relative to the ostium.
- Confirm the absence of thrombus (use Color Doppler and echo contrast as necessary).
2. Record LAA ostium and LAA length measurements (0°, 45°, 90° and 135° sweep). Measure the
LAA ostium at approximately
these angles:
- at 0° measure from coronary artery marker to a point 2 cm from tip of the “limbus”
- at 45° measure from top of the mitral valve annulus to point 2 cm from tip of the “limbus”
- at 90° measure from top of the mitral valve annulus to a point 2 cm from tip of the “limbus”
- at 135° measure from top of the mitral valve annulus to a point 2 cm from tip of the “limbus”
Measured maximum LAA ostium width must be ≥17 mm or ≤31mm to accommodate available device size
SH-303719-AB June 2015
D) Patient Flow through LAAC Procedure
Scheduling Patients
1)
2)
3)
4)
Schedule pre-procedure diagnostic studies, labs, echo, etc.
Schedule procedure date (LAA day) for lab time, implanter, anesthesia, TEE physician, patient, company representative
(LAAC team)
Ensure discharge protocol is understood prior to procedure and re-iterated at discharge
Schedule post-procedure follow-up office visit, labs and TEE
Scheduling Tools / Best Practices
•
•
Dedicated LAA days (operator, anesthesia, echo, lab staff)
Ensure ample inventory and supplies
•
WATCHMAN Checklist
•
Ensure patient understands pre and post procedure expectations
•
Standard Discharge worksheet
SH-303719-AB June 2015
D) Patient Flow through LAAC Procedure
Pre
Procedure
SH-303719-AB June 2015
Procedure
Post
Procedure
D) Patient Flow through LAAC Procedure
Pre-Procedural Screening
-
-
Understanding the indication and patient selection is key
- Ensure patient qualifies for a WATCHMAN
- Imaging requirements (size, thrombus, etc)
Educate patient and family on procedure
Consent patient
Pre-Procedural Screening Tools / Best Practice
-
Download Central (click above)
- Patient Education Material
- Sample Documents (WATCHMAN homework and Information Sheet)
SH-303719-AB June 2015
D) Patient Flow through LAAC Procedure
Procedure Understanding
•
Download Central (click above)
• Procedure explanation & video (click above)
Understanding of Potential Complications
•
•
•
•
Pericardial Effusion
Device Migration
Peri-Procedural CVA
Assess complication
SH-303719-AB June 2015
D) Patient Flow through LAAC Procedure
Post Procedure
-
•
-
Patient Post Procedure
- Hospital Stay
- 1 night overnight (in most cases)
- Follow Up Office Visits
- Follow Up Office visit 7 – 10 post procedure (or your protocol)
- TEE Follow Up at 45 days
- Drug Regimen
- Recommended (next page)
SH-303719-AB June 2015
Coordinator / Hospital Post Procedure
- Data collection for internal database/required registry
- Discharge Instructions completed by NP / Physician
- Follow up and TEE scheduled
- Update Referral MD on procedure and patient outcome
SH-303719-AB June 2015
C) Patient Flow through LAAC Procedure
Post-Procedural Information (found in DFU)
1. Post-procedure warfarin therapy is required in ALL patients receiving a WATCHMAN Device. Patients should remain on
81-100 mg of aspirin and warfarin should be taken post-implant (INR 2.0-3.0). At 45 days (±15 days) post-implant, perform
WATCHMAN Device assessment with TEE. Cessation of warfarin is at physician discretion provided that any peri-device
flow demonstrated by TEE is ≤5 mm. If adequate seal is not demonstrated, subsequent warfarin cessation decisions are
contingent on demonstrating flow ≤5 mm. At the time the patient ceases warfarin, the patient should begin clopidogrel 75 mg
daily and increase aspirin dosage to 300-325 mg daily. This regimen should continue until 6 months
have elapsed after implantation. Patients should then remain on aspirin 300-325 mg indefinitely. If a patient remains on
warfarin and aspirin 81-100 mg for at least 6 months after implantation, and then ceases warfarin, the patient should not
require clopidogrel, but should increase to aspirin 300-325 mg daily, which should be taken indefinitely.
2. At 45 days and 12 months: assess WATCHMAN Device with TEE.
Confirm absence of intra-cardiac thrombus.
Perform color Doppler assessment to include the device/LAA border at the following approximate TEE angles (0°, 45°,
90° and 135°). Measure any residual leak around the device if necessary.
If thrombus is observed on the device, warfarin therapy is recommended until resolution of thrombus is demonstrated by
TEE.
3. Prescribe appropriate endocarditis prophylaxis for 6 months following device implantation. The decision to continue
endocarditis prophylaxis beyond 6 months is at physician discretion
SH-303719-AB June 2015
C) Patient Flow through LAAC Procedure
SH-303719-AB June 2015
E) Patient Selection
SH-303719-AB June 2015
E) Patient Selection
INDICATIONS FOR USE
The WATCHMAN Device is indicated to reduce the risk of
thromboembolism from the left atrial appendage in patients with
non-valvular atrial fibrillation who:
– Are at increased risk for stroke and systemic embolism based on
CHADS2 or CHA2DS2-VASc[1] scores and are recommended for
anticoagulation therapy;
– Are deemed by their physicians to be suitable for warfarin; and
– Have an appropriate rationale to seek a non-pharmacologic alternative
to warfarin, taking into account the safety and effectiveness of the
device compared to warfarin
SH-303719-AB June 2015
E) Patient Selection
PATIENT SELECTION FOR TREATMENT
•
Selection among available treatment options must first take into account whether anticoagulation is indicated to reduce
the risk of stroke based on CHADS2 or CHA2DS2-VASc scores. Next, in a patient who is deemed by their physicians to
be suitable for anticoagulation with warfarin, physicians and patients should consider the rationale for implantation of the
WATCHMAN Device as an alternative to long-term warfarin therapy. Specific factors may include one or more of the
following:
– A history of major bleeding while taking therapeutic anticoagulation therapy.
– The patient’s prior experience with oral anticoagulation (if applicable), which may include an inability to maintain a
stable therapeutic International Normalized Ratio (INR) or inability to comply with regular INR monitoring AND
unavailability of an approved alternative anticoagulation agent.
– A medical condition, occupation, or lifestyle placing the patient at high risk of major bleeding secondary to trauma.
Some studies of patients with a history of falls, or at risk for falls and head trauma, have shown that the benefits of
anticoagulation therapy to reduce the risk of stroke outweigh the risk of major, life-threatening bleeding. An
individualized benefit and risk assessment should be made in such patients.3, 4, 5
– The presence of indication(s) for long-term warfarin use, other than non-valvular atrial fibrillation (e.g. mechanical
heart valve, hypercoagulable states, recurrent deep venous thrombosis).
•
Specific factors that need to be considered for the WATCHMAN Device and implantation procedure include the following:
– Overall medical status, including conditions which might preclude the safety of a percutaneous, transcatheter
procedure.
– Suitability for percutaneous, trans-septal procedures, including considerations of:
• Cardiac anatomy relating to the LAA size and shape.
• Vascular access anatomy (e.g., femoral vein size, thrombus, or tortuosity.)
• Ability of the patient to tolerate general or local anesthesia.
• Ability of the patient to undergo required imaging.
– Ability to comply with the recommended post-WATCHMAN Device implant pharmacologic regimen, especially for
patients at high risk for bleeding, i.e., the need for warfarin plus aspirin for at least 45 days post-device
implantation, clopidogrel and aspirin through 6 months post-procedure, and aspirin indefinitely.
SH-303719-AB June 2015
E) Patient Selection
• Patients with high risk for ischemic events
• Patients with high risk for bleeding events
• Patients with reasonable anatomy and access
• Patient must be a candidate for long-term anticoagulation
• Reasonably high risk enough for the patient to notice or
comprehend the complications of anticoagulation
SH-303719-AB June 2015
F) Identify and Educate the
Internal and External Referral
Pathways
SH-303719-AB June 2015
Referral Patterns
Within implanter’s practice
Inside the hospital
(EP, IC, clin cards, Neuro, GI, ER)
External Referring centers
(EP, IC, cards, Neuro, GI, ER)
Private practice
(GC, GP, Geriatrics…)
Patients
SH-303719-AB June 2015
Steps to Building Awareness
Begin
Plan your referral strategy and educate your business partners
Act
Publicize through local media and build your referral base
Share
Accelerate adoption by deepening referring physician
understanding
Educate
Guide patient flow through education
SH-303719-AB June 2015
F) Identify and Educate the Internal and External Referral
Pathways
Locate with Atrial Fibrillation
Primary
Care
Provider
Coumadin
Clinic
Primary
Cardiologist
Direct
Referral
SH-303719-AB June 2015
Stroke
Team
LAA
Program
Non
Invasive/EP
F) Identify and Educate the Internal and External Referral
Pathways
Identify Internal & External Referral Pathways
Internal
-
Clinic (current patients)
Afib Clinic (internal) + Coumadin clinic
Cardiologist
AHPs
Geriataric
ER / hospitalist (onset or AFIB / stroke)
EMR Data query (existing patients)
TEE Screening
GI
Neurologist
External
-
Current external referrals (cardiologist,
GPs, GI, Neurologist, etc)
New referrals due to exclusive technology
Educate Internal & External Referral Pathways
Internal
-
Grand rounds
Lunch & Learns
Morning conference
Marketing team (website, newsletter to
internal employees)
SH-303719-AB June 2015
External
-
Marketing team (News, media & print to
external stakeholders)
Dinner engagements
Local society meeting
F) Identify and Educate the Internal and External Referral
Pathways
Referral to Treatment Timeline
48-72 hours
Patient/MD
contacted
Records/preauth initiated
SH-303719-AB June 2015
7 days
Consult with
TTE/TEE
Additional
workup
(Baseline
additional
customary
pre-procedure
testing)
10 days
Presented
w/treatment
plan in place
Research if
appropriate
Scheduled for
pre-procedure
visit
Within 14-28
days
Patient is
treated
F) Identify and Educate the Internal and External Referral
Pathways
Referral Education and Materials
-
-
Download Central (click above)
- Education Tools:
- WATCHMAN Device Overview and WATCHMAN Economic Value Proposition
- Media Kit Tools:
- Hospital Press Release, Hospital Newsletter, Video, Images and Product messaging
- Tools to Engage Referring Physicians
- Email Blast Template, Letter of Introduction, Education Event Invite, Education Event Thank
You letter
Additional Tools
- Therapy Awareness Toolkit (hard copy & electronic)
- Implanters step-by-step instruction & easily accessible tools for how to drive awareness for
their WATCHMAN program with their referring physicians.
SH-303719-AB June 2015
G) Market Yourself as a Center of
Excellence
SH-303719-AB June 2015
Potential Marketing Opportunities
• Use the WATCHMAN™ Device as a proof point for why referring
physicians and their patients should seek out care at your institution
by incorporating the WATCHMAN Device into:
• Hospital website/newsletter
• Newsletters for referring physicians
• Social media outlets
• Identify a patient who was enrolled in the clinical study who would be
willing to share their story
• Consider inviting local media to your institution to coincide with an
implant
• Use a patient story you may have identified
• Interview the implanting physician
• Issue hospital press release
• Engage hospital switchboard so they know who to direct
patients to when asked about stroke/WATCHMAN Device
SH-303719-AB June 2015
The WATCHMAN™ LAA Closure Device is CE Marked and is currently available For Investigational Use Only in the United States. Not for sale in the United States.
Hospital Marketing Resources
• Hospital Press Release Template
• Product Messaging Guide
• Hospital Newsletter Template
• Product Images (.jpg files)
• Implant animation video
• Patient Brochure
• Patient Website
• Patient Testimonials
*** Link to Resources ****
SH-303719-AB June 2015
The WATCHMAN™ LAA Closure Device is CE Marked and is currently available For Investigational Use Only in the United States. Not for sale in the United States.
Summary:
• Starting a left atrial appendage program takes a dedicate team to
support patient flow, LAAC cases and new patients
• Appropriate and optimal patient selection is key to success
• Education at all levels of the hospital: administration, operators,
coordinator, lab, anesthesia, cv surgery, referral community is key to
long term program success
• Build and educate referral pathways to ensure patient flow
SH-303719-AB June 2015
ABBREVIATED STATEMENT
WATCHMANTM Left Atrial Appendage Closure Device
with Delivery System and WATCHMAN Access System
INDICATIONS FOR USE
The WATCHMAN Device is indicated to reduce the risk of thromboembolism from the left atrial appendage in patients with non-valvular atrial fibrillation who:
• Are at increased risk for stroke and systemic embolism based on CHADS2 or CHA2DS2-VASc scores and are recommended for anticoagulation therapy;
• Are deemed by their physicians to be suitable for warfarin; and
• Have an appropriate rationale to seek a non-pharmacologic alternative to warfarin, taking into account the safety and effectiveness of the device compared to warfarin.
The WATCHMAN Access System is intended to provide vascular and transseptal access for all WATCHMAN Left Atrial Appendage Closure Devices with Delivery Systems.
CONTRAINDICATIONS
Do not use the WATCHMAN Device if:
• Intracardiac thrombus is visualized by echocardiographic imaging.
• An atrial septal defect repair or closure device or a patent foramen ovale repair or closure device is present.
• The LAA anatomy will not accommodate a device. See Table 46 in the DFU.
• Any of the customary contraindications for other percutaneous catheterization procedures (e.g., patient size too small to accommodate TEE probe or required catheters) or conditions (e.g., active infection, bleeding disorder) are present.
• There are contraindications to the use of warfarin, aspirin, or clopidogrel.
• The patient has a known hypersensitivity to any portion of the device material or the individual components (see Device Description section) such that the use of the WATCHMAN Device is contraindicated.
WARNINGS
• Device selection should be based on accurate LAA measurements obtained using fluoro and ultrasound guidance (TEE recommended) in multiple angles (e.g., 0º, 45º, 90º, 135º).
• Do not release the WATCHMAN Device from the core wire if the device does not meet all release criteria.
• If thrombus is observed on the device, warfarin therapy is recommended until resolution of thrombus is demonstrated by TEE.
• The potential for device embolization exists with cardioversion <30 days following device implantation. Verify device position post-cardioversion during this period.
• Administer appropriate endocarditis prophylaxis for 6 months following device implantation. The decision to continue endocarditis prophylaxis beyond 6 months is at physician discretion.
• For single use only. Do not reuse, reprocess, or resterilize.
PRECAUTIONS
• The safety and effectiveness (and benefit-risk profile) of the WATCHMAN Device has not been established in patients for whom long-term anticoagulation is determined to be contraindicated.
• The LAA is a thin-walled structure. Use caution when accessing the LAA and deploying the device.
• Use caution when introducing the WATCHMAN Access System to prevent damage to cardiac structures.
• Use caution when introducing the Delivery System to prevent damage to cardiac structures.
• To prevent damage to the Delivery Catheter or device, do not allow the WATCHMAN Device to protrude beyond the distal tip of the Delivery Catheter when inserting the Delivery System into the Access Sheath.
• If using a power injector, the maximum pressure should not exceed 100 psi.
• In view of the concerns that were raised by the RE-ALIGN1 study of dabigatran in the presence of prosthetic mechanical heart valves, caution should be used when prescribing oral anticoagulants other than warfarin in patients treated with the WATCHMAN
Device. The WATCHMAN Device has only been evaluated with the use of warfarin post-device implantation.
ADVERSE EVENTS
Potential adverse events (in alphabetical order) which may be associated with the use of a left atrial appendage closure devi ce or implantation procedure include but are not limited to:
Air embolism, Airway trauma, Allergic reaction to contrast media/medications or device materials, Altered mental status, Anemia requiring transfusion, Anesthesia risks, Angina, Anoxic encephalopathy, Arrhythmias, Atrial septal defect , AV fistula , Bruising,
hematoma or seroma, Cardiac perforation , Chest pain/discomfort, Confusion post procedure, Congestive heart failure, Contrast related nephropathy, Cranial bleed, Decreased hemoglobin, Deep vein thrombosis, Death, Device embolism, Device fracture, Device
thrombosis, Edema, Excessive bleeding, Fever, Groin pain, Groin puncture bleed, Hematuria, Hemoptysis, Hypotension, Hypoxia, Improper wound healing, Inability to reposition, recapture, or retrieve the device, Infection / pneumonia, Interatrial septum thrombus,
Intratracheal bleeding, Major bleeding requiring transfusion, Misplacement of the device / improper seal of the appendage / movement of device from appendage wall, Myocardia erosion, Nausea, Oral bleeding, Pericardial effusion / tamponade, Pleural effusion,
Prolonged bleeding from a laceration, Pseudoaneurysm, Pulmonary edema, Renal failure, Respiratory insufficiency / failure, Surgical removal of the device, Stroke – Ischemic , Stroke – Hemorrhagic, Systemic embolism, TEE complications (throat pain, bleeding,
esophageal trauma), Thrombocytopenia, Thrombosis, Transient ischemic attack (TIA), Valvular damage, Vasovagal reactions
There may be other potential adverse events that are unforeseen at this time.
CAUTION: Federal law (USA) restricts this device to sale by or on the order of a physician. Rx only. Prior to use, please see the complete “Directions for Use” for more information on Indications, Contraindications, Warnings, Precautions, Adverse Events, and
Operator’s Instructions.
© 2015 Boston Scientific Corporation or its affiliates. All rights reserved.
1Eikelboom
JW, Connolly SJ, Brueckmann M, et al. N Engl J Med 2013;369:1206-14.
SH-303719-AB June 2015
 Program - Boston Scientific")