I-29_Fleischer - Advocate Health Care
advertisement

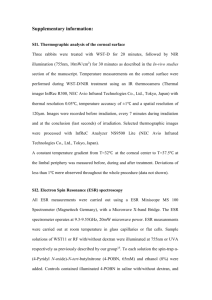
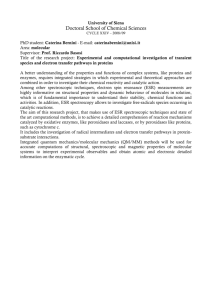
Serum Inflammatory Markers in the Diagnosis of Diabetic Foot Osteomyelitis: A Meta-Analytic Review Adam Fleischer, DPM, MPH, Maureen Allanson, BS, James Wrobel, DPM, MS Department of Surgery, Advocate Illinois Masonic Medical Center Abstract: Introduction: The aim of this meta-analytic review was to help establish optimal cut-off levels when using erythrocyte sedimentation rate (ESR) and Creactive protein (CRP) in the diagnosis of diabetic foot osteomyelitis (OM). A secondary aim was to determine whether these simple diagnostic tests demonstrate more of a “threshold effect” or “dose-response” when discriminating between patients with and without OM. Methods: Six eligible articles were identified through a search of Medline and EMBASE electronic databases from 1966 to 2010. Summary likelihood ratios for predicting the presence of OM in the case of both a positive test result (LR+, sensitivity/1-specificity) and negative test result (LR-, 1sensitivity/specificity) were calculated along with 95% confidence intervals (CIs) using random-effects models for several commonly reported thresholds for ESR and CRP. Mantel-Haenszel test was used to test for dose-response as thresholds were increased given a positive result (LR+) and decreased for a negative result (LR-). Results/Conclusion: ESR > 80mm/h proved to be the best threshold and test for ruling in OM (LR+ 9.40 [95% CI 0.65 - 135). Furthermore, there was an obvious dose-response with increasing ESR levels, and a three-fold increase in the likelihood of OM as ESR levels increased from 60mm/h to 80mm/h (p = 0.04). CRP ≤ 3.2mg/dl proved to be the best blood test for ruling out OM (LR- 0.23 [95% CI 0.17-0.52]), however, unlike ESR, CRP demonstrated more of a threshold effect in the diagnosis of OM as increasing and decreasing levels did not appear to alter the likelihood of having underlying OM significantly (p > 0.05). Articles were included for review if they fulfilled all of the following criteria: Data could be extracted into 2x2 tables The diagnostic test was compared with a reference standard. There were a total of 305 patients represented in this meta-analysis. The majority of these people were inpatients with a mean prevalence of OM of 59%. Table 1. Studies Describing CRP or ESR in the Diagnosis of Lower Extremity Osteomyelitis in Patients with Diabetes Mellitus In studies that included patients with and without DM, only those patients with DM were included in the analysis. Summary likelihood ratios for predicting the presence of OM in the case of both a positive test result and negative test result, as well as sensitivities and specificities were calculated using random-effects models for several commonly reported thresholds for ESR and CRP. The Mantel-Haenszel test for trend was used to test for dose-response as thresholds were increased given a positive result and decreased for a negative result. P values less than 0.5 were considered significant. All analyses were performed using SAS version 9.2 for Windows. Malabu et al 2007 Results: Introduction: Our original search yielded 152 potential articles of which 19 were selected for review by the authors. Fourteen articles were excluded: 9 articles did not use ESR or CRP in the diagnosis of osteomyelitis and the data could not be extracted in the remaining 5. Our reference search provided us with an additional 35 articles; however only 1 of these articles fulfilled all of the inclusion criteria mentioned previously. NS Ertugrul et al 2009 II Prospe ctive Yes III Retros pective No 56.3 54 0 61.0 69 100 Pathology or radiographs or Technitium-99 three phase bone scans 64.0 52 54 Histopathology or microbiological culture or T1 weighted MRI scan 100 Histopathology (focal necrosis or intramedullary fibrosis with infiltration of neutrophils) 61.5 63 resonance imaging, NS, Not specified, OM, osteomyelitis *Level I: independent, blind evaluation of test with gold standard among a large sample of consecutive patients with suspected target condition.. Level II: independent, blind evaluation of test with gold standard among a small sample of consecutive patients with suspected target condition. Level III: nonindependent, blind evaluation of test with gold standard among a nonconsecutive group of patients with suspected condition. Level IV: nonindependent evaluation of test with standard of uncertain validity among a sample of patients who have the target condition. Level V: nonindependent evaluation of test with standard of uncertain validity among a sample of patients † Calculations based on number of ulcers Methods: Figure 1. Search strategy All six articles examined ESR’s relation to diabetic osteomyelitis however, only one article, Fleischer et al 2009, described CRP thresholds. The search was limited to studies involving adults and English language articles from the period 1966 through 27 June 2010. The articles we examined were of fair to poor quality generally. Two-thirds of the studies were prospective. We identified additional articles through a hand search of references from retrieved articles, previous reviews, and polling experts. The titles and abstracts of the articles retrieved were evaluated to determine their eligibility for our review. Publications in abstract and letter form were included to minimize publication bias. None of the article displayed level one evidence and only two studies reported consecutive patient enrollment. All but one of the studies used bone histopathology to diagnose osteomyelitis; however, Kaleta et al and Ertrugal et al utilized the histopathology goldstandard inconsistently at about 55% of the time. ESR > 80mm/h was identified as the single most specific laboratory test for diagnosing OM (spec=94.2%). There was an obvious dose-response observed for the likelihood of underlying OM with increasing ESR thresholds, and a three-fold increase in the likelihood of OM as ESR threshold was increased from 70mm/h to 80mm/h (3.11 -> 9.40). This trend was statistically significant using the Mantel-Hanszel test with a p value of 0.04 (Table 2). Table 2. Summary Characteristics for Erythrocyte Sedimentation Rate for Diagnosing Osteomyelitis ESR threshold n Sensitivity Specificity >60 mm/h 129 80.5 (74.0-85.8) 73.1 (63.4-80.9) >70 mm/h 267 64.7 (60.6-68.0) 82.5 (75.3-88.2) >80 mm/h 129 62.3 (56.8-64.9) 94.2 (86.1-98.0) Search strategy III Prospe ctive NS Positive results of two imaging modalities (bone scan, MRI, radiographs) or positive probe to bone Table 1. Abbreviations: CRP, C-reactive protein, ESR, Erythrocyte sedimentation rate, MRI, magnetic To better characterize how ESR and CRP might be used in the diagnosis of diabetic foot OM. Rabjohn et al 2007 Fleischer et al 2009 Purpose We searched MEDLINE and EMBASE databases with the following search terms: “diabetic” and “osteomyelitis” or “diabetic” and “ulcer”, in addition to each of the following words: C-reactive protein and erythrocyte sedimentation rate. Prospe ctive In total, six articles were included in our meta-analysis (Figure 1). Diabetes mellitus (DM) is a significant public health concern, with an estimated 23.6 million people affected in the US alone. The US spends approx. $174 billion, or ~1 out of every 5 healthcare dollars, on patients with diabetes annually. Foot-related complications in the form of ulceration and infection are the leading cause of hospitalization and lower extremity amputation (LEA) in patients with diabetes, costing the US healthcare system $43,000 to $63,000 per event. Early recognition of diabetic OM may curtail the need for LEA, however, confirmatory tests such as biopsy are invasive. Diagnostic tests such as MRI are expensive and not always available and standard radiographs lack sufficient sensitivity to accurately diagnose early OM. Therefore, simple laboratory tests of common serum inflammatory markers (e.g., ESR, CRP) have been proposed as diagnostic aids, but there is uncertainty regarding their usefulness in DM OM, and it is unclear whether or not these tests demonstrate either a dose response or threshold effect. IV Patients with foot ulcer (n=43) Inpatients with clinically suspected osteomyeli tis (n=95) Inpatients with diabetic foot lesions (n=46) Inpatients with a single forefoot ulceration (n=54) LR (+)* 2.89 (0.38-21.5) 3.11 (1.21-7.99) 9.40 (0.65-135) LR (-)† 0.245 (0.24-2.56) 0.424 (0.178-1.01) 0.365 (0.03-5.26) Table 2. Data in parentheses represent 95% confidence intervals. Abbreviations: LR (+), positive likelihood ratio; LR (-), negative likelihood ratio; ESR, erythrocyte sedimentation rate *Mantel Haenszel test for trend with increasing threshold levels = 4.041, p = 0.044 †Mantel Haenszel test for trend with decreasing threshold levels = 0.636, p = 0.425 Table 3. Summary Characteristics for C-Reactive Protein for Diagnosing Osteomyelitis CRP threshold n Sensitivity Specificity 2.3 mg/dl 54 88.0 (79.6-94.7) 40.0 (25.3-51.0) 3.2 mg/dl 54 85.3 (75.7-92.2) 65.0 (48.7-76.8) 8.4 mg/dl 54 55.9 (45.9-62.5) 80.0 (63.0-91.3) LR (+)* 1.47 (0.10-2.84) 2.44 (1.12-3.76) 2.79 (1.51-4.08) LR (-)† 0.29 (0.21-0.49) 0.23 (0.17-0.52) 0.55 (0.32-1.90) Table 3. Data in parentheses represent 95% confidence intervals Level of Study Consecutive Prevalence of Biopsy, Source Evidence* Type Enrollment Population Age OM, % % Method of Diagnosis of OM Inpatients and outpatients Culture and/or pathologic criteria with foot (osteonecrosis, marrow fibrosis, Newman Prospe ulcer and/or presence of inflammatory et al 1991 II ctive Yes (n=35) 55.0 cells) 68† 100† Inpatients with osteomyeli Pathology , positive results of at tis or least two imaging modalities (bone Kaleta et Retros cellulitis scan, MRI, radiographs), or positive al 2001 IV pective No (n=29) 62.0 66 53 probe to bone Statistical Analysis Background They were original studies describing CRP or ESR in the diagnosis of lower extremity osteomyelitis in patients with DM Neither increasing nor decreasing levels of CRP demonstrated a dose response for diagnosing OM as evident by the nonsignifcant Mantel-Haenszel test. CRP 3.2 mg/dl was the best threshold for diagnosing OM with the highest combined total or sum for sensitivity and specificity of 85.3 and 65.0 respectively. Abbreviations: LR (+) , positive likelihood ratio; LR (-), negative likelihood ratio; CRP, C-reactive protein *Mantel Haenszel test for trend with increasing threshold levels = 1.236, p = 0.266 †Mantel Haenszel test for trend with decreasing threshold levels = 1.381, p = 0.240 As CRP threshold (green arrow) for establishing OM is raised from 2.3 to 3.2 to 8.4, the likelihood of getting a true positive compared to a false positive remains essentially the same, indicating that CRP may demonstrate more of a threshold effect for diagnosing underlying OM (Figure 2). However, this is not true of ESR. As the ESR threshold (blue arrow) for diagnosing OM is increased from 60 to 70 to 80, the likelihood of getting a false positive decreases significantly as the likelihood of getting a true positive remains relatively constant. This trend suggests that ESR demonstrates more of a dose response likelihood of OM with increasing levels (Figure 3). Figure 2. Summary receiver operating characteristic curves for CRP (from Fleischer et al. 2009, unpublished figure, n=54). Figure 3. Summary receiver operating characteristic curves for ESR (from Fleischer et al. 2009, unpublished figure, n=54). Conclusions: 1. ESR demonstrates a dose-response likelihood of having underlying OM with increasing levels (p=0.04); however CRP does not show this same pattern (p=0.266). 2. The likelihood of having OM increased three-fold as the ESR threshold was increased from 70 mm/h to 80 mm/h. 3. CRP, on the other hand, demonstrates more of a threshold effect in the diagnosis of OM, with 3.2 mg/dl being the optimal cut-point. 4. ESR appears to be a specific marker for diabetic OM, with increasingly higher LR+ values at higher threshold levels (p<0.05). An elevated ESR above 80 mm/h strongly favors the diagnosis of OM (LR+ 9.40). 5. CRP, conversely, appears to be a sensitive marker for diabetic OM, with values lower than 3.2 effectively ruling out underlying OM (LR- 0.23). 6. Because serum inflammatory markers, by themselves, lack accuracy, we believe they will be most useful in modulating our pre-test probability for OM prior to considering our more formal diagnostic (MRI, radiographs) or confirmatory tests (biopsy/culture). References: Ertugrul, BM, Savk, O, Ozturk, MC, Oncu, S, Sakarya, S. The diagnosis of diabetic foot osteomyelitis: Examination findings and laboratory values. Med Sci Monit 15: 307312, 2009. Fleischer, AE, Didyk AA, Woods, JB, Burns, SE, Wrobel, JS, Armstrong, DG. Combined clinical and laboratory testing improves diagnostic accuracy for osteomyelitis in the diabetic foot. J Foot Ankle Surg 48:39-46, 2009. Kaleta, JL, Fleischli, JW, Reilly, CH. The diagnosis of osteomyelitis in diabetes using erthorcyte sedimentation rate: A pilot study. J Am Pod Med Assoc. 91:445-450, 2001. Malabu, UH, Al-Rubeaan, KA, Al-Derewish, M. Diabetic foot osteomyelitis: Usefulness of erythrocyte sedimentation rate in its diagnosis. West Afr J Med 26:113-116, 2007. Newman, LG, Waller J, Palestro, CJ, Schwartz, M, Klein, MJ, Hermann, G, Harrington, E, Harrington, M, Roman, SH, Stagnaro-Green, A. Unsuspected osteomyelitis in diabetic foot ulcers: Diagnosis and monitoring by leukocyte scanning with indium in 111 oxyquinoline. J Am Med Soc 266:1246-1251, 1991. Rabjohn, L, Roberts, K, Troiano, M, Schoenhaus, H. Diagnostic and prognostic value of erythrocyte sedimentation rate in contiguous osteomyelitis of the foot and ankle. J Foot Ankle Surg. 46:230-237, 2007.