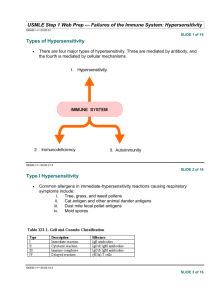
Immunology Stack

Immunology Stack
Slackers Facts by Mike Ori
Disclaimer
The information represents my understanding only so errors and omissions are probably rampant. It has not been vetted or reviewed by faculty. The source is our class notes.
The document can mostly be used forward and backward. I tried to mark questionable stuff with (?).
If you want it to look pretty, steal some crayons and go to town.
Finally…
If you’re a gunner, buck up and do your own work.
B and T Cell progenitor cell
Pre-lymphoid
HSC stem cell markers
CD34 (stem cell factor?), CD133
Myeloid progenitor descendents
Granulocytes (Neutrophils, monocytes,
Basophils, Eosinophiles)
Erythrocytes
Platelets
Myeloid Lineage Cytokines
IL-3, IL-5, GM-CSF
Lymphoid Lineage Cytokines
IL-3, IL-7
B Cell Markers
CD19, CD20
Plasma Cell Markers
CD38
Immature B Cell Ig
Early: Heavy chain + psuedo-light chain
Late: IgM with heavy and light chains
Mature B Cell Ig
IgM, IgD
Common T-Cell Marker
CD3
T Helper Markers
CD4
CD3 (all T’s)
Cytotoxic T Cell Marker
CD-8
CD-3 (all T’s)
B Cell Maturation Site
Bone marrow
T Cell maturation site
Thymus
Congenital lack of thymus, low T cell count, low
IgG (?)
DiGeorge syndrome
T cell receptor subunits
Alpha-beta on CD-4, CD-8
Gamma-delta (not discussed)
Isotype
The major class of an antibody (IgM, IgG, etc)
Allotype
Allelic type changes between Ig of the same isotype.
Idiotope
Antigenic determinant associated with the variable region.
Idiotype
Sum of all idiotopes
Anti-idiotype
The molecule that fits in the idiotype
Domain
A globular region on an antibody consisting of
100-110 amino acids
Hypervariable Region
The area of an antibody subject to recombination and to somatic hypermutation
Complementarity determining region
Antigen
A compound recognizable by antibodies
Immunogen
An antigen capable of creating an immune response
Epitope
The part of an antigen that an antibody recognizes
Paratope
The portion of an antibody that binds the antigen
Hapten
A small molecule that is able to cause an immune response only when bound to a carrier
Carrier
A molecule that can bind haptens in way that can elicit an immune response
Heavy chain types
Chains are defined by the type of Ig created
(M,A, etc)
Light chain types
Kappa and lambda
Light chain rearrangement order
Kappa then lambda
Four chances
Heavy chain rearrangement order
Random. Either the maternal or paternal rearranges. Two chances
Hinge region function
Contributes flexibility to the antibody. Protein cleavage location.
Antibody Fab region function
Binds the antigen
Fc region funciton
Conveys the non-antigen binding properties of the antibody
J chain function
Joins antibody monomers
Secretory protein function
Binds dimeric IgA at the cell surface allowing for transcytosis
Monomeric Ig with complement binding region
IgG
Monomeric Ig without complement binding region
IgE
Pentameric Ig
IgM
Dimeric Ig
IgA
Most abundant Ig in the body (total)
IgA
Most abundant Ig in the serum
IgG
IgG half life
23 days
Transplacental antibody
IgG
Affinity
The strength of interaction between a single hapten or epitope and an antibody.
Avidity
The sum affinity of an antibody
Mucosal surface antibody
IgA
Ig of initial infection
IgM
Breast milk associated antibody
IgA
Principle light and heavy chain binding method
Disulfide bonds
Name the heavy chain variable segments
V – D – J
Name the light chain variable segments
V – J
Heavy chain reorganization scheme
D-J combine then V combines with VDJ
Light chain reorganization scheme
VJ recombine
Since there are only two regions, they combine directly.
What is the function of recombination signal sequence
Sit before and after each segment serving as homology regions that assist in removal of segments.
What is the function of recombinase activating genes
Recombination proteins that excise regions flanked by RSS regions.
What is combinatorial diversity
Antibody diversity generated by recombining V –
D – J segments
Junctional diversity
Diversity generated by repair of imprecise joins as a result of RSS excision
What is somatic hypermutation
Introduction of point mutations during B cell clone development
IgM -> IgE class switching cytokine
IL-4
IgM to IgG class switching cytokine
Interferon ??
Cell causing class switching
CD4 T Helper
Name the complement pathways
Alternative
Classical
Lectin
Complement functions?
Opsonization and neutrophil/macrophage activation (C3b)
Lysis (MAC)
Activation of mast cells (C3a/C5a)
Chemotaxis (C5a > C3a)
B cell function
When activated, become antibody secreting plasma cells
CD4+ T cell function
Create cytokines that activate other immune system components. Can have some direct antimicrobial effects
CD-8 T cell function
Destroy host cells displaying antigens on MHC-I.
Secrete pore forming and proteolytic enzymes under influence of IFN-gamma (and TNFalpha?)
T Regulatory cell marker
CD 4
T Regulatory cell function
Regulate the action of the immune system to prevent autoimmunity
CD4 TH cell classes
TH1 – Viral association
TH2 – allergy/parasite association
TH17 – autoimmune association
MCH used to display intracellularly derived protein fragments
MHC-I
MHC used to display extracellularly derived protein fragments
MHC-II
Proteasome function
Degrades intracellularly derived peptides
TAP function
Passes proteasome processed proteins into the
ER for display by MHC-I molecules.
MHC-I structure
MHC-II structure
MHC-I peptide fit
Fits peptides up to 10 amino acids in length.
Has closed ends. Peptides interact with pockets that determine the fit.
MHC-II peptide fit
Fits peptides up to 20 amino acids in length.
Has open ends. Peptides interact with pockets that determine the fit
MHC-II presenting cells
Dendritic cells
Macrophages
B cells
Thymic epithelial cells
MHC-I presenting cells
All cells
CD-28 to CD-80/86 function
Signals interaction of TCR with MHC is occurring with an APC. This activates the cell.
CD-28 to CTLA-4 interaction
Signals interaction of TCR with MHC is occurring with a non APC cell. This sparks anergy.
Adjuvant
A substance which when mixed with an immunogen improves the immune response to the immunogen
MHC inheritance
Usually inherited as haplotypes due to chromosomal colocation and proximity.
Hence 50% homology(word?) with each parent.
MHC Expression
Codominant expression with both parental haplotypes
MHC-I Gene nomenclature and quantity
A,B,C genes
MHC-II Gene nomenclature and quantity
Three pairs of alpha and beta genes. DP, DQ, DR.
T cell signal 1
MHC-II interaction with APC stimulating T cell activity
T Cell signal 2
Co-stimulation of T cell by B7 (apc) and CD28 (T cell) that stimulates T cell activity
T cell signal 3
Signals by cytokines from presenting or adjacent
APC that stimulate T cell activity
Immunologic synapse
TCR, CD4/8, and co-stimulatory molecule clusters at the point of contact between APC and T cell.
Perforin function
CD8 T cell product that forms pores in plasma membranes.
Granzyme function
Proetolytic enzymes released from CD8 cells
TH1 cytokines
IL-2
IFN-gamma
TH2 Cytokines
IL-4,5,6,10
TH17 cytokines
IL-17,23
Treg cytokines
CTLA-4
IL-10
Type I hypersensitivity characteristic
Antigen IgE interaction
Type II hypersensitivity characteristic
Antibody complexes form on cell surface antigens. Complement fixation/opsonization results in cell death.
Type III hypersensitivity characteristics
Circulating antibody/antigen complexes deposit in kidney glomeruli, eyes, synovium of joints, choroid plexus, skin
Type IV hypersensitivity characteristics
TH1 mediated activation of macrophages in response to self or modified self antigens presented by tissue macrophages
Type I Hypersensitivity Examples
Allergic rhinitis
Allergic asthma
Urticaria
Eczema
Systemic anaphylaxis
Type II hypersensitivity examples
Goodpasture’s syndrome
Transfusion reactions
Erythroblastosis fetalis
Autoimmune hemolytic anemia
Rheumatic fever
Hyperacute graft rejection
Type III hypersensitivity examples
SLE
Arthus Reaction
Serum sickness
Rheumatoid arthritis
Farmers lung
Type IV hypersensitivity types/examples
Contact hypersensitivity
Tuberculin hypersensitivity
Granulomatous hypersensitivity
Jones Mote Hypersensitivity
Cutaneous basophil activation
Jones-mote type IV hypersensitivity
Reddening, edema, necrosis following repeated intradermal injections at a site
Arthus reaction
Molecular Mimicry
When a portion of a protein from an infectious agent mimics a self protein such that cross reactions can occur
What cell type is thought to control autoimmunity
T-reg (CD4 subset) cells
What cells are thought to play a role in developing autoimmunity
TH17 CD4 cells
Estrogen’s role in autoimmunity
Induces IFN-gamma and can push TH2 responses to TH1 responses leading to TH1 mediated diseases like MS
B Cell defect sequelae
Recurrent pneumonia, sinusitis, septicemia
T Cell defect sequelae
B cell defect
Wide ranging opportunistic infection with viruses, bacteria, protozoa
Think about AIDS related disease
Neutrophil defect sequelae
Recurrent oral ulceration
Recurrent fever
Recurrent bacteremia
Complement defect <=C3/C4
Recurrent pyogenic infection
Autoimmune disease
Complement defect >= C5
Recurrent Neisserial infection
Complement C9 defect
No known disease
Low T cell count due to congenital absence of thymus
DiGeorge Syndrome
Cr22 deletion
Defective gamma chain for IL-2 receptor
X-linked SCID due to defective intracellular signaling
Adenosine deaminase deficiency
SCID due to enzymatic defect
Absence of T and B cells
Sever combined immunodeficiency
Deficiency causing frequent pyogenic infections such as pneumonia with low Ig
Lack of B cell activity
Deficiency causing frequent viral or intracellular bacterial infection
T cell deficiency
Hyper IgM cause
Defect in T cell class switch signaling to B cells.
Can result from T cell or B cell defects in
CD40L/CD40, IL-4/Receptor, IL-2/Receptor
Histamine effects
Bronchial constriction
Vasodilation
Increased mucous secretion
Pemphigus vulgaris detail
Type II hypersensitivity that attacks desmosomes in the epidermis resulting in blistering, scaling, and separation of the layers of the epidermis.
Bullous pemphigoid details
Type II hypersensitivity reaction against hemidesmosomes in the dermal/epidermal junction resulting in blistering.
B=between layers
Hemolytic anemia hypersensitivity details
Type II reaction by preformed isohemagglutinins in the blood directed against A,B, Rh blood groups
Type II hypersensitivity immune complex deposition characteristics
Smooth, ribbon-like deposition of Ab in the glomerulus or other structures as a result of binding cellular Ag present in the structure
Type III hypersensitivity immune complex deposition characteristics
Lumpy deposition of immune complexes in the glomerulus due to deposition of preformed
Ab/Ag complexes
Hypotension, rapid heart rate, bronchiole constriction, laryngeal obstruction, pulmonary edema is a sign of what?
Anaphylaxis
Anaphylaxis mechanism
Antigens reach the blood stream and activate basophils by interacting with IgE bound to their surface. This results in massive histamine release as a consequence of degranulation.
Type IV skin test positive sign
Induration
What is a forward blood cell typing test
Mixture of pt RBC with known anti-sera to directly read the pt blood type
What is a reverse blood cell typing test
Addition of pt sera to known A,B,O,Rh blood cells. Yields the Ab’s the patient has. Can infer the PT type.
InfeR=Reverse
What is the purpose of a direct antiglobulin test
AKA Coombs test
Detects antibodies already directly bound to PT
RBC’s. Can confirm reason for hemolysis
Wash cells
Add anti-human IgG
Observe clumping
What is the purpose of the indirect antiglobulin test
Detects antibodies in the patient serum. Used in prescreening to prevent hemolytic reaction
Add serum to antigenic RBC
Incubate and wash
Add anti-human IgG
Observe clumping
Autograft definition
Transplant of one’s own tissues to a new site in the body. CABG donation from leg veins.
Isograft defintion
Transplant of tissue from a genetically identical individual. In mice this occurs in highly inbred strains. In humans it can only occur in monozygotic (identical) twins.
Allograft definiton
Transplantation of tissue between genetically distinct members of the same species
Xenograft definition
Transplant of tissue between members of different species.
Histocompatibility
Sharing histocompatibility markers.
Graft vs Host Disease (GVHD) defintion/cause
T cells in a graft react against host tissue to cause disease. Usually thought of in the context of stem cell transplant but may also occur in other types of transplants.
What is the major rejection mediator cell
CD4 T Helpers
Rank the MHC classes in order of rejection importance
MHC-II – most important
MHC-I – least important
NOTE: ABO Rh are the most important overall
Hyperacute graft rejection characteristics
Occurs within minutes of establishing blood flow to a transplanted organ as a result of isohemagglutinins interaction with blood type antigens on the surface of endothelial tissue.
Cannot be stopped.
Accelerated graft rejection characteristics
Rejection beginning within 2-5 days post transplant as a result of prior sensitization to antigens on donor cells. Spin up of previous memory cells. Generally cannot be stopped.
Acute graft rejection characteristics
Rejection beginning 7-21 days post transplant as a result of HLA mismatch induced activation of
T cells. Generally can be suppressed by interfering with T cell function. Usually involves skin, GI tract, liver but not connective tissue.
Chronic graft rejection characteristics
Graft rejection after 3 months due to disruption of graft tolerance. Generally cannot be reversed. Typically involves skin, GI tract, liver, and connective tissue.
Cyclosporin effects
Suppressed production of IL-2 by T helpers
GVHD symptoms
Early: diarrhea, jaundice, rash, platelet consumption
Late: Anorexia, scaly rash, dry mouth, dry eyes, liver dysfunction