Methamphetamine: New Knowledge about the Epidemic
advertisement

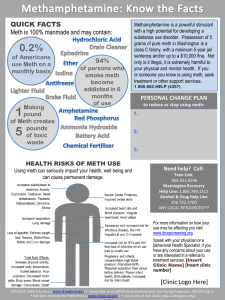
Methamphetamine: New Knowledge about the Epidemic, the Neurobiology and Clinical Issues Richard A. Rawson, Ph.D, Professor Integrated Substance Abuse Programs Semel Institute for Neuroscience and Human Behavior David Geffen School of Medicine University of California at Los Angeles www.uclaisap.org rrawson@mednet.ucla.edu Supported by: National Institute on Drug Abuse (NIDA) Pacific Southwest Technology Transfer Center (SAMHSA) United Nations Office of Drugs and Crime Methamphetamine Methamphetamine is a powerful central nervous system stimulant that strongly activates multiple systems in the brain. Methamphetamine is closely related chemically to amphetamine, but the central nervous system effects of methamphetamine are greater. Forms of Methamphetamine Methamphetamine Powder IDU Description: Beige/yellowy/off-white powder Base / Paste Methamphetamine IDU Description: ‘Oily’, ‘gunky’, ‘gluggy’ gel, moist, waxy Crystalline Methamphetamine IDU Description: White/clear crystals/rocks; ‘crushed glass’ / ‘rock salt’ EPHEDRINE H H C C OH CH3 H H C C H CH3 H N CH3 METHAMPHETAMINE H N CH3 Scope of the Methamphetamine Problem Worldwide According to surveys and estimates by WHO and UNODC, methamphetamine is the most widely used illicit drug in the world except for cannabis. World wide it is estimated there are over 26 million regular users of amphetamine/methamphetamine, as compared to approximately 16 million heroin users and 14 million cocaine users Methamphetamine The US Epidemic Figure 1. Methamphetamine/Amphetamine Treatment Admission Rate per 100,000 Population Aged 12 or Older: 1992-2002 Source: 2002 SAMHSA Treatment Episode Data Set (TEDS). The Eastward Spread of Methamphetamine Primary Amphetamine/Methamphetamine TEDS Admission Rates: 1992 (per 100,000 aged 12 and over) > 58 35 - 58 12 - 35 < 12 No data Primary Amphetamine/Methamphetamine TEDS Admission Rates: 1997 (per 100,000 aged 12 and over) > 58 35 - 58 12 - 35 < 12 No data Primary Amphetamine/Methamphetamine TEDS Admission Rates: 2003 (per 100,000 aged 12 and over) Incomplete Data < 5 5 - 59 60-126 127+ The Methamphetamine Epidemic: Admissions/100,000: 1992-2003 It keeps going up 350 300 California 250 Hawaii 200 Iowa 150 Oregon 100 Washington 50 03 20 02 20 01 20 00 20 99 19 98 19 97 19 96 19 95 19 94 19 93 19 19 92 0 Figure 2. Methamphetamine/Amphetamine Treatment Admissions, by Route of Administration: 1992-2002 Source: 2002 SAMHSA Treatment Episode Data Set (TEDS). National Association of Counties (NACo) 2006 Survey of Sheriffs Methamphetamine remains number one drug problem according to new survey of the nation’s counties. Legislation that restricts the sale of precursors works. The majority of meth currently being abused is from outside of the state. The full survey is available at www.naco.org. National Association on Counties (NACo) 2006 Survey of Sheriffs % Sheriffs ranking meth worst problem 100% in Calif, Hawaii, Idaho, Arizona, New Mexico, Wyoming, Washington, Utah, Nevada 88% Oklahoma, Iowa 79%, Louisiana 75% Nebraska 74% 64% Georgia 44% North Carolina 43% Alabama National Association on Counties (NACo) 2006 Survey of Sheriffs Crimes related to meth continue to grow during past year. – 55% of law enforcement officials reported an increase in robberies or burglaries in the last year. – 48 % reported an increase in domestic violence. – 41 % reported an increase in simple assaults. – 31% reported an increase in identity theft crime, which is up from the 27 percent reported in 2005. Methamphetamine: A Growing Menace in Rural America In 1998, rural areas nationwide reported 949 methamphetamine labs. Last year, 9,385 were reported. This year, 4,589 rural labs had been reported as of July 26. Source: El Paso Intelligence Center (EPIC), U.S. DEA Anhydrous Ammonia Tank Tips Officers to Possible Meth Lab 5/4/04 Omaha, Neb. – A large anhydrous ammonia tank helped Sarpy County Sheriff’s deputies bust a suspected methamphetamine lab Tuesday. SOURCE: TheOmahaChannel.com Meth Epidemic; less drama, more long term risk/danger Cocaine/Crack epidemic hit fast (in NYC 1986-87, as well as other major east coast cities); overnight emergency, tremendous media attention. Big federal response (Reagan and Bush I). High visibility deaths, stigmatization as a ghetto drug. Dramatic decreases in indicators by early 1990s, except in inner cites of east coast. Crack epidemic: Rapid onset; Rapid decrease Meth epidemic: Slow west to east spread. No decrease in western cities. Use becomes endemic? Methamphetamine: What does it do? Methamphetamine Acute Physical Effects - Increases Heart rate Blood pressure Pupil size time Respiration Sensory acuity Energy -Decreases Appetite Sleep Reaction Methamphetamine Acute Psychological Effects Increases – Confidence – Alertness – Mood – Sex drive – Energy – Talkativeness Decreases – Boredom – Loneliness – Timidity Methamphetamine Chronic Physical Effects - Tremor - Weakness - Dry mouth - Weight loss - Cough - Sinus infection - Sweating Burned lips; sore nose Oily skin/complexion Headaches Dental Problems Anorexia METH Use Leads to Severe Tooth Decay “METH Mouth” Source: The New York Times, June 11, 20 Meth Use in Hawaii The number of crystal methamphetaminerelated deaths has already doubled in Oahu in the last five years. "You've heard the stories about people on ice who die in confrontations with police, but most ice deaths happen quietly, sending people to the morgue after their bodies just can't keep up with the crystal meth in their systems," Honolulu Chief Medical Examiner Dr. Kanthi De Alwis said. Meth Use in Hawaii As of the middle of May, not even halfway through the year, the city medical examiner's office already recorded 38 deaths connected to crystal methamphetamine. So, we're well on the way to exceeding last year's total of 68. Deaths: 2005 (mid-May) - 38 deaths 2004 - 68 deaths 2003 - 56 deaths 2002 - 62 deaths 2001 - 54 deaths 2000 - 34 deaths Methamphetamine Chronic Psychological Effects - Confusion Concentration Hallucinations Fatigue Memory loss Insomnia - Irritability Paranoia Panic reactions Depression Anger Psychosis Methamphetamine Psychiatric Consequences Paranoid reactions Permanent memory loss Depressive reactions Hallucinations Psychotic reactions Panic disorders Rapid addiction MA Psychosis Inpatients from 4 Countries No. of patients having symptoms (%) Psychotic symptom Lifetime Current Persecutory delusion Auditory hallucinations Strange or unusual beliefs Thought reading Visual hallucinations Delusion of reference Thought insertion or made act Negative psychotic symptoms Disorganized speech Disorganized or catatonic behavior 130 (77.4) 122 (72.6) 98 (58.3) 89 (53.0) 64 (38.1) 64 (38.1) 56 (33.3) 35 75 39 27 38 20 18 36 19 14 (20.8) (44.6) (23.2) (16.1) (22.6) (11.9) (10.7) (21.4) (11.3) (8.3) Srisurapanont et al., 2003 MA Psychosis 69 physically healthy, incarcerated Japanese females with hx MA use – 22 (31.8%) no psychosis – 47 (68.2%) psychosis 19 resolved (mean=276.2±222.8 days) 8 persistent (mean=17.6±10.5 months) 20 flashbackers (mean=215.4±208.2 days to initial resolution) – 11 single flashback – 9 Recurrent flashbacks 2001 Yui et al., Polymorphism in DAT Gene associated with MA psychosis in Japanese 2003 Ujike et al., Source: Skidmore, S. (2006, April 21) Oregon Man Survives 12 Nails to the Head. The Associated Press. 33-year-old man, high on methamphetamine is brought to the ER in Portland Oregon complaining of a severe headache. Doctors did not see any immediate cause for the headache and placed the patient in an exam room and ordered tests including X-rays to rule out head trauma. – The man at first claimed it was an accident, but he later admitted that it was a suicide attempt. – The nails were removed, and the man survived without any serious permanent damage. – He was eventually transferred to psychiatric care; he stayed for almost one month under court order but then left against doctors’ orders MSNBC-TV A Major Reason People Take a Drug is they Like What It Does to Their Brains 200 % of Basal DA Output NAc shell 150 100 Empty 50 Box Feeding 200 150 100 15 10 5 0 0 0 60 120 Time (min) 180 ScrScr BasFemale 1 Present Sample 1 2 3 4 5 6 7 8 Number Scr Scr Female 2 Present 9 10 11 12 13 14 15 16 17 Mounts Intromissions Ejaculations Source: Di Chiara et al. Source: Fiorino and Phillips Copulation Frequency DA Concentration (% Baseline) Natural Rewards Elevate Dopamine Levels FOOD SEX Effects of Drugs on Dopamine Release METHAMPHETAMINE 400 % of Basal Release Accumbens 1000 500 COCAINE DA DOPAC HVA 300 200 100 0 0 1 2 0 3hr Time After Cocaine % of Basal Release Time After Methamphetamine 250 NICOTINE 200 Accumbens Caudate 150 100 250 % of Basal Release % Basal Release 1500 Accumbens Accumbens ETHANOL Dose (g/kg ip) 200 0.25 0.5 1 2.5 150 100 0 0 1 2 3 hr Time After Nicotine 0 0 1 2 3 Time After Ethanol Source: Shoblock and Sullivan; Di Chiara and Imperato 4hr Prolonged Drug Use Changes the Brain In Fundamental and Long-Lasting Ways What Can Imaging Tell Us? In design of new medications – knowledge of affected circuitry can point to chemical dysfunction that may be helped by medication. In the design of behavioral treatments it can tell you the types and severity of deficits and dysfunctions in the brain and the timetable of their recovery (or not). This information can be helpful in guiding the behavioral targets for treatment and the types and durations of treatment that can best accommodate the brain recovery Brain imaging can show how much viable tissue there is to work with. And, it can show the affect of treatment. Brain Function in Methamphetamine Abusers Do meth abusers show abnormalities in brain metabolites? Do brain metabolite abnormalities relate to cognitive performance – such as selective attention? Does the brain recover following cessation of meth use? Decreased dopamine transporter binding in meth users resembles that in Parkinson’s Disease patients Control Methamphetamine PD Source: McCann U.D.. et al.,Journal of Neuroscience, 18, pp. 8417-8422, October 15, 1998. Partial Recovery of Brain Dopamine Transporters in Methamphetamine (METH) Abuser After Protracted Abstinence 3 0 ml/gm Normal Control METH Abuser (1 month detox) METH Abuser (24 months detox) Source: Volkow, ND et al., Journal of Neuroscience 21, 9414-9418, 2001. Because… Their Brains have been Re-Wired by Drug Use Control > MA 4 3 2 1 0 MA > Control 5 4 3 2 1 0 Methamphetamine Cognitive and Memory Effects Frequency of Impairment by Neuropsychological Domain 60 60 % Impaired Controls MA Users 50 50 40 40 30 30 20 20 10 10 0 Attention/ Psychomotor Speed Learning and Memory Working Memory Fluency Inhibition Executive Systems Function 0 Defining Domains: Executive Systems Functioning a.k.a. frontal lobe functioning. Deficits on executive tasks assoc. w/: – Poor judgment. – Lack of insight. – Poor strategy formation. – Impulsivity. – Reduced capacity to determine consequences of actions. Brain Serotonin Transporter Density and Aggression in Abstinent Methamphetamine Abusers* * Sekine, Y, Ouchi, Y, Takei, N, et al. Brain Serotonin Transporter Density and Aggression in Abstinent Methamphetamine Abusers. Arch Gen Psychiatry. 2006;63:90-100. Objective of Study Investigate the status of brain serotonin neurons and their possible relationship with clinical characteristics in currently abstinent methamphetamine abusers. Results 1. • 2. • Serotonin transporter density in global brain regions was significantly lower in methamphetamine abusers Suggests that abuse of methamphetamine leads to a global and severe reduction in the density of human brain serotonin transporters Values of serotonin transporter density in widely distributed brain regions were found to negatively correlate with the duration of methamphetamine use. Suggests that the longer methamphetamine is used, the more severe the decrease in serotonin transporter density. Results (Continued) Magnitude of aggression in methamphetamine abusers increased significantly with decreasing serotonin transporter densities in some brain regions. 3. • Bitofrontal cortex, anterior cingulate, temporal cortex No correlation between a representative measure of serotonin transporter density and the duration of methamphetamine abstinence. Individuals abstinent for > 1 year still had a substantial decrease in serotonin transporter density. 4. • Suggests reductions in the density of the serotonin transporter in the brain could persist long after methamphetamine use ceases. Methamphetamine Use, Self-Reported Violent Crime, and Recidivism Among Offenders in California Who Abuse Substances * Cartier J, Farabee D, Prendergast M. Methamphetamine Use, SelfReported Violent Crime, and Recidivism Among Offenders in California Who Abuse Substances. Journal of Interpersonal Violence. 2006;21:435-445. Objective of Study Examine the associations between methamphetamine (MA) use and three measures of criminal behavior: (a) self-reported violent criminal behavior, (b) return to prison for a violent offense, and (c) return to prison for any reason. Methods Participants – 808 low- to medium-level inmates Clear history of substance abuse Within 12 months of release Half the sample entering an in-prison substance abuse (SA) program and the other half from a neighboring prison that offered no formal SA treatment Matched by age, ethnicity, sex offender status, and commitment offense Methods Continued • Baseline and 12-Month Follow-Up Interviews Modified versions of criminal justice treatment evaluation forms developed by researchers at Texas Christian University Sections on sociodemographic background, family and peer relations, health and psychological status, criminal involvement, indepth drug-use history, and an AIDS-risk assessment Results Those who used MA (81.6%) were significantly more likely than those who did not use MA (53.9%) to have been returned to custody for any reason or to report committing any violent acts in the 30 days prior to follow-up (23.6% vs. 6.8%, respectively) Results Continued After controlling for drug trade involvement, MA use was still significantly predictive of self-reported violent crime and general recidivism Implications of Results • These findings suggest that offenders who use MA may differ significantly from their peers who do not use MA and may require more intensive treatment interventions and parole supervision than other types of offenders who use drugs Methamphetamine Abuse, HIV Infection Causes Changes in Brain Structure Jernigan,T, et al American Jnl of Psychiatry Aug 2005 Methamphetamine abuse and HIV infection cause significant alterations in the size of certain brain structures, and in both cases the changes may be associated with impaired cognitive functions, such as difficulties in learning new information, solving problems, maintaining attention and quickly processing information. Co-occurring methamphetamine abuse and HIV infection appears to result in greater impairment than each condition alone Methamphetamine Abuse, HIV Infection Causes Changes in Brain Structure Jernigan,T, et al American Jnl of Psychiatry Aug 2005 Brain scans to analyze structural volume changes in 103 adults divided among four populations: methamphetamine abusers who were HIV-positive; methamphetamine abusers who were HIV-negative; nonabusers who were HIV-positive; and nonabusers who were HIV-negative. They also assessed the ability to think and reason using a detailed battery of tests that examined speed of information processing, attention/working memory, learning and delayed recall, abstraction/executive functioning, verbal fluency, and motor functioning. Methamphetamine Abuse, HIV Infection Causes Changes in Brain Structure Jernigan,T, et al American Jnl of Psychiatry Aug 2005 Methamphetamine abuse is associated with changes in the the brain’s parietal cortex (which helps people to understand and pay attention to what’s going on around them) and basal ganglia (linked to motor function and motivation). The degree of change in the parietal cortex was associated with worse cognitive function HIV infection is associated with prominent volume losses in the cerebral cortex (involved in higher thought, reasoning, and memory), basal ganglia, and hippocampus (involved in memory and learning Methamphetamine Abuse, HIV Infection Causes Changes in Brain Structure Jernigan,T, et al American Jnl of Psychiatry Aug 2005 “In HIV-infected people, the cognitive impairments are associated with decreased employment and vocational abilities, difficulties with medication management, impaired driving performance, and problems with general activities of daily living, such as managing money,” “The impact of methamphetamine could potentially affect treatment and relapse prevention efforts, as well as things like money management and driving performance.” Methamphetamine Abuse, HIV Infection Causes Changes in Brain Structure Jernigan,T, et al American Jnl of Psychiatry Aug 2005 Younger methamphetamine abusers showed larger effects in some brain regions. Among HIV-infected individuals, the researchers noted a direct association between the severity of the infection and greater loss of brain matter. In methamphetamine abusers who are also HIVpositive, decreased volumes are correlated with increased cognitive impairment in one brain region, the hippocampus. Children Children who live in and around the area of the meth lab become exposed to the drug and its toxic precursors and by-products. 80-90% of children found in homes where there are meth labs test positive for exposure to meth. Some are as young as 19 months old. Children Children can test positive for methamphetamine by: – Having inhaled fumes during the manufacturing process – Coming into direct contact with the drug – Through second-hand smoke Children Hundreds of children are neglected by parents who are meth cooks. Nationally, over 20% of the seized meth labs in 2002 had children present. In Washington State, the counties of Grays Harbor, Spokane, Thurston, and Klickitat all reported that children were found at half the labs seized in 2002. In Lewis County, children were found at 60-70 %, and in Clark-Skamania, 35%. Children In 2002, a total of 142 children were present at lab seizures in Riverside and San Bernardino Counties. Most children reported as being present during a seizure were school age. Children Social workers now accompany law enforcement during lab seizures with children involved. – Parents are often charged with second-degree criminal mistreatment, along with manufacturing charges. – Allowing children to live in a toxic environment where additional risks of explosion and fire are high is considered to be neglect at best to child Children are not small adults! Different diet Growing & developing rapidly Higher metabolic & respiratory rate Developing nervous system Unusual habits (hand-to-mouth behaviors; close to floor, contact with many surfaces, at risk for all poisonings) Biologic & developmental vulnerability Prenatal Meth Exposure Preliminary findings on infants exposed prenatally to methamphetamine (MA) and nonexposed infants suggest… – Prenatal exposure to MA is associated with an increase in SGA (small for gestational size). – Neurobehavioral deficits at birth were identified in NNNS (Neonatal Intensive Care Unit Network Neurobehavioral Scale) neurobehavior, including dose response relationships and acoustical analysis of the infant’s cry. Lester et al 2005 Methamphetamine and Sex: Connection in Heterosexuals Percent Responding "Yes" Q.2: My sexual drive is increased by the use of … 100 90 80 70 60 50 40 30 20 10 0 85.3 70.6 55.3 55.6 43.9 18.120.5 opiates male female 11.1 alcohol cocaine Primary Drug of Abuse meth Percent Responding "Yes" Q.4: My sexual performance is improved by the use of … 100 90 80 70 60 50 40 30 20 10 0 58.8 61.1 19.1 15.9 opiates 32.4 24.4 alcohol male female 18.4 11.1 cocaine Primary Drug of Abuse meth Percent Responding "Yes" Q.6: My sexual pleasure is enhanced by the use of … 100 90 80 70 60 50 40 30 20 10 0 73.5 16.018.2 opiates 38.2 24.4 66.7 44.7 male female 11.1 alcohol cocaine Primary Drug of Abuse meth Percent Responding "Yes" Q.8: My use of … has made me become obsessed with sex and/or made my sex drive abnormally high. 100 90 80 70 60 50 40 30 20 10 0 76.5 55.3 44.4 3.2 6.8 opiates 19.514.7 alcohol male female 11.1 cocaine Primary Drug of Abuse meth Percent Responding "Yes" Q.10: I am more likely to have sex (e.g., intercourse, oral sex, masturbation, etc.) when using … 100 90 80 70 60 50 40 30 20 10 0 79.4 65.8 41.5 61.1 50.0 male female 27.8 7.411.4 opiates alcohol cocaine Primary Drug of Abuse meth Percent Responding "Yes" Q.12: I am more likely to practice “risky” sex under the influence of … (e.g., not use condoms, be less careful about who you choose as a sex partner, etc.) 100 90 80 70 60 50 40 30 20 10 0 48.8 35.3 52.9 55.6 male female 16.7 4.36.8 opiates 57.9 alcohol cocaine Primary Drug of Abuse meth Percent Responding "Yes" Q.13: I have become involved in sex acts that are unusual for me when I am under the influence of … (e.g., marathon masturbation, go to “peep” shows, cross-dress, voyeurism, expose yourself, etc.) 100 90 80 70 60 50 40 30 20 10 0 52.9 52.6 1.1 4.5 12.2 opiates 20.6 alcohol 44.4 male female 16.7 cocaine Primary Drug of Abuse meth Percent Responding "Yes" Q.16: Sexual fantasies or desires have previously “triggered” my use of … 100 90 80 70 60 50 40 30 20 10 0 47.4 26.8 32.4 11.1 5.3 4.5 opiates 41.238.9 alcohol cocaine Primary Drug of Abuse meth male female Percent Responding "Yes" Q.19: My sexual behavior under the influence of … has caused me to feel sexually perverted or abnormal. 100 90 80 70 60 50 40 30 20 10 0 52.9 47.4 33.3 3.22.3 opiates 14.6 5.9 alcohol 11.1 cocaine Primary Drug of Abuse meth male female Female Methamphetamine Users: Social Characteristics and Sexual Risk Behavior Semple SJ, Grant I, Patterson TL Women and Health Vol. 40(3), 2004 Demographics (n=98) Ethnicity – – – – – 44% Caucasian 33% African American 16% Latina 2% Native American 5% Other Education – 96% had less than a college education Marital Status – 54% had never been married Employment – 77% were unemployed Demographics Psychiatric Health Status – 38% reported having a psychiatric diagnosis 53% depression 17% bipolar 14% schizophrenia Patterns of Use – 83% smoked Context of Meth Use – Meth was used primarily with either a friend (95%) or a sexual partner (84%). Social and Legal Problems – 36% reported having a felony conviction. Sexual Partners of Meth-Using Women On average women had 7.8 sexual partners in a two-month period (SD=10.7, range 1-74). 84% had casual partners during the past two months. – 90% of all casual partners were reported to be meth users. 31% had an anonymous partner in the past two months. – 76% of anonymous sex partners were meth users. No spouses or live-in partners were reported to be HIV-positive. Sexual Risk Behavior Participants engaged in an average of 79.2 sex acts over a two-month period. Most sexual activity was unprotected. The average number of unprotected and protected sex acts over the two-month period was 70.3 and 8.8, respectively. In terms of unprotected sex: – 56% of all vaginal sex acts were unprotected – 83% of all anal sex acts were unprotected – 98% of all oral sex acts were unprotected Methamphetamine Use and HIV Risk Behaviors Among Heterosexual Men -- Preliminary Results from Five Northern California Counties, December 2001-November 2003 CS Krawczyk, et al., 2006, The Body (http://www.thebody.com/cdc/straights_meth.html#tab2) Recent Versus Never Meth Use* 100 Recent Meth No Meth Use 90 80 70 60 50 40 30 20 10 0 Female Partner Anal with Female Casual Female Partner Multiple Parters IDU Partner Sex for Drugs or $ Injection-Related HIV Risk Injected in the Past 6 Months: – MA Users: 37.1% – Non-MA Users: 11.1% Of these-– 24% used “dirty” syringes – 30% shared cookers, rinse water, etc. Men-Who-Have-Sex-With-Men "The difference between sex with crystal and sex without it is like the difference between Technicolor and black-and-white," one man told me at Tina's Café in San Francisco. “Once you have sex with crystal, it's hard to imagine having it any other way.” New Yorker Magazine, New York. “Crystal tells your brain to go back and get more, more, more. The logical side of your mind is saying, 'I can't keep doing this,' but you are still on your way to the dealer's house.” New Yorker Magazine, New York. “The more I used it, the more I needed it. At one point, I broke into my own house to try and steal furniture.” New Yorker Magazine, New York. "On the Internet, you can be whoever you want to be. Smoke some crystal, get online, and there is nothing you won't or cannot do." New Yorker Magazine, New York. More about HIV+ Meth-Using MSM The following data is based on a small qualitative study: – Participants snorted meth for 9.4 years – Used to “party,” “to get high,” and “to escape” – Got high and looked for sex partners – Used meth with other MSMs but not with heterosexual meth users. SOURCE: Patterson and Semple (2003) Journal of Urban Health, 80: iii77-iii87. Other Data on Meth-Using MSM The following data is based on a sample of 90 HIV+ meth-using MSM: – 46% identified as “binge” users – Average binge lasted 5.6 days – Binge users reported significantly more social difficulties, sexual risk behaviors, and mental and physical health problems SOURCE: Patterson and Semple (2003) Journal of Urban Health, 80: iii77-iii87. Crystal Methamphetamine Use By Latino Men Newly diagnosed HIV-positive Latino men who have sex with men were almost 9 times more likely to report crystal use than HIV-negative men Crystal use was highest among Latinos (20%) Crystal was associated with a higher prevalence of unprotected anal sex and with newly diagnosed HIV Sex-Related HIV Risk (Odd Ratios of MA Users vs. Non-MA Users) 1.5 Traded Sex for Money/Drugs 2.5 Unprotected Sex w/ Non-Partner 4.8 Unprotected Sex w/ IDU 0 1 2 3 4 5 In Los Angeles County, heroin injectors at low risk; gay male meth users at extreme risk % HIV Positive Drug Abuse Problem or Public Health Problem 70 60 50 40 30 20 10 0 MMT-LAC Her-LAC MethHWD Meth-RC LAC HIV Epi (1999-2004); UCLA/ISAP (1998-2004) Weekend Warriers: How It Works. Sun Mon Tues Wed Thur s Fri $50 - $75 for the weekend (excluding cover charges) Sat Intervention: Prevention and Treatment Approaches Methamphetamine and HIV in MSM: A Time-to-Response Association? 100 90% Percent HIV+ 80 62% 60 41% 40 20 0 26% 8% Probability Sample* Recreational User** Chronic Non Treatment*** Outpatient Psychosoc**** Residential**** * Deren et al., 1998, Molitor et al., 1998; ** Reback et al., in prep, *** Reback, 1997; **** Shoptaw et al., 2002; ****VNRH, unpublished data Substance Abuse Treatment Sex Risks Reduced with Treatment: UARI Past 30 Days 3.5 3 2.5 CBT CM CBT+CM GCBT 2 1.5 1 0.5 2(3)=6.75, p<.01 12 -M os os M 6- ks -W 16 ks -W 12 W ks 8- W ks 4- Ba se l in e 0 Methamphetamine Women’s Issues Craving Adolescents A nx Pa ie ra ty no id Id ea tio n Ps yc ho tic is m Ph ob ic Ho st ili ty 1.40 An xi et y So m O at bs iz es at io si ve n In Co te m rp pu er ls so iv na e lS en si tiv ity De pr es si on Mean BSI Score Behavior Symptom Inventory (BSI) Scores at Baseline 1.60 all significant at p< .001 Female 1.20 Male 1.00 0.80 0.60 0.40 0.20 0.00 Beck Depression Inventory (BDI) Scores at Baseline 20.00 p < .001 18.00 Mean BDI Score 16.00 14.00 12.00 10.00 8.00 6.00 4.00 2.00 0.00 Female Male Self-Reported Reasons for Starting Methamphetamine Use 40% 35% *p< .001 Male 30% Female 25% 20% 15% 10% 5% 0% *to lose weight *to relieve depression Percent Using by Route Route of Methamphetamine Administration 64 70 60 50 40 30 20 24 11 10 0 Route of Administration intranasal (IN) smoke (SM) inject (IDU) Craving by Route % No Craving at baseline 70 60 50 40 30 IN SM IDU 20 10 0 P<.05 Length in Treatment (wks) Treatment Length by Route 10 9 8 7 6 5 4 IN SM IDU 3 2 1 0 P<.05 MA-Free Samples by Route % of MA-free UA (3 wks) 0.7 0.6 0.5 0.4 0.3 IN SM IDU 0.2 0.1 0 P<.05 Hepatitis C by Route % Prevelance 50 45 40 35 30 25 20 15 10 5 0 44 21.05 15 IN (n=38) SM (n=202) IDU (n=72) Total (n=314) 10 P<.05 BSI Psychiatric Symptoms by Route 30 25 20 BL PST TX-End PST 6-Mo PST 12-Mo PST 15 10 5 0 IN SM Positive Symptom Total (PST) IDU P<.05 Adolescent Meth Abuse Treatment Admissions Matrix (Boys) (Girls) – 2002 – 2003 – 2004 Phoenix – 2002 – 2003 – 2004 16% 25% 22% 63% 67% 69% (Boys) 25% 23% 27% 43% 51% 53% Sample Characteristics 305 Adolescents (13-18 years old) Average Age ~ 16yrs old (sd=1.138) Gender: 70.2% Males Ethnicity: 55.3% White & 33.1% Latino Ethnic Identification 60 55.3 Percent 50 40 33.1 30 20 3 1 n ia As O 7.6 10 0 er th k ac Bl te hi o tin La W Ethnicity Drug of Choice: N=305 Methamphetamine Pot Alcohol Methamphetamine & Pot Methamphetamine & Alcohol Pot & Alcohol Cocaine Opiates (Heroin) Other 74 (24.3%) 149 (48.9%) 24 (7.9%) 9 (3%) 6 (2%) 26 (8.5%) 6 (2%) 3 (1%) 8 (2.6%) Drug Use by Gender 90 85.1 80 70 63.7 60 50 36.3 40 30 20 14.9 10 0 Meth Other Males Females Treatment History by Drug Use Total (N=275*) *30 Missing METH (n=85) OTHER (n=190) % Completed % Not Completed 139 (50.5%) 136 (49.5%) 37 (43.5%) 46 (54.1%) 102 (53.7%) 88 (46.3%) Legal Problems Missing Data* Total (n=268) METH OTHER USERS (n=189)* (n=79)* Illegal Behaviors Arrest Probation Juvenile Hall 177 (66.0%) 124 (65.6%) 53 (67.1%) Psychological Distress Missing Data* Depression* Suicidality Attempted Suicide Does not want to live Like to injure yourself Psychopathology* Paranoid Feelings Losing Mind Hearing Voices P<.05 Total % Yes (n=275) OTHER (n=196) 128 (46.5%) 83 (42.6%) (n=79) 45 (57.7%) 72 (26.2%) 48 (24.5%) 24 (30.8%) 87 (31.6%) 53 (27.0%) 34 (43.0%) METH USERS Do meth users stop on their own? Meth use via intranasal or oral routes may D/C meth on their own Oral and intranasal use until a decade ago Meth users take 7-10 years to enter Rx Large majority now smoke or inject. They don’t stop on their own. These users are now entering AOD system. Treatment demand is and will expand. Many meth users show up in primary care and mental health systems Methamphetamine Research Meth vs Cocaine: Do Users Switch ? Meth users: White, Mexican/Central American, Rural, Suburban Coke users: African-American, Caribbean, Urban Each group stigmatizes the other Evidence of “switching” minimal, but no prior experience with major shifts in availability. The cocaine to meth “switch” more likely than the reverse, since meth is less expensive, lasts longer and supplies are easier to establish and maintain. Current Status of Meth Research Brain imaging research is impressive, valuable and quite well developed programs Research on meth and kids in labs needed Research on meth and adolescent treatment needed Treatment research developing slowly – No medications available and moving ahead slowly – Few studies of behavioral treatments Thank you rrawson@mednet.ucla.edu www.uclaisap.org