Super User Class Nursing Documentation Revisions Training
advertisement

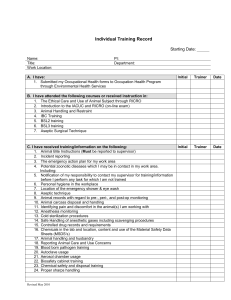
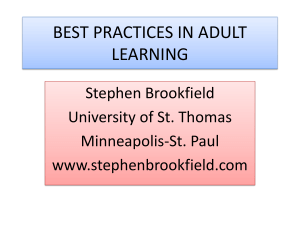
Charting a New Course for Patient Documentation Super User Training Manual Page 1 Document1 Set Up 1. Pull up the Nursing Documentation Super User Power Point 2. Distribute to each terminal: Pt Name Card 3. Flip chart or use Board- write trainer’s names – have markers to record responses 4. Sign In Roster 5. PPT: super user class nursing doc 6. Handout to take back up Copies of Culture change presentation to staff ( for reference – don’t need copy for every) Super User Support Guidelines 7. VIDEO CLIPs ( Not ready 7/18 ) a. what would you do with 20 minutes b. RISK MANAGEMENT 8. Role Play exercises 1-5 9. Handouts: a. Job Aide b. Nursing Documentation Guidelines Policy c. Unit Practice Welcome/Intro/ Vision : (10 minutes) Show slide #1 Introductions Restrooms Length of class is 2 hours Page 2 Document1 What you will learn today Trainer Show slide #2 Thank You Trainer: Show slide #3 The Super User role is vital to implementation of this change. We want to thank you for agreeing to be a super user. Why Chart a New Course Trainer: Show slide #4 This pie chart is the amount of time nurses spend doing various activities from time studies that were conducted. What are we doing the most? Documentation a whopping 35%! Clearly - nurses need more time with their patients & less time writing about what they are doing with their patients Page 3 Document1 These documentation revisions are to re-distribute the pieces of pie Nursing documentation is very important to patient care. Nurses are really telling the story of the patient. So we wanted to be sure we told this story well. Just cutting out fields in HED doesn’t help tell the story better. Documentation is also there to help support other disciplines – providers, RT, PT, Dieticians, SW, etc…. Shifting our thought to value – how we make sure everything that the nurse is documenting is valuable and contributes to that story and informs the care you and others give. Just cutting out time isn't the entire goal – we are putting value back into what nurses document! Every minute is important. Every field should be important! FOCUS Trainer: Show slide #5 The new documentation is being designed for use by proficient, ethical nurses will be challenging old thinking that often resulted in added documentation to address performance issues of very small numbers of low performers. additional documentation burden penalized all nurses often did not achieve the desired outcomes of bringing deficient practice up to standard. old ways of thinking are very ingrained so during this initial communication period, one of our biggest opportunities is “myth busting”. Page 4 Document1 STOP Trainer: Show slide #6 Myth Buster Section (3 minutes) What would you do? Trainer: Show slide #7 ASK …What would you do…..With 10-20 minutes more in your shift? Hopefully you have already discussed this in a staff meeting, (if not your manager will be covering this ) If you had 10-20 minutes time back per shift due to less time spent on documentation, what would you be able to do with your patients and families during that time that you cannot do now? Page 5 Document1 Allow time for response: Users to call out… Impt that they be able to verbalize this to others as they are role modeling this as a super user. WHEN READY….VIDEO CLIP – what would you do with 20 minutes Myth Busters Trainer: Show slide #8 So if we all agree that we want to put value back in our documentation and spend more time with the patient vs writing what hold us back…. Why is it so hard to change. There are some beliefs that are just not correct o If it’s not charted it’s not done o Misconceptions about regulatory requirements o Quality of documentations = quality of my care Transition to this new process will involve changing the culture and some deeply held beliefs and challenging misconceptions. We need you to be the myth busters…. MYTH 1: If it’s not Charted, its not done Trainer: Show slide #9 Fundamental beliefs from nursing school or orientation to our first jobs. Reinforced for so long by so many people and situations that you would have no reason to consider thinking or feeling a different way. We are asking you to be open to new ways of thinking based on evidence and facts and hope you will be willing to think in new ways that will allow you to alter your documentation practices. Page 6 Document1 Risk Management tells us this is just not true! VIDEO CLIP – RISK MGT- NOT READY YET Myth 2: “I have to chart this because it’s required by … “ [Joint Commission, Hospital Policy, Risk Management, etc.] Joint Commission standards require certain outcomes – for example, screening for nutritional risk factors that would warrant a consult to a Dietician BUT they do not mandate what that screening process looks like or specify what must be documented The same is true of many regulatory requirements Generally want us to follow our own policies Our documentation policies are about to change drastically and one big outcome from that will be a reduction in quantity of documentation required HANDOUT OUT DRAFT POLICY: Nursing Guidlines– we’ll review more closely later MYTH 3: “Quantity of documentation = quality of care I provide” If I don’t document a lot it looks like I haven’t worked hard This is not nursing school where you get a better grade the longer your care plan is Changing long-standing, deeply held beliefs is not just about facts. o We also have to understand the emotions and values associated with those beliefs IMPORTANT- We need staff to BELIEVE that changing their documentation is NOT going to negatively impact the quality of care their patients receive. Page 7 Document1 ASK: What other documentation myths should we add to this list? Allow time for responses- - NOTE on FLIP CHART Will result in staffing changes Trainer: Show slide #10 We are reducing documentation in order to increase nurse to patient ratios or make other staffing changes NOT TRUE! No further changes are planned to the staffing models. Documentation reductions are needed to make the model work better. No staff nurse involvement Trainer: Show slide #11 Those making all these changes are out of touch with what really happens at the bedside- these changes will never work. NOT TRUE! Many were involved in developing the revisions! “Real Nurses” were involved Trainer: Show slide #12 Here is a list of the various committee members that have worked on these changes… these are real nurses giving input and making decisions about revisions ASK Are any of you that worked on the revisions here in class today? Allow users to respond. Page 8 Document1 What is NOT changing: Trainer: Show slide #13 Care Organizer & Admin-Rx General format of HED screens and how to select items from drop down menus or typing annotations Nursing Admission History will continue to be documented in StarPanel Clinical Care Classification (CCC) (SABA model) standardized terminology for documentation of problems Required documentation denoted by ALL CAPS Concept of Priority Problems/goals- (but HOW these are documented is being simplified) Patient Scenario Trainer: Show slide #14 Page 9 Document1 The Nit and the Grit of the changes Trainer: Show slide #15 (sign on with own ID, choose HED train, use pt on handout) HANDS-ON (1hr 5 min) Trainer/Learner: Sign on to CWS and Click HED train icon. (minimize the ppt) From Care Organizer, Click HED button Select the patient on your card Page 10 Document1 In the training region you will see both the current tabs as well as the new tabs. The new tabs are in ALL CAPS. Locate these tabs Plan Vitals/I&O Assessment Interventions Devices Education Protocols Page 11 Document1 Old VS New Tab- How to tabs on Nonimplemented units Show slide #17 There will be fewer tabs and they will be re-ordered. The PLAN tab will be the first tab displayed followed by the Vitals I&O tab when we go live… right now in train you still see the Vitals and I&O first. Instead of having various assessment and intervention tabs for different pt care areas, all assessment documentation regardless of pt location will be in the assessment tab. Interventions tabs now separate to make it quicker to go directly to documenting care rendered. New- Devices tab to document information re: devices – ICP, LVAD etc.. Page 12 Document1 Education tab consolidates all education related documentation – including discharge readiness. Are you the type of person that wants to see everything in one place, and doesn’t mind scrolling? Use the new ALL DOC tab where most data from the other tabs are displayed. There will not be tabs specific to clinical areas (AKA med/surg, ICU, Peds). ASSESSMENT TAB Trainer/Learner Click on the Assessment Tab (Show All if collapsed) You may notice: • Decreased Care Categories (menus on left side of HED) • There will be fewer items in the list • Some things have been consolidated- for instance all the IV associated items will be listed under the new “lines” category • Every care category should be addressed upon admission NOTE EXCEPTIONS: • Reproduction assessed on OB, GYN & GU only • Lines only if pt has an IV • CAPS designate required documentation for every shift and change in level of care (not changed). • Data required for approved population based decisions support (Braden PU scale, Glascow coma scale) or to meet current regulatory requirement will be addressed every shift Page 13 Document1 Review of Care Categories Let’s practice documenting for a patient we have just rec’d from the ED as a way of getting familiar with the care categories. Pain Page 14 Document1 Note: Pt was given pain med in Admin-Rx so we are not double documenting that in the assessment or intervention section but will document the pt’s pain score 30-60 minutes following med administration or interventions for pain. We will come back to Reassessment. Neuro Trainer/Learner Click Neurological in the care category list (Show All if collapsed) Trainer/Learner Click NEURO ASSESSMENT Trainer/Learner Hover over Neuro ASSESSMENT to display the normals This neuro assessment will be the place to document the status and if there is a problem. Note the drop down boxes. Page 15 Document1 Note the various categories… You are familiar with WNL and the SABA problems (notice you do not have to click a link to start a priority problem, you start it from this drop down). ASK What do WEL & OEL mean? Look at your Job Aide HANDOUT -Job Aide Page 16 Document1 PROBLEMS Abnormal finding rise to the level of being actual problems if: it is a problem for the patient/family the problem is one of the primary reasons the patient is hospitalized and will be a primary focus for care provided Page 17 Document1 the patient is at high risk to develop a serious complication NEURO Trainer/Learner Click WNL because pt is alert and oriented X3 w/o neuro issues. ASK Notice NEURO ASSESSMENT is in all caps. What does that mean? (Response – must be documented on every shift) Cardiac Trainer/Learner Click CARDIAC ASSESSMENT Trainer/Learner Hover over CARDIAC ASSESSMENT to display the normals. The “hover over” information has been greatly enhanced with the documentation revisions. Instead of documenting standards or “normals” reference the hover overs for that information. In this example when hovering over cardiac assessment, you can see what WNL means and thus eliminate the need to document all the normal values if the pt has no problems. You note the pt is in afib w/o symptoms. The pt reports that they stay in a fib and this is considered their norm. What would you document? Trainer/Learner Click WEL since this is the pt’s norm. Trainer/Learner annotate”A fib X5 years w/o symptoms per pt” Since this the first time assessing this. If pt were on telemetry or a monitor, we would also document under EKG rhythm- A Fib. Page 18 Document1 Vascular/ perfusions Trainer/Learner Click Vascular / perfusion assessment and denote it as WNL. ASK “This care category is not in all caps. What does that mean?” (Response- must be documented upon admission and if abnormal must be charted every shift or as condition changes – but if WNL/WEL doesn’t need to be charted every shift. RESP Trainer/Learner Click RESP ASSESSMENT Trainer/Learner Click Gas exchange alteration Document Wheezes present in BLL cough w productive secretions- thick yellow sputum ASK: what do you chart in R & L Upper Lobes? Nothing, they are normal. GI Trainer/Learner: Click GI ASSESSMENT Trainer /learner document: Pt has hypoactive Bowel Sounds but otherwise no GI issues. ASK “What would you select?” Response: OEL (outside expected limits)– why- because that isn’t normal but it hasn’t risen to status of being a problem but will need to be reassessed to assure it doesn’t develop into a problem. Page 19 Document1 Trainer/Learner Click OEL, then under bowel sounds field, select “hypoactive” SKIN Let’s skip down to skin. In a real admission you will document in each care category. Trainer /learner document pt has stage 1 PU on L buttock, select in the skin assessment category, Choose Pressure Ulcer Trainer/Learner document Start a wound for the PU (there is no change in this process) Braden hasn’t changed, it must be documented on each shift. If the pt is at risk, it will automatically display in red. FALLS RISK/SAFEY o This is required every shift for VCH. o VUH : Fall/Safety Assessment & fall risk status every shift. Morse scale on admission, transfer, or after fall event. LINES Trainer/Learner: Open lines, Note that all lines are listed here. Starting a line hasn’t changed otherwise. We won’t take time to document the IV here. In real life you would document on each care category upon admission. SAVE Trainer/Learner Click Save (BUT DON’T CONFIRM YET) From the Save and Confirm screen, review the list of problems that were identified during the assessment. Trainer/Learner Identify the top 2-3 priority problems by clicking on the !! . This will denote these problems in RED text on all screens. Page 20 Document1 Remember that there are shades of gray to selecting problems and their priorities. Intent is to tell the pt story. Trainer/Learner Identify Save and confirm REASSESSMENT Trainer/Learner: Click on Reassessment (look at handout) After the initial assessment, reassessments are continually done by the nurse. The practice of re-assessing your patient is NOT changing but when that re-assessment must be documented is changing. Re-assessments are documented as warranted based on orders and or patient condition and per unit standards Timeframes: • ICU – at least two more times during the shift • Acute Care – Document re-assessment if patient condition changes. Documenting Response to care at the end of your shift will summarize any changes in your patient otherwise. Review the care categories thar are prority problems, problems and OEL to see if there are changes. If the patient is stable in some or all categories only document “unchanged”. If there are changes document “unchanged except”and then denote only the changes. Remember we want the differences to stand out so don’t document those items that have not changed. Pain must be documented with each re-assessment only if the patient was experiencing pain > than pain goal they had set. Remember to document pain score after administering pain med. Page 21 Document1 Trainer/Learner Document Unchanged except and denote that pt now has nausea- mild. ASK? “What do you have to document on Admission?” All care categories EXCEPTIONS: document reproductive on ob/gyn/gu pts only and lines only if pt has iv lines. “What do you document on every shift? “ Care categories in ALL CAP Braden, Rass etc. Other categories if there are problems or OEL When do you document the reassessment section? • ICU – at least two more times during the shift following the initial shift assessment • Acute Care – Document re-assessment if patient condition changes. Documenting Response to care at the end of your shift will summarize any changes in your patient otherwise. Trainer/Learner Click Save & confirm Add a problem later in the shift: During reassessment, you now determine an area to be a problem you can click on the reassessed value to modify it by click on the exclamation point. Page 22 Document1 It will now show up in the Plan section. You can click on either, the category OEL or the finding and modify it by clicking on the exclamantion point. Education You have collected the patient’s care contact information as well as oriented the pt and their family to the VUMC and unit. Document this information in the Education tab. Trainer/Learner click EDUCATION tab. (Show All if needed) Trainer/Learner Enter Care contact information – be creative and make up some data Trainer/Learner Click the Education section. Scroll to notice discharge at the top, then generic educational info – then disease specific (corresponds to KRAMES categories) Click Pulmonary and select Conditions. Annotate Pneumonia Click on Links and open Krames (under misc), type pneumonia to locate education. In real life we would print this document to give to the pt. Page 23 Document1 ASK Where would you document this handout? Handout (annonate) – the handout name Trainer/Learner In Handouts type: What is Pneumonia (name of handout) About the Education Tab Patient & Family education is an ongoing process and part of our care standards. Documentation is focused on the outcomes of education, rather than the individual components of a teaching session. So be sure to document patient/ care contact response to educational sessions. Per input from nurses, instead of documenting learner, challenges and engagement for each topic, now documented once for each educational session Educational categories and dropdowns, mirror Krames. Denote in Handouts names of documents or educational “bundles” or Krames # Free text field - If other material is used or to denote additional information there is Trainer /Learner : save and confim PLAN The plan of care reflects prioritized problems, interventions, significant care team communications, plan changes, goals, patient response to care and discharge readiness. Tab name changed from CARE PLAN to PLAN. “E-docs pathway will no longer be denoted in HED – should only be saved in StarPanel if it is actually being used as the basis for the plan.” Trainer/Learner click PLAN tab. ( Show All if needed) Trainer/Learner Click Notification (Show All if collapsed) This will be the first item in many tabs. Staff asked for free text boxes instead of having a format – there is a 240 character limit but if need more space just use one of the other communication Page 24 Document1 boxes. Denote who was notified and why as well as actions taken. (EXAMPLE: Dr Patel notified of inadequate pain relief w/ po meds and orders changed to PCA w/ bolus) Instead of clicking “starting priority problem “ in the Care Plan Tab with the revisions, all problems identifiedin the assessment, will automatically display in the Plan tab. If identified as priority problem during the assessment, the priorities problems will be RED. If a problem needs to be noted as a priority after the initial assessment has been completed and confirmed, you can click on the problem and modify to add the !! later. Goals are set at the beginning of your shift for Priority Problems Instead of having to structure goals on your own, many goals have been predefined for each category ( you may notice these are not as specific and detailed ) This makes it quicker & easier to select measureable goals. You may still customize a goal if the “pre-fabbed” goals don’t fit for your patient. Goal attainment is assessed at the end of the shift in Response to Care instead of a Nursing summary and Plan and Priorities. o Toward the end of the shift, just as before, assess progress toward goals and recommendations for the on coming shift. Instead of documenting the phase of the care plan, a nursing summary and plan and priorities, document a single summary note in the Response to Care/Recommendation area. (will document this in a moment) There is a 240 character limit- If this is not sufficient space, use one or more of the adjacent “Communication/ event” note to supplement. Don’t get carried away-this narrative should be short and to the point. Trainer/Learner click - PLAN tab. (Show All if needed) Page 25 Document1 ON YOUR OWN: select goals for each of the priority problems (trainer document : pain goal of 3, Pulmonary- Exhibit improved lung sounds, Self report ability to breath comfortably) Trainer /Learner : save and confim (There is an interventions section under Plan but go to the Interventions tab to do this!) Reinforce: How Do I Select The Right Priority Problem(s)? o Choose what is most important for your patient (i.e. pain control) and that you as a nurse can impact. o The goal is to communicate the plan and achieve good outcomes o If you can support it with your nursing judgment and documentation, there are no wrong choices. Reinforce: Problems are identified through ongoing assessment of the patients physiological, functional, and psychosocial state Priority problems are the 1-2 (no more than 3) issues of care that will be the focus during the shift Don’t forget to include the patient in problem identification and goal setting Explicit goals are set early for 1-2 high priority problems to help focus and adjust the plan for care throughout the shift Goals should reflect outcomes that can be achieved through nursing care (independent or collaborative) INTERVENTIONS New Interventions tab – no longer embedded in assessment category Organized by care categories Easier to find! Trainer/Learner click INTERVENTIONS Page 26 Document1 Document that the pt performed Incentive Spirometry & DB Trainer/Learner Skin interventions Trainer/Learner click Pressure Ulcer care and select PU stage 1 care was performed Specific details of care not spelled out, reference hover overs, Links or Mosby for specifics. In HED just document the care (see below example of skin breakdown control. In this example, note that Skin Breakdown Control is denoted by the PU stage. Utilize Links to display details of the various interventions associated with each PU stage. Links content has been re-organized to mirror the care categories. Hover over feature may also give additional information. Trainer demonstrate accessing the skin care resources in links Page 27 Document1 Trainer/Learner : Save and confirm DEVICES New “Devices” tab added to aid in quickly documenting all devices Previously, these were embedded in the assessment/intervention sections Many of these items are cardiac related Trainer/Learner; click Devices tab Review items in this category – nothing to document for this pt scenario Page 28 Document1 PROTOCOLS TAB RESPONSE TO CARE/RECOMOMENDATIONS Toward the end of the shift, a summary statement should be made re: the pts response to the care provided their progress toward goals and any recommendations for the upcoming shift. In the old system this was in the nursing summary and plan/priorities fields. There is just one field now - response to care/recommendations in the PLAN tab. The response to care is a short statement that communicates outcomes of care to the team: Were goals of care achieved? Did problems improve or worsen. Did new problem arise? What adjustments to the plan were made. How did the patient tolerate interventions Do not repeat numeric values captured elsewhere (i.e. VS, lab values, etc.) unless to describe whether a priority goal was met Page 29 Document1 Trainer/Learner: Click PLAN tab, click Plan of Care, Show All Trainer/Learner: Click response to care type “Wheeze decreased bil w/ DB & cough, reports less pain and decreasd shortness of breath, cont. to wean o2 , enc IS Q 2h w/a . Draw Vanc level at 1800.” Save and Confirm ASK: Do you see how this replaces the nursing summary, plan and priorities? Note that we are not explictly denoting goal is met or not. Transition, Policy and Super User Expections ( 25 Min) Transitioning As you can see these are some major changes. So what is the plan to get all the staff trained and the units implemented? We will have to use a phased approach to implement these changes over several weeks. As these changes are made, unlike previous changes, charting from old tabs won’t display on new tabs and vice versa. Since our patients move between units, we must be prepared to live in both worlds for a little while. ALL DOCS Trainer/Learner click ALL DOC tab(click Show All) The New All Docs tab, displays most of the data documented on any of the new tabs in one single view – expect to scroll Page 30 Document1 o All Docs is preferred view when a patient is transferred from an implemented unit to a non-implemented unit To view additional results, click on the item and select “Show All Values” Several weeks between when the pilot units (8N, 8S and 8VCH) implement the revisions and other units implementation The new tabs will NOT display for the non implemented units On the implemented unit the old tabs will not display You can still view the tabs though: To view documentation on old tabs: Trainer/Learner 1) Click Chart in the top tool bar and select the item to display. The most of the new tabs are in ALL CAPS. 2) Select the desired tab to display Notice that if you do not open a charting session, the data will display in a collapsed view (i.e. hourly display) click chart and the data expands and each column will represent the actual time data was documented i.e. each column will represent a documentation session). SUPER USER PREP ASK: What did you find confusing or new? Allow time for responses. Nursing Documentation Policy Review Trainer: Show slide #22 Handout- Nursing Documentation Guidelines- BUT TAKE BACK UP!!! Page 31 Document1 Up to this point we have been covering the content that staff will be getting in the LMS Modules As “Super Users” you will need additional information Take a few minutes to REVIEW THE DOCUMENTATION Guidelines. Emphasize that it is in draft form and evolving Trainer: Allow learners time to read and tell them it is available on the SSS Website Tips Trainer: Show slide #23 Page 32 Document1 Discharges Trainer: Show slide #24 Discharge Plan of Care Reviewed, Discharge Readiness and Discharge Problems needing follow-up have been moved from the Assessment/Problem section to the Plan of Care section on the PLAN Tab. The discharge plan of care must be reviewed q 24/ unit policy Discharge readiness is in ALL CAPS so it must be documented every shift. Upon Discharge : o A current shift assessment should be completed prior to discharge, problems needing follow-up should be identified and documented with a plan to address… o Will there be f/u with Home health, outpt clinic or just what for those un met goals o Discharge Problems needing followup will be addressed when the pt is discharged – for example if they are not independent with theirvs dressing change an Home Health is to continue education and support Post mortum care- documented under the psychosocial interventions, terminal care section. Page 33 Document1 When to Document What – A word about timing Trainer: Show slide #25 HANDOUT JOB AID: Documentation Guidelines : A summary of when to document what Review this Job aid, this pulls all the pieces together re: when to document what. ASK: what questions do you have? Does this help? Make Sense? Display of Data Trainer: Show slide #26 Currently, most of the documentation is displayed in a real time view. Some spend a lot of time adjusting times they document to be at the top of the hour so the data aligns in a single column, making viewing info easier. With the revisions, the displays of the data have been collapsed to facilitate easy viewing. Learner: Open up HED and click on the assessment tab, get a sense of what I mean. Data displays in 1 hour increments VS/I&O Assessment Interventions Pain/CDR Device Protocols Learner: click on the Plan tan and get a sense of what I mean. Page 34 Document1 Displays in 12h increments Plan ALL DOCS Displays in 24h increments Education REMEMBER: hover over the category and click on Show All if you want to view all the results for that item. Shift to Shift Handovers Trainer: Show slide #27 Use the Plan tab to facilitate handovers. It should capture the patient story. SUPPORT 22 Min Training and Implementation Trainer: Show slide 28 Training Manager presentation to staff re: culture change PASS AROUND THE HANDOUT PPT THAT MANGERS DO PRIOR TO GO LIVE. (take back up, we can email the customized version if they want it) Page 35 Document1 Transitioning from Old to New Trainer: Show slide #29 GO LIVE DAY Tech team will push the new tabs to HED “LIVE” by 0700 Day shift will begin using the new tabs To view previous charting, toggle back to the “old tabs” from the tabs drop down menu or via the chart option in the top tool bar Page 36 Document1 Roles and Responsibilies Trainer: Show slide #30 Resources Trainer: Show slide #31 Having troubles… Know when you need to get help! Page 37 Document1 Trainer: Show slide #32 On Line Resources Trainer: Show slide #33 Learners: ½ practice getting to Pegasus ½ pull up SSS Nursing Education web site. Ask How did you get to it? Numerous ways Promoting Adoption Trainer: Show slide #34 Page 38 Document1 Timing Is Everything Trainer: Show slide #35 Page 39 Document1 Approach Trainer: Show slide #36 Approach Cont Trainer: Show slide #37 Page 40 Document1 Follow Up Trainer: Show slide #38 Slide 39 Page 41 Document1 Difficult People (SKIP ROLE PLAYS IF RUNNING SHORT ON TIME) Trainer: Show slide #40 ASK IS this you or the user you are helping… Being a super user is NOT easy and you will encounter difficult people. Let’s spend a few minutes practicing how to handle these situations. Role Play Activity ( takes at least 10 mins) Trainer: pass out 5 role play exercises and assign groups. Instructions: Take the next 5 minutes in your group to brain storm about these scenarios and then be prepared to share. If you want to act out – GREAT! Allow groups 5 minutes to work then 1 minute report Learners are asked… What is the Best Way to handle the situation? What is the Worst Way to handle the situation? Act out examples of both… be creative. Role Play #1 You are doing support on a unit & a staff member become very hostile & argumentative. This is occurring at the nurses station with others around including pts & families KEY: Make sure they include: • De-escalation • Involve unit mgt. team • Take the discussion to a more private area • Other? Role Play #2 You are doing support on a unit & everyone working reports they do not need help. You reviewsome work & observe that one particular person is struggling and making many mistakes Key: Make sure they include: • Avoid embarrassing struggler Page 42 Document1 • Show data of what is wrong • Other? Role Play #3 You are doing support on a unit & in report you have been told that Nancy Nurse has not received help from Super User/SSS yet. Every time she was asked earlier she was “too busy” & that she always seems to be busy. Support is ending soon & your task is to assess how Nancy is doing & impose some assistance. Key: Make sure they include: • Consultation w/CSL to verify “business” legit • In assertive (but NOT aggressive) manner, impress up on the resister that this is NOT going away and that you really want to help them be successful in the very short amount of time allocated to support • Other? Role Play #4 You are doing support on a unit on the “go live day”. It has been horribly busy. One nurse that you are attempting to help is practically in tears she is so frustrated. This is a very experienced nurse that is well respected by her peers but really struggles with computers. Key: Make sure they include: • “Taking care of pt. MOST important” • Focus on not more than 3 key messages to address highest priority concerns • Document concerns. We have got to make this work for this nurse or no one else will trust it. • Other? Role Play #5 You are doing support on a unit on the “go live day”. It has been horribly busy. All the staff are complaining that they system is unsafe & they can’t believe that you are making them use it. One nurse absolutely refuses to use the system. From your perspective the system is generating a lot of errors and response time is extremely slow. You are very frustrated as well. Key: Make sure they include: • Fall back if features really not working is to use downtime procedures for that specific issue • Make sure to report system issues • Consult with SSS partner • Other? Page 43 Document1 Strategies Trainer: Show slide #41 Let’s summarize what you learned… What are some dos and don’t’s Be comforting not confrontational. I know it’s hard and it take more time right now. I understand your frustration. ASK: What else??? WRITE ON BOARD OR FLIP CHART Discuss. Page 44 Document1 REPEAT AFTER ME… Trainer: Show slide #43 HAPPY USERS HAPPY SUPER USERS- OUR GOAL Trainer: Show slide #44 ASK What can you think of that would help support you during this transition? WRITE ON BOARD OR FLIP CHART Page 45 Document1 Next Steps Trainer: Show slide #45 After Class Responsibilities Communicate to Nicole & Karen any issues/ comments from users. Denote names and units if specific f/u needed Report to CAPS any issues that are specific to a unit Collect all the items that were passed out but need to be taken back up o Copies of the Culture Change presentation by managers (YELLOW SHEETS) Place in trainer manual o Role Plays (Laminiated Sheets) Place in trainer manual o Pt name card (return to drawers) Return rosters to Julie and denote which learners were not present Report to Julie if we are running low on handouts or supplies Assure that LCD is turned off Page 46 Document1