Unit One: Introduction to Physiology: The Cell and
advertisement

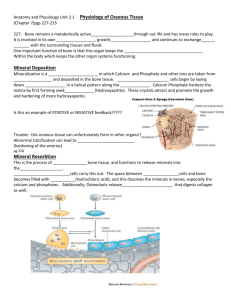
Chapter 79: PTH, Calcitonin, Calcium and Phosphate Metabolism, Vitamin D, Bone, and Teeth Guyton and Hall, Textbook of Medical Physiology, 12 edition Overview of Ca and P Regulation in ECF and Plasma • Calcium in the Plasma and Interstitial Fluid a. About 41% of the calcium is combined with the plasma proteins and is non-diffusible through the capillary membrane b. About 9% of the calcium is diffusible but combined with anionic substances c. Remaining 50% is both diffusible and ionized Overview of Ca and P Regulation in ECF and Plasma • Inorganic Phosphage in the ECF a. Exists in two forms HPO4 (1.05 mmol/L) and H2PO4 (0.26 mmol/L) b. Increase in ECF phosphate and the two forms increase proportionately c. If pH becomes more acidic, H2PO4 increases and HPO4 decreases Overview of Ca and P Regulation in ECF and Plasma Fig. 79.1 Distribution of the three forms of calcium Overview of Ca and P Regulation in ECF and Plasma • Non-bone Physiologic Effects of Altered Calcium and Phosphate Concentrations in the Body Fluids a. Hypocalcemia causes nervous system excitement and tetany b. Hypercalcemia depresses nervous system and muscle activity Overview of Ca and P Regulation in ECF and Plasma • Absorption and Excretion of Ca and P Fig. 79.3 Overview of calcium exchange between different tissue compartments of a person ingesting 1000 mg calcium per day Bone and Its Relation to Extracellular Ca and P • Organic Matrix of Bone a. 90-95% collagen fibers b. Rest is a homogeneous ground substance c. Ground substance-composed of ECF, proteoglycans, especially chondroitin sulfate and hyaluronic acid Bone and Its Relation to Extracellular Ca and P • Bone Salts a. Crystalline salts are primarily calcium and phosphate b. Magnesium, sodium, potassium, and carbonate ions are also present c. Calcium salts have great compressible strength and collagen has great tensile strength Bone and Its Relation to Extracellular Ca and P • Precipitation and Absorption of Calcium and Phosphate in Bone-Equilibrium with the ECF a. Mechanism of bone calcification 1) Initial stage in bone production is the secretion of collagen molecules and ground substance by osteoblasts 2) Collagen polymerizes to form collagen fibers and forms the osteoid substance 3) Calcium salts ppt into the osteoid and eventually the osteoid traps the osteoblasts which then are referred to as osteocytes Bone and Its Relation to Extracellular Ca and P 4) After a few days the ppt calcium forms hydroxyappetite crystals b. Calcium exchange between bone and ECF-calcium is in equlibrium between bone and ECF; provides a rapid buffering system to keep the calcium ion concentration in the ECFs from rising to excessive levels or falling to low levels under transient conditions of excess or decreased availability of calcium Bone and Its Relation to Extracellular Ca and P • Deposition and Absorption of Bone-Remodeling a. Bone is continually being deposited by osteoblasts and being absorbed by osteoclasts; osteoclasts are found in bone cavities and on the outer surfaces b. Absorption of bone-the function of osteoclasts; release proteolytic enzymes and organic acids c. PTH stimulates osteoclast activity and bone resorption Bone and Its Relation to Extracellular Ca and P • Deposition and Absorption of Bone-Remodeling d. Bone deposition and absorption are normally in equilibrium (except in growing bones where deposition exceeds absorption) e. Value of continual bone remodeling-bone adjusts in strength in proportion to the degree of bone stess; replacement of old bone with new bone keeps the bones tough but not brittle; allows for the proper support of mechanical forces by deposition and absorption in accordance with growth patterns Bone and Its Relation to Extracellular Ca and P • Deposition and Absorption of Bone-Remodeling f. Repair of a fracture activate osteoblasts-in a fracture osteobalsts are formed from osteoprogenitor cells; fracture maximally activates peristeal and intraosseus osteoblasts involved in the break; eventual formation of the callus (bony ridge surrounding the break) Bone and Its Relation to Extracellular Ca and P Fig. 79.4 Osteoblastic and osteoclastic activity in the same bone Bone and Its Relation to Extracellular Ca and P Fig. 79.5 Bone resorption by osteoclasts Bone and Its Relation to Extracellular Ca and P Fig. 79.6 Structure of bone Vitamin D • Cholecalciferol (Vitamin D3) is Formed in the Skinas a result of irradiation of 7-dehydrocholesterol, a substance normally in the skin, by uv light rays from the sun • Cholecalciferol is Converted to 25-Hydroxycholecalciferol in the Liver Vitamin D Fig. 79.7 Activation of vitamin D3 to form 1,25-dihydroxycholecalciferol and the role of vitamin D in controlling the plasma calcium concentration Vitamin D Fig. 79.8 Effect of increasing vitamin D3 intake on the plasma concentration of 25-hydroxycholecalciferol. Vitamin D Fig. 79.9 Effect of plasma calcium concentration on plasma concentration of 1,25-Dihydroxycholecalciferol Vitamin D • Formation of 1,25-Dihydroxycholecalciferol in the Kidneys and Its Control by PTH • Calcium Ion Concentration Controls the Formation of 1,25-Dihydroxycholecalciferol • Actions of Vitamin D a. Vitamin D receptors are present in most cells of the body and are located in the nuclei of the target cells. Vitamin D • Actions of Vitamin D b. Vitamin D has a “hormonal” effect promoting intestinal calcium absorption c. Promotes phosphate absorption by the intestines d. Decreases renal calcium and phosphate excretion e. Extreme quantities cause absorption of bone f. Small quantities promote bone calcification Parathyroid Hormone (PTH) •Physiologic Anatomy of the Parathyroid Glands a. Normally there are four glands located immediately behind the thyroid gland b. Removal of two of the glands generally causes no major physiologic abnormalities (removal of the third causes a transient hypoparathyroidism) Parathyroid Hormone (PTH) • Physiologic Anatomy of the Parathyroid Glands Fig. 79.10 The four parathyroid glands lie immediately behind the thyroid gland. Parathyroid Hormone (PTH) • Chemistry of Parathyroid Hormone a. First is a preprohormone, the prohormone, and finally the active hormone; MW 9500 b. PTH increases calcium and phosphate absorption from the bone and decreases calcium excretion by the kidneys Parathyroid Hormone (PTH) • Chemistry of Parathyroid Hormone Fig. 79.11 Approximate changes in calcium and phosphate concentrations during the first 5 hours of PTH infusion at a moderate rate Parathyroid Hormone (PTH) • Osteolysis-Rapid Phase of Ca and P Absorption From Bone a. In the presence of large quantities of PTH, removal of bone salts occurs from two areas (1) from the bone matrix in the vicinity of the osteocytes, and (2) near the osteoblasts along the bone surface • Activation of the Osteoclasts-Slow Phase of Bone Absorption and Calcium Phosphate Release a. Occurs in two phases (1) immediate activation of the osteoclasts already formed and Parathyroid Hormone (PTH) (2) formation of new osteoclasts b. Several days of excess PTH usually cause the osteoclastic system to become well developed, but can continue to growth for months under the strong stimulus of PTH c. After a few months, osteoclastic resorption can lead to weakened bones and a secondary stimulation of osteoblasts to correct the condition Parathyroid Hormone (PTH) • PTH Decreases Calcium Excretion and Increases Phosphate Excretion by the Kidneys a. Causes rapid loss of phosphate due to a decrease in proximal tubular reabsorption b. Increases the renal absorption of calcium, magnesium, and hydrogen c. Decreases the absorption of sodium and amino acids d. PTH is necessary otherwise there would be a continual loss of calcium from the ECF and bones Parathyroid Hormone (PTH) • PTH Increases the Intestinal Absorption of Ca and P a. Cyclic AMP mediates the effects of PTH b. Slightest decrease in calcium concentration in ECF causes the parathyroid gland to increase the rate of secretion within minutes c. If decreased calcium concentration continues, the parathyroid glands will hypertrophy (i.e. ricketts, during pregnancy, and lactation) Parathyroid Hormone (PTH) Fig. 79.12 Approximate effect of plasma calcium concentration on the plasma concentrations of PTH and calcitonin Parathyroid Hormone (PTH) Fig. 79.13 Summary of the effects of PTH on bone, the kidneys, and the intestine in response to decreased extracellular fluid calcium ion concentration Calcitonin • Increased Plasma Calcium Concentration Stimulates Calcitonin Secretion a. Synthesis and secretion of calcitonin occur in the parafollicular or C cells of the thyroid gland b. Calcitonin is a 32 amino acid peptide with a MW 3400 Calcitonin • Calcitonin Decreases Plasma Calcium Levels a. The immediate effect is to decrease the absorptive activities of the osteoclasts b. The second and more prolonged effect is to decrease the formation of new osteoclasts c. Calcitonin has only minor effects on calcium handling in the kidney tubules d. Calcitonin has a weak effect on plasma Ca levels in the adult human Summary of Control of Ca Ion Concentration • The First Line of Defense: Buffer Function of the Exchangeable Calcium in Bones • The Second Line of Defense: Hormonal Control of Calcium Ion Concentration Pathophysiology of PTH, Vitamin D, and Bone Disease • Hypoparathyroidism • Primary Hyperparathyroidism • Secondary Hyperparathyroidism • Ricketts • Osteoporosis Physiology of the Teeth • Functions of Different Parts of the Teeth Fig. 79.14 Functional parts of a tooth Physiology of the Teeth • Functions of Different Parts of the Teeth a. Enamel-covers the outer surface of the crown of the tooth; once the tooth has erupted no more enamel is formed; extremely hard b. Dentin-main body of the tooth and is composed of hydroxyapatite crystals embedded in collagen fibers; deposited and nourished by a layer of cells called odontoblasts Physiology of the Teeth • Functions of Different Parts of the Teeth c. Cementum-bony substance secreted by cells of the periodontal membrane which lines the tooth socket; collagen fibers and cementum hold the tooth in place; increases in thickness and strength with age d. Pulp-fills the pulp cavity and is composed of connective tissue with nerve fibers, blood vessels, and lymphatics Physiology of the Teeth • Dentition a. Two sets of teeth: the deciduous or milk teeth and the permanent teeth b. Deciduous-erupt between the 7th month and the second year of life, and last until the 6th to the 13th year of life; 20 in number c. Permanent-replaces each deciduous tooth and an additional 8-12 molars appear posteriorly for a total of 28-32 Physiology of the Teeth • Formation of the Teeth Fig. 79.15 A: Primordial tooth organ B: Developing tooth C: Erupting tooth Physiology of the Teeth • Metabolic Factors Influence the Development of the Teeth a. Rate of development and speed of eruption can be accelerated by both thyroid and growth hormones b. Deposition of salts is affected by the amount of calcium and phosphate in the diet, the amount of vitamin D, and the rate of PTH secretion Physiology of the Teeth • Metabolic Factors Influence the Development of the Teeth a. Rate of development and speed of eruption can be accelerated by both thyroid and growth hormones b. Deposition of salts is affected by the amount of calcium and phosphate in the diet, the amount of vitamin D, and the rate of PTH secretion c. Mineral exchange-new salts replace old salts, similar to what occurs in bone Physiology of the Teeth • Dental Abnormalities a. Caries-result from the action of bacteria on teeth (most common Streptococcus mutans); begins with the formation of plaque; fluoride makes the teeth 3x more resistant to caries as teeth without fluoride b. Malocclusion-usually caused by hereditary abnormality; the teeth do not interdigitate properly and therefore cannot perform their normal grinding or cutting action.