Single Payer Economics:
Making Sense of Health Care
Finance
Leonard Rodberg, PhD
Urban Studies Dept., Queens College/CUNY
and
NY Metro Chapter, Physicians for a National
Health Program
1
High Cost of Health Insurance
Premiums: Even the Middle
Class Can No Longer Afford It
National Average for Employer-provided Insurance:
Single Coverage
Family Coverage
$ 4,704 per year
$12,680 per year
Median household income = $50,233
Source: Kaiser Family Foundation/HRET Survey of Employee Benefits, 2008;
U.S. Census Bureau, 2008
2
Private Insurers’ High Overhead
30%
26.5%
19.9%
20%
16.3%
10%
3.1%
0%
Medicare
Non-Profit Blues
Commercial
Carriers
International Journal of Health Services 2005; 35(1): 64-90
Investor-Owned
Blues
3
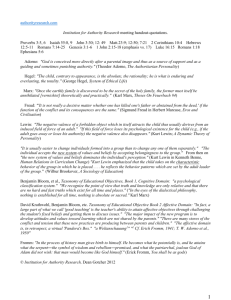
Billing and Insurance: Nearly 30% of
All Health Care Spending
Allocation of Spending for Hospital and Physician Care
Paid through Private Insurers
Other Insurer Costs
and Profit
11%
Insurer Billing
8%
Hospital Billing
4%
Medical Care
64%
Physician Billing
5%
Medical Care
Administration
9%
Source: James G. Kahn et al, The Cost of Health Insurance Administration in California:
Estimates for Insurers, Physicians, and Hospitals, Health Affairs, 2005
4
The Mandate Model
Obama/Ted Kennedy/Jacob Hacker
•
•
•
•
The problem : Too many uninsured
The solution: Everyone should buy insurance
Employers should contribute or offer insurance
Continued reliance on private insurance, with
the option of a public plan
• “Keep what you have”
• No regulation of insurance company premiums
or reimbursement and denial practices
5
The Mandate Model Won’t Work
• Won’t lead to 100% coverage
• Private health insurance will be a continuing
consumers nightmare (copay, deductible, denials)
• Doesn’t address widespread underinsurance
• Increases cost of the system by billions of dollars
• Many payers remain, so the savings from a single
funding source can’t be achieved.
• There is no way to control costs as long as there
are many separate plans.
It treats the symptom – the uninsured –
while ignoring the disease – private insurance.
6
A FALSE POLICY CHOICE
Assertion: “Let’s first cover everybody.
Then we can deal with the system’s
inefficiencies.”
Fact: We will never have enough money to
provide everyone with decent coverage
until we eliminate the principal sources of
waste and inadequate coverage.
7
Conyers/Kucinich/et al
Expanded and Improved Medicare for All
“single payer national health insurance”
HR 676
• Automatic enrollment - everyone receives
a card assuring payment for all needed care
• Doctors and hospitals remain independent,
negotiate fees, budgets with public agency
• Public agency processes and pays bills
• Financed through progressive taxes
8
How We Pay for Health Care
Today
Federal
Government
(existing
Medicare,
Medicaid, other)
Private
Insurance
Out-of-pocket
State and Local
Govt (existing
Medicaid, other)
Source: Health Affairs, Feb. 2008; data for 2006
9
How Single Payer Could Be Paid For:
One Example from a Recent Study of a
California Plan
Employer Payroll
Tax (8%)
Employee Payroll
Tax (4%)
Surcharge on income
(1% above $200,000)
Federal
Government
(existing
Medicare,
Medicaid, other)
State and Local
Govt (existing
Medicaid, other)
Business (selfemployed) income tax
(12% )
Investment income tax
(4% )
Note: Payroll and income taxes between $7,000 and $200,000 only.
Source: Health Care for All Californians Act: Cost and Economic Impacts Analysis, The Lewin Group, January 2005
10
Covering Everyone with
No Additional Spending
Additional costs
Covering the uninsured and poorly-insured
Elimination of cost-sharing and co-pays
Total Costs
Savings
Reduced insurance administrative costs
Reduced hospital billing costs
Reduced physician office costs
Bulk purchasing of drugs & equipment
Primary care emphasis & reduce fraud
Total Savings
Net Savings
+6.4%
+5.1%
+11.5%
-5.3%
-1.9%
-3.6%
-2.8%
-2.2%
-15.8%
- 4.3%
Source: Health Care for All Californians Plan, Lewin Group, January 2005
11
Family Spending: Savings for Most
Source: Health Care for All Californians Plan, Lewin Group, January 2005
12
Employer Spending: Savings for Those
Currently Offering, Modest Cost for the Rest
Source: Health Care for All Californians Plan, Lewin Group, January 2005
13
Why Health Care Is On the Agenda:
Escalating Cost
Average Annual Premiums for Single and Family
Coverage, 1999-2008
$2,196
$2,471*
2000
Family Coverage
$6,438*
$2,689*
$7,061*
$3,083*
2002
Single Coverage
$5,791
$8,003*
$3,383*
$9,068*
$3,695*
2004
$9,950*
$4,024*
$10,880*
$4,242*
2006
$11,480*
$4,479*
$12,106*
$4,704*
2008
$0
$2,000
$4,000
$6,000
$12,680*
$8,000
$10,000
$12,000
$14,000
* Estimate is statistically different from estimate for the previous year shown (p<.05).
Source: Kaiser/HRET Survey of Employer-Sponsored Health Benefits, 1999-2008.
14
The Growth in Cost Must be Addressed
if Any Plan is to Succeed
Single payer offers real tools to contain costs –
• Budgeting, especially for hospitals
• Investment planning
• Emphasis on primary care and coordination of care
Mandate plans offer only hopes –
• Computerization
• Chronic disease management
• Insurance company competition
There is no data or experience to suggest that
these will cut costs or limit the rise in cost.
15
Studies of Single Payer Plans
Government Accounting Office
US
Congressional Budget Office
US
Congressional Budget Office
US
Lewin Group
New Mexico
Lewin Group
Minnesota
Solutions for Progress
Delaware
Lewin Group & Solns for Progress Massachusetts
Lewin Group
Maryland
Lewin Group
US (ANA Proposal)
Lewin Group
Vermont
Lewin Group
California
Solutions for Progress
Rhode Island
Mathematica, Inc.
Maine
Missouri Foundation for Health
Missouri
Lewin Group
Georgia
Kenneth Thorpe, Emory University US
Lewin Group
Colorado
June 1991
December 1991
April, July, Dec 1993
November 1994
February 1995
April 1995
December 1998
June 2000
September 2000
August 2001
April 2002 & January 2005
November 2002
December 2002
October 2003
June 2004
August 2005
August 2007
All reach the same conclusion: Everyone would be insured for
comprehensive care for no more than we are now spending.
16
No Study (Yet) of HR 676!
Blue Ribbon Task Force on Single Payer
Blue
Ribbon
Task
Force
Health Reform – to oversee that study
Rep. John Conyers (D., MI), Honorary Co-Chair
Michael Lighty
Joel Alpert, MD
Dir of Public Policy, California Nurses Assoc
Prof. of Pediatrics, Boston University School of Medicine
Don McCanne, MD
Dean Baker, PhD
Senior Policy Fellow, PNHP
Co-Director, Center for Economic and Policy Research
David McLanahan, MD
Thomas S. Bodenheimer, MD
Rudy Mueller, MD
Professor, Department of Family and Community Medicine, UCSF David L. Rabin, MD, Co-Chair
Olveen Carrasquillo, MD
Rsch Prof of Family Medicine, Georgetown Univ Medical Center
Assoc. Prof. of Med &Health Policy, Columbia Univ Medical Center Edie Rasell, MD, PhD
Chunhuei Chi, PhD
Minister for Workplace Justice, United Church of Christ
Assoc Professor, Dept. of Public Health, Oregon State University
Leonard Rodberg, PhD, Executive Director
Rose Ann DeMoro
Professor and Chair, Urban Studies Department, Queens College
Executive Director, California Nurses Assoc
Gordon Schiff, MD
Oliver Fein, MD
Ctr for Patient Safety Rsch&Practice, Brigham&Women’s Hosp
Prof of Clinical Med and Public Health, Weill Cornell Medical CollegeSteven S. Sharfstein, MD
Harvey Fernbach, MD
Pres and CEO, Sheppard Pratt Health System
Hugh Foy, MD
Paul Sorum, MD PhD
Prof and Dir of Surgical Specialites Clinic, U Wash School of Med
Prof of Internal Medicine and Pediatrics, Albany Medical College
John Geyman, MD
Jaime Torres, MD
Prof Emeritus, Department of Family Medicine, Univ of Washington President, Latinos for Natl Health Insurance
Kevin Grumbach, MD
Walter Tsou, MD
Prof and Chair, Department of Family & Comm Medicine, UCSF
Former Commissioner, Department of Health, Philadelphia
David Himmelstein, MD
Steffie Woolhandler, MD
Cambridge Hospital/Harvard Medical School, Co-founder, PNHP
Cambridge Hospital/Harvard Medical School,Co-founder, PNHP
James G. Kahn, MD
Quentin Young, MD, Co-Chair
Professor of Health Policy, UCSF
Natl Coordinator, PNHP, Past Pres, Amer Public Health Assoc
17
Will We Get Real Health Care Reform
Before the Premium Takes All our Income?
Today
Source: American Family Physician, November 14, 2005
18
 0
0