Organ Donation
What Is the New York Organ
Donor Network (NYODN)?
Organ Procurement Organization (OPO)
Federally-designated
Oversight by Federal Government
58 OPO’s in the United States
OPO’s serve as organ sharing units
Service Area
New York City
(Bronx, Brooklyn, Manhattan, Queens, Staten Island)
Long Island
5 counties in New York State
(Rockland, Putnam, Orange, Westchester & Duchess)
1 county in Pennsylvania (Pike)
13 million persons
> 100 hospitals
The Donor Network is the 2nd largest OPO in the US
What Does NYODN Do?
Receives all calls from hospitals on deaths & potential organ & tissue donors
Evaluates organ & tissue donor potential
For organs, sends nurses to hospitals to evaluate & maintain potential donors
Requests consent for organ & tissue donation
Arranges for recovery of organs & tissue
Determines appropriate organ allocation (UNOS)
Gets organs to appropriate Transplant Centers
Donor Family Services
Community Education / Public Awareness
Hospital and Family Services
Source: New York Organ Donor Network
4 Types of Donors
BRAIN DEAD - Can donate organs and tissues
(ventilator-dependent patient)
Donor after Cardiac Death (DCD) – can donate kidneys, liver, lungs, and tissues
(ventilator dependent patient)
CARDIAC DEAD - Can donate tissues
LIVING DONOR - Can donate kidney, partial liver or lung, bone marrow and blood
Misconception: Can take organs even if not on vent
Organs & Tissues That
Can Be Transplanted
Heart & Heart Valves
Liver
Intestines
Femoral Veins
Saphenous Veins
Tendons
New York Organ Donor Network
Corneas
Lungs
Kidneys
Pancreas
Skin
Bone
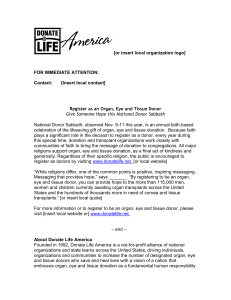
The Essential Issue
Need for Organ Donation in U.S.
98,357 as of 8:09am on 3/19/08
100,000
90,000
80,000
70,000
60,000
50,000
40,000
30,000
20,000
10,000
0
21,914
15,467
4,509
1990
29,415
37,609
16,627
4,520
19,044
5,100
1992 1994
50,130
20,494
5,419
1996
65,005
73,824
20,961
5,791
1998
22,953
5,984
2000
82,749
6,190
2002
88,149
24,891
27,035
7,151
2004
Deceased Donors Size of Waiting Lists Transplants
Source: United Network for Organ Sharing
Regulations
CMS (formerly HCFA) - Hospitals
Conditions of Participation
* Implemented August 1999
Hospitals required to:
– Notify OPO of all deaths immediately after expiration
– Notify OPO of all imminent deaths (Any ventilator dependent patient who exhibits neurological injury indicating evolvement to brain death)
Maintain patient viability to evaluate for brain death.
Request for organ donation will be made only by trained requestors.
NYSDOH, The Joint Commission, & CMS regulations all agree on organ donation.
Latest Revision Effective 1/1/07
Standard LD.3.110
“
The organization Leaders implements policies and procedures developed with the medical staff’s participation for procuring and donating organs and other tissues.”
Elements of Performance for LD.3.110 (A4):
The hospital notifies the OPO in a timely manner of a patient who has died, or whose death is imminent, as follows in the following ways:
In accordance with clinical triggers defined jointly with hospital medical staff and the designated OPO
Within time requirements jointly agreed to by the hospital and designated OPO (ideally, within one hour)
Prior to the withdrawal of any life-sustaining therapies including medical or pharmacological support
Source: Joint Commission Resources, http://www.jcrinc.com/12858/
Brain Death Determination:
The Beginning…
What do you do?
Starts with injury to brain and loss of reflexes…
1.
2.
3.
4.
5.
Recognize brain death and start BD protocol
Notify the OPO of possible donor
Support blood pressure with pressors/fluids
Do not mention donation to the family
Allow the OPO to approach after brain death has been discussed with family members or if family brings up disconnection
The Role of a Family Services Coordinator
Serve as a link between hospital staff and the potential donor families
Support families, answer their questions & address their concerns
Provide the opportunity for organ & tissue donation
Offer resources to families ( bereavement, burial assistance, victim services )
Inform families of our Donor Family Services program
Organ Donation Can Occur in
Two Ways
Heart-Beating Donors : Patient is declared dead based on Brain Death
Criteria
Non-Heart-Beating Donors : Patient is declared dead based on Cardio-
Pulmonary Criteria
Definitions
Brain Death: T he irreversible cessation of brain function, including the brain stem.
Donation after Cardiac Death (DCD): A procedure in which organs are surgically recovered following the pronouncement of death based on the “irreversible cessation of circulatory and respiratory functions”
Brain Death Determination
Know your hospital policy
While many policies are different, the criteria is same everywhere (NYS released new guidelines in Dec 2005)
– No response to painful stimuli
– No cranial reflexes: corneal, cold calorics, doll’s eyes
– Pupils fixed and dilated
– No spontaneous respirations (Apnea trial)
– Confirmatory test not required
Brain Death Determination:
EVALUATION PROCESS
Once a Referral is Made
On-site clinical evaluation by transplant coordinator - review of medical records
Physical examination
Monitor organ function (lab testing)
Establish suitability-patient declared brain dead/patient is medically suitable
Next of kin identified
When time is right approach is made to family
Criteria for Determining
Brain Death - Part I
PRE-EXISTING CONDITIONS
• Known mechanism of injury
• Absence of toxic CNS depression
• Absence of metabolic CNS depression
Criteria for Determining
Brain Death - Part II
CLINICAL EVALUATION
• No pupillary reflex
• No corneal reflex
• No oculocephalic reflex
• No oculovestibular reflex
• No gag or cough reflex
• Apnea
Brain Death Determination
Imminent Death in accordance with the
New York Organ Donor Network is defined as “any ventilator dependent patient who exhibits neurological criteria indicating evolvement to brain death”.
Categories of patient diagnoses that would give rise to “imminent deaths” of this definition are anoxia, traumatic head injury, brain tumor, and cerebral vascular accident.
Brain Death Determination
The determination of brain death is made by two clinical examinations:
For adults: two clinical assessments should be six hour apart unless a confirmatory test confirms the diagnosis of brain death. If a confirmatory test confirms the diagnosis of brain the clinical examination may be two hours apart.
The clinical examinations must be performed by an attending physician credentialed in neurology, neurosurgery or critical care intensivist (attending physician in any intensive care unit) who has agreed to perform brain death protocol by returning a signed review of this policy. Two separate attending physicians should perform the two clinical exams.
Brain Death Determination
Three Cardinal Findings in Brain Death - Coma, Absence of brainstem reflexes and
Apnea (all 3 must be present) :
Coma (unresponsiveness):
1. No response to sound including name; no grimacing to pressure applied to nailbeds (unless its spinally mediated), supraorbital ridge or tempo-mandibular joint;
2. No motor response to pain in all extremities.
Absence of brainstem reflexes:
– No pupillary response to light, size: mid-position (4 mm) to dilated (9 mm)
– No oculocephalic response (“Doll’s Eyes”):
May be tested only when no fractures or instability of the cervical spine are apparent
No eye movements to neck rotation
No vertical eye movement with neck flexion
– No oculovestibular reflex (“Cold Calorics”)
-Technique: a. Visualize the tympanic membrane to ensure that excess cerumen is removed and to check for rupture b. The patient remains supine with head tilted forward at 30 degrees c. Irrigate the external ear canal with 50 cc of ice water d. Observe eye movement for one minute e. Allow 5 minutes before testing opposite side
APNEA TEST: Technique
Patient must be apneic with adequate stimulus (pCO2 >60mmHg, pH
<7.40). The apnea test is generally performed after the second examination of brainstem reflexes. The apnea test need only be performed once when its results are conclusive. a. Check ABG record. Baseline ABG must be available b. Adjust ventilatory settings to achieve pCO2 of >35 mm Hg c. Ventilate patient with FiO2 100% for 10 minutes d. Connect pulse oximeter e. Disconnect ventilator f. Place cannula in trachea, deliver 100% O2 at 6L/m g. Observe for respiratory movements h. Adequate hypercarbia (pCO2 > 60 mm Hg or PCO2 increase is 20 mm
Hg over baseline normal PCO2) j. Observe for respiratory movements and draw ABG after approximately 8 minutes from the beginning of the apnea test k. Return patient to the ventilator at the completion of the apnea test
APNEA TEST, Cont.
Interpretation: a. If respiratory movements are absent and arterial pCO2 is > 60 mm Hg or increased 20 mm Hg over baseline normal, the apnea test result is positive b. If respiratory movements are observed, the apnea test is negative c. If respiratory movements are not observed and the pCO2 is < 60 mm Hg or increase in PCO2 < 20 mm Hg from baseline, the apnea test is indeterminate and should be repeated
Precautions: a. The apnea test may be done only when the following conditions are met:
-Temperature > 36.5 degrees C (97.7 F)
-Systolic blood pressure > 90 mm Hg
-Euvolemia.
-Normal PO2 (PO2 > 60 mm Hg on FIO2 < 60%) b. Discontinue apnea test if:
– Patient develops hypotension (systolic BP < 90 mm Hg)
– Patient develops significant oxygen desaturation
– Cardiac arrhythmias develop
– If any of the above events occur, immediately draw an ABG if possible and: reconnect the patient to the ventilator.
– If PCO2 is > 60 mm Hg or PCO2 increase is > 20 mm Hg over baseline normal PCO2, the apnea test is result positive.
Brain Death Determination
Confirmatory Tests
Brain death is a clinical diagnosis. In some patients, skull or cervical injuries, cardiovascular instability, or other factors may make it impossible to complete parts of the assessment safely. In such circumstances, a confirmatory test verifying brain death is necessary. Confirmatory tests are required ONLY if the following conditions which may interfere with the clinical examination are present and therefore make the diagnosis uncertain:
1. Severe facial or cervical spine trauma
2. toxic levels of any sedative drugs, aminoglycosides, tricyclic antidepressants, antiepileptic drugs, anticholinergics, neuromuscular blocking agents, or chemotherapeutic agents
3. Pulmonary dysfunction severe enough to make the apnea test impossible to perform or interpret (I.e. sleep apnea, chronic CO2 retention, uncorrectable hypoxemia).
The consulting neurologist, neurosurgeon or intensivist makes the determination whether a confirmatory test is necessary and which test should be used.
Brain Death Determination
Confirmatory Tests
The following confirmatory tests are available:
– Technetium-based nuclear brain scan: If no uptake of isotope in brain parenchyma and no cerebral blood flow, the test is positive
– Electroencephalograph: 30 minutes of continuous EEG recording showing electrocerebral inactivity, the test is positive. Tracings will comply with the minimum technical standards for EEG recording as outlined by the American Electroencephalograph Society.
*The ICU setting may result in false readings due to electronic backgrounds noise creating innumerable artifacts
– Transcranial Doppler Ultrasonography: No diastolic flow or reversed flow or small systolic peaks in early systole without diastolic flow or with reversal of flow are consistent with the diagnosis of brain death. Lack of Doppler signal cannot be interpreted as confirmation of brain death because 10% of patients do have temporal windows.
– Conventional cerebral angiography: No intercerebral filling at the level of the carotid bifurcation of circle of ‘Willis, the test is positive
Criteria for Donation After
Cardiac Death (DCD)
Patient has devastating non-recoverable illness or injury and is ventilator dependent
Decision is made for withdrawal of support according to patient wishes and hospital policy
Cardio-pulmonary arrest will likely occur within 60 minutes after withdrawal of support
Patient has good kidney and liver function
Location of withdrawal of support is changed to OR
DCD Procedure
Decision is made for withdrawal of support;
Withdrawal of support is approved by hospital;
Patient is evaluated for medical suitability for organ donation;
Next of kin/authorized party is provided option of Donation
After Cardiac Death and details about the procedure including opportunity to be present in OR;
Next of kin/authorized party makes decision to donate organs and written consent is obtained;
Organ Recovery Team is notified and assembled;
DCD Procedure (cont)
Patient will be transferred to OR on ventilator and monitor;
Patient will be connected to monitor and anesthesia machine in OR;
Blood samples will be drawn;
Recovery team will prep and drape patient;
Organ preservation solutions will be prepared;
Heparin will be given prior to withdrawal of support;
Recovery team will leave the room;
Support will be withdrawn by Attending
MD/Designee;
DCD Procedure (cont)
Family will be escorted into OR and provided emotional support;
When patient’s heart and respirations stop, family will be asked to leave room;
Patient will be pronounced dead;
DCD Procedure (cont)
Recovery team will re-enter room after family leaves;
Abdominal incision will be made after waiting 5 minutes;
Aortic cannula will be placed and aortic flush will be started;
Chest may or may not be opened;
Organs will be recovered;
If patient does not arrest, patient will be transferred to designated area and palliative care will be provided;
Reminders about DCD
Decision to withdraw support is separate from donation discussion
Withdrawal of support process should not be modified in any way because the patient is going to donate
If patient does NOT arrest within allotted time frame, the pt will be transferred back to the ICU or other pre-determined area. Comfort Care will continue as per hospital policy.
The ventilator will NOT be reinstated. The pt was going to be disconnected whether donation was taking place or not.
Consequences of Brain Death
•
Loss of Vasomotor tone - Hypotension
Altered perfusion
•
Hypothalamic dysfunction - Diabetes Insipidus
Hypothermia
•
Pulmonary dysfunction - Apnea
Infection
Neutrogena pulmonary edema
Potential Organ Donor: Clinical
Management Goals
• Hemodynamic Stability
• Normothermia
• Optimal oxygenation
• Fluid/electrolyte balance
• Prevent infection
Management of Patients Undergoing OD
Evaluation: Procedures
Arterial catheter
CVC catheter
Echocardiogram, if age < 65 for possible heart donation
Cardiac Catheterization if directed, for possible heart donation fiberoptic bronchoscopy / bronchoalveolar lavage (FOB/BAL) if directed for possible lung donation
Management of Patients Undergoing OD
Evaluation: Mechanical Ventilation
Control Mode Ventilation
Adjust frequency (breaths per minute) to maintain PaCO2 35-45 with normal pH
Adjust Vt 5-10 cc/kilogram, maintaining Peak
Inspiratory Pressure < 35 cm H20
Adjust FiO2 to maintain SaO2 > 90 %
Adjust Peep to maintain SaO2 > 90% on an fiO2 of < 50%
Management of Patients Undergoing OD
Evaluation: Hormonal Resuscitation Protocol
Administer IV boluses of:
– 20 micrograms T-4 (Thyroxine)
– 15 milligrams/kilogram methylprednisolone (Solumedrol)
– 1 unit Arginine Vasopressin
– 10 units regular insulin (not if BG < 100)
–
1 amp of D50 (50cc of D50% - contains 25 grams of glucose)
– if blood glucose < 300
Start continuous infusions:
– Start an Vasopressin drip: (concentration as per pharmacy). Start at 0.5 units per hour. Titrate up by 0.5 units every 5 minutes to keep SBP
>100, MAP > 60 not to exceed a maximal dose is 4.0 units/hr.
– Start a drip of 200 micrograms T-4 (thyroxine) in 500cc normal saline at
25cc (10 micrograms) per hour.
– Titrate T-4 by 2 microgram increments to maintain desired blood pressure – do not exceed 20 micrograms/hour
– Reduce levels of other vasopressors (if in place) as much as possible
– Start insulin drip (concentration as per hospital pharmacy) at 1unit/hr and adjust rate to maintain blood glucose 80 – 150 mg/dl.
– Glucose determinations by finger stick or serum every 1 hr.
website: www.donatelifeny.org
 0
0


Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users