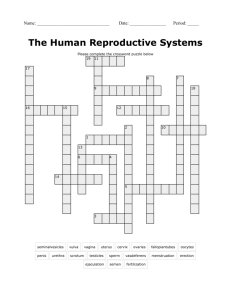
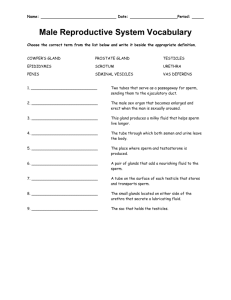
The Reproductive System: Chapter 16
advertisement

The Reproductive System: Chapter 16 I. II. Introduction Gonads primary sex organs (testes in males, ovaries in females) produce sex cells (gametes: sperm in males, ova in females) secrete sex hormones Reproductive role is to produce offspring. If the time is suitable, the sperm and egg (ovum) fuse to produce a fertilized egg, which is the first cell of the new individual. Once fertilization has occurred, the female uterus provides a protective environment in which the embryo, later called the fetus, develops until birth. Anatomy of the Male Reproductive System A. Testes (pl) – Testis (sing) olive sized divided into lobules and each lobule contains 1-4 tightly coiled seminiferous tubules seminiferous tubules: sperm forming factories Interstitial cells around the seminiferous tubules produce androgens like testosterone Exocrine and Endocrine function B. Duct System Epididymis Comma shaped, 20 feet long coiled on top and around testis Provides temporary storage for immature sperm Takes 20 days for sperm to travel through and mature to gain their swimming ability Ductus Deferens Propels live sperm from the storage site, epididymis, to the ejaculatory duct. At moment of ejaculation, the thick layers of smooth muscle create peristaltic waves to squeeze sperm forward. Vasectomy: minor operation in which a surgeon makes a small incision into the scrotum and cuts the ductus deferens to prevent sperm from reaching the body’s exterior. Urethra Extends from base of urinary bladder to the tip of the penis Carries both urine and sperm to the body exterior, but they never pass at the same time due to sphincter control C. Accessory Glands and Semen Seminal Vesicles Produces 60% of fluid volume of semen Produces thick, yellowish secretion, rich in sugar, vitamin C, and prostaglandins to nourish and activate the sperm Prostate Gland Size of chestnut, located just below the bladder Secretes a milky fluid that activate sperm Has a reputation as a health destroyer Can be felt by finger exam through the anterior rectal wall Hypertrophy of gland makes urination difficult and enhances risk of infections and kidney damage Prostatic cancer is the 3rd most prevalent in men Slow growing, hidden condition Bulbourethral Glands Pea size, inferior to prostate gland First secretion to pass down the urethra when man sexually excited Cleanses the urethra of traces of acidic urine and serves as lubricant Semen Milky, white, sticky mixture of sperm and accessory gland secretions III. IV. D. External Genitalia Scrotum divided sac of skin that hangs outside the abdominal cavity Hangs loosely to provide the testes a temp. 3 degrees C below body temp. (which is necessary for healthy sperm production) Penis Designed to deliver sperm in to female reproductive tract Consists of shaft that ends in enlarged tip, the glans penis. Skin covering penis is loose and folds downward to form cuff of skin, the foreskin. Often foreskin is surgically removed shortly after birth by circumcision. The urethra is surrounded by three elongated area of erectile tissue, a spongy tissue that fills with blood during sexual excitement. This causes the penis to enlarge and become rigid, erection. Male Reproductive Functions A. Spermatogenesis: sperm production Begins during puberty and continues throughout life Every day a man makes millions of sperm Process of spermatogenesis takes 64-72 days, but they are still unable to swim and must mature in the epididymis. Mature sperm: 1. Head contains DNA, the genetic material covered by helmet-like, acrosome that breaks down and releases enzymes that help sperm penetrate the egg when it is in close contact Midpiece mitochondria wrapped around it provide ATP needed to propel the sperm Tail Propel the sperm with whip like movements B. Testosterone Production Testosterone causes the secondary male sex characteristics to appear 1. deepening of voice due to enlargement of the larynx 2. increased hair growth over the body, esp. axillary and pubic regions and face 3. enlargement of skeletal muscles to produce the heavier muscle mass typical of the male physique 4. increased heaviness of the skeleton due to the thickening of the bones Anatomy of the Female Reproductive System A. Ovaries size and shape of almonds Each ovary contains many tiny structures called ovarian follicles that consist of an immature egg, called an oocyte As developing egg within a follicle begins to ripen or mature, the follicle enlarges. When mature, the developing egg is ready to be ejected from the ovary, an event called ovulation. After ovulation the ruptured follicle is transformed into the corpus luteum which eventually degenerates. Ovulation occurs every 28 days, but it can vary. B. Duct System Fallopian Tubes Receive the ovulated oocyte and provide a place for fertilization to occur. About 4 inches long and extends from ovaries to uterus. There is no actual contact between fallopian tubes and ovaries instead the ends of the fallopian tubes have fingerlike projections, fimbriae, which surround the ovary and wave the oocyte from the ovary into the tube. The oocyte is carried to the uterus by peristaltic contractions and the beating of cilia. The journey can take 3-4 days and the oocyte is only viable for 24 hours, the fallopian tubes are the usual site of fertilization Sperm must swim against the current of the cilia to reach the oocyte. Uterus Located between the bladder and rectum Hollow organ that functions to receive, retain, and nourish a fertilized egg. 3 portions: body, fundus, cervix Cancer of the cervix is common among women between the ages of 30 and 50. Pap smear is the single most important diagnostic test for detecting this slow-growing cancer. 3 layers: endometrium: inner layer implantation of embryo occurs in this layer and resides there during development when a woman is not pregnant, the endometrial lining is sloughed off about every 28 days myometrium: middle layer of muscle in the uterus composed of smooth muscle that plays an active role during delivery of a baby, when it contracts rhythmically to force the baby out of the mother’s body. epimetrium: outer layer V. Vagina Thin-walled tube 3-4 inches long extending from cervix to the body exterior Called the birth canal providing the passageway for the delivery of an infant and for the menstrual flow to leave the body. Receives the penis during intercourse; therefore, female organ of copulation Distal end of vagina closed by hymen that tends to bleed when it is ruptured during the first sexual intercourse, but it can be torn during sports or tampon insertion. C. External Genitalia: Vulva mons pubis: fatty, rounded area overlying the pubic bone, covered by pubic hair labia majora: two elongated folds covered by hair labia minora: two delicate hairless folds inside of the labia majora The labia majora enclose a region called the vestibule, which contains the openings of the urethra and vagina. Just anterior to the vestibule is the clitoris, which is a structure corresponding to the male penis that is composed of erectile tissue that becomes swollen with blood during sexual excitement. Female Reproductive Functions and Cycles A. Oogenesis and the Ovarian Cycle oogenesis: production of female sex cells By birth the female’s lifetime supply of oocytes (approx. 700,000 of them) are already in place in the ovarian follicles. At puberty, the anterior pituitary gland begins to release FSH which stimulates a small number of primary follicles to grow and mature each month, and ovulation begins to occur each month. These cyclic changes that occur monthly constitute the ovarian cycle. Only about 400-500 of the potential 700,000 ova are released in a female’s lifetime. B. Menstrual Cycle: cycle that the endometrium goes through each month after month as it responds to changes in the levels of ovarian hormones in the blood. Days 1-5: Menses Thick endometrial lining sloughed off Bleeding 3-5 days Blood loss is about ¼ to ½ cup. Days 6-14: Proliferative Stage Stimulated by rising estrogen levels produced by the growing follicles of the ovaries, the endometrium is repaired, glands formed, and blood supply is increased. VI. VII. Endometrium is once again velvety and thick Ovulation occurs at the very end of this stage in response to a surge of LH in the blood. Days 5-28: Secretory Stage Rising levels of progesterone produced by the corpus luteum of the ovary act on the endometrium and increase its blood supply more Endometrial glands begin to secrete nutrients If fertilization does not occur, the phases are repeated about every 28 days. C. Hormone Production by the Ovaries Estrogens Produced by the Follicle cells of the growing and mature follicles Cause the appearance of the secondary sex characteristics: Enlargement of accessory organs of female reproductive system Development of breasts Appearance of axillary or pubic hair Increased deposits of fat beneath the skin in general Widening and lightening of the pelvis Onset of menses, or the menstrual cycle Progesterone Produced by the corpus luteum as long as LH is present in the blood Produced by the placenta in pregnancy, not the ovaries. Mammary Glands Present in both sexes, but they function only in females Role is to produce milk to nourish a newborn baby Estrogen causes the female mammary glands to increase in size at puberty. Cancer of the breast Leading cause of death in American women. 1 in 8 women will develop this condition Signaled by a change in skin texture, puckering, or leakage from the nipple Mammograms: x-ray examination detects breast cancer too small to feel Survey of the Pregnancy and Embryonic Development A. Accomplishing Fertilization An oocyte is fertilizable for up to 24 hours, sperm are viable within the female reproductive tract for up to 72 hours. Consequently, for fertilization to occur, sexual intercourse must occur no more than 72 hours before ovulation and not later than 24 hours after, at which point the oocyte is approximately one-third of the way down the uterine tube. It takes 1-2 hours for a sperm to complete the journey up the female duct system to the end of the uterine tubes. Following sperm penetration, the secondary oocyte completes meiosis II. Then ovum and sperm nuclei fuse (Fertilization) forming a zygote. B. Events of Embryonic and Fetal Development If fertilization occurs, embryonic development begins immediately. Cleavage, a rapid series of mitotic divisions without intervening growth, begins with the zygote and ends with a blastocyst. By day 14 after ovulation, the young embryo (blastocyst) has implanted in the endometrium and the placenta is being formed. hCG released by the blastocyst maintains hormone production of the corpus luteum, preventing menses, until the placenta assumes its endocrine role. The placenta serves respiratory, nutritive, and excretory needs of the embryo and produces hormones of pregnancy. It is generally functioning by the 3rd week. All major organ systems have been laid down by 8 weeks, and at 9 weeks the embryo is called a fetus. Growth and tissue-organ specialization are the major events of the fetal period. C. Effects of Pregnancy on the Mother 1. Anatomical changes The uterus enlarges during pregnancy from the size of a fist to occupy most of the pelvic cavity by 16 weeks. The increasing bulkiness of the abdomen changes the woman’s center of gravity. Placental production of the hormone, relaxin, causes pelvic ligaments and the pubic symphysis to relax, widen and become flexible. This increased motility eases birth passage, but it may also result ina waddling gait during pregnancy. Good maternal nutrition is necessary throughout pregnancy if the developing fetus is to have all the building materials it needs to form its tissue and organs. Even though a mother is eating for two, she does not need to eat twice as much food, only about 300 more calories a day. The emphasis should be on high-quality not quantity. 2. Physiological Changes Gastrointestinal System a. Suffer nausea, commonly called morning sickness, until system adjusts to the elevated levels of progesterone and estrogen b. Heartburn is common because the esophagus is displaced and the stomach is crowded c. Constipation is another problem because motility of the digestive tract is declined during pregnancy. Urinary System a. Kidney dispose of fetal metabolic waste also b. Because she produces more urine during pregnancy and the Uterus compresses the bladder, urination is more frequent, more urgent, and sometimes uncontrollable. Respiratory System a. Nasal mucosa responds to estrogen by becoming swollen and congested; thus, nasal stuffiness and occasional nosebleeds occur. b. Vital capacity and respiratory rate increase, but residual volume decreases, so many women exhibit dyspnea (difficulty breathing) during the later stages of pregnancy. Cardiovascular System a. Total body water and blood volume increases 25-40% to accommodate the additional needs of the fetus. b. Blood pressure and pulse typically rise and increase cardiac output by 20-405 which helps propel the greater blood volume around the body D. Childbirth (parturition) Due date is 280 days from the last menstrual period. 1. Initiation of Labor During the last few weeks of pregnancy, estrogens reach their highest levels in the mother’s blood, which has two important consequences. 1. causes the myometrium to form abundant Oxytocin receptors (allowing it to become more sensitive to the hormone Oxytocin) 2. Interferes with progesterone’s quieting influence on the uterine muscle, which results in weak, irregular contractions called Braxton Hicks contractions – false labor. As birth nears, two more chemical signals cooperate to convert the false labor pains into the real thing 1. Certain cells of the fetus begin to produce Oxytocin, which in turn stimulates the placenta to release prostaglandins. Both of these hormones stimulate more frequent and powerful contractions of the uterus. 2. At this point, the increasing emotional and physical stresses activate the mother’s hypothalamus, which signals fro Oxytocin release by the posterior pituitary. VIII. 3. These combined effects of rising levels of Oxytocin and prostaglandins initiate the rhythmic, expulsive contractions of true labor. Positive feedback mechanisms – stronger contractions cause the release of more Oxytocin causing even more vigorous contractions. 2. Stages of Labor Stage 1: Dilation Stage Time from the appearance of true contractions until the cervix is fully dilated by the baby’s head (about 10 cm in diameter) As contractions progress, the infant’s head is forced against the cervix and it begins to soften, become thinner (effaces) and dilates. Amniotic fluid is released (water breaks) Longest part of labor – usually last 6-12 hours. Stage 2: Expulsion Stage Time from full dilation to delivery of the infant In this stage, the infant passes through the cervix and vagina to the outside of the body. Mother feels the urge to push with abdominal muscles. Phase can take as long as 2 hours, it is typically 50 minutes in a first birth and around 20 minutes in subsequent births. During an extremely prolonged stage 2, dystocia may occur. This is a condition when oxygen delivery to the infant is inadequate, leading to fetal brain damage. To prevent this, a cesarean section (C-section) may be performed. A C-section is delivery of the infant through a surgical incision made through abdominal and uterine walls. Stage 3: Placental Stage Delivery of the placenta, usu. Takes about 15 minutes. Developmental Aspects of the Reproductive System Sex of an individual is determined at time of fertilization (males have X and Y chromosomes and females have XX), but the gonads do not develop until the 8th weeks of embryonic development. The presence or absence of testosterone determines whether male or female accessory reproductive organs are formed. The reproductive system is inactive during childhood. Reproductive organs mature and become functional for childbearing during puberty. In males, puberty onset, occurring around 13 years old, is signaled by the enlargement of the tests and scrotum followed by the appearance of pubic, axillary, and facial hair. Growth of the penis goes on over the next 2 years and sexual maturation is indicated by the presence of mature sperm in the semen. In females, the first sign of puberty, around 11 years old, is the budding breasts. The first menstrual period, called menarche, usually occurs about 2 years later. Dependable ovulation and fertility are deferred until the hormonal controls mature, and event that takes nearly two more years. Tumors of the breast and cervix are the most common reproductive cancers in adult females, and prostate cancer is a widespread problem in adult males. During menopause, female reproductive capabilities end, and reproductive organs begin to atrophy. Hot flashes and mood changes may occur. Reproductive capacity does not appear to decline significantly in aging males.