Dee Chapter 31 : Foot Fractures
advertisement

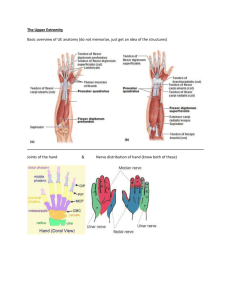
Tendon transfers Dee Chapter 60 OKU Hand Topics Principles of tendon transfer Radial nerve palsy Median nerve palsy Ulnar nerve palsy Combined nerve lesions Principles of tendon transfer Fundamental concept Recipient musculotendinous unit is more important to limb function than the donor unit Alternatives to tendon transfer Neurorrhaphy Intercalary tendon graft Tendon lengthening Tenodesis Free muscle transfer Arthrodesis Main requirements 1. 2. 3. 4. 5. 6. Supple skin, subcutaneous tissue and joint Muscle must have adequate power Muscle must have sufficient amplitude (or excursion) Must have a satisfactory line of pull Preferably synergistic action Functional integrity of the donor function must be preserved Supple skin, subcut and joint Power Amplitude or excursion Line of pull Synergistic Donor function Must not have joint or soft tissue contracture Directly proportional to cross sectional area of muscle Independant of length or excursion Work capacity of muscle = power x amplitude (kg.m) Potential excursion is the difference between maximal length on traction, and length at maximal contraction Usually resting length is directly in the middle of these 2. i.e. Excursion = (tension length – resting length) x 2 Should be as straight as possible Each turn or bend reduces power and amplitude Preferably should be synergistic to new action But sometimes not possible, doesn’t have to be Must be maintained by another capable muscle to prevent imbalance Surgical considerations Timing of surgery depends on Joint need preop contracture release, splinting, therapy Skin/subcut may require pedicle or free flap Power must match the lost muscle Also transferred muscle usually loses 1 power grade, so must use a muscle that is minimum 4+ or 5 Practical guidelines: Wrist motors 30mm Finger extensors 50 mm Finger flexors 70mm New function more easily learnt if synergistic cause of problem prognosis for recovery patient preference to some extent Nerve problems may want to wait for nerve to recover to see eventual function may also consider alternative like neurolysis, neurorrhaphy + N grafting Indications for early tendon transfer < 12 weeks 1. proximal N lesions 2. irreparable N lesions 3. other lesions with statistically poor chance of acceptable recovery 4. donor tendon completely expendable 5. no imbalance will be created later by nerve regeneration Skin planning and incisions Pre-op planning – list of deficits vs list of available donor muscles Multiple short transverse incisions are better than long ones Need soft tissue cover over tendon junctures May use end-to-side, end-to-end, or tendon weave Radial nerve palsy Functional impairment No wrist extension No MCPJ extension Loss of abduction and extension of thumb Without wrist extension there can be no power grip Usually sensory component is not significant in radial N palsy If PIN only, wrist extension may be preserved by functioning ECRL – so no need to address wrist Treatment Most use dynamic extension splints and OT to keep wrist, hand and fingers supple Some suggest early transfers which serve as internal splints controversial and not used by everybody early PT (pronator teres) to ECRB end to side transfer o PT still works as a pronator o But also allows wrist extension – power grasp o May make external splinting unnecessary o If inadequate motor function returns, then extra transfers for MCPJ extension and thumb extension/abduction Some common transfers for radial N palsy FCU retained for important role in wrist flexion PT used for wrist extension because of work capacity and also pronator function still preserved FDS long and ring fingers passed through hole in interosseus membrane to transfer to their target muscles mobilised proximally so that when their muscle mass sits in the hole, rather than the tendon to avoid adherence at transfer site FCR is strong abductor of thumb MC Easier to do than boyle But main disadvantage is use of FCU as a donor because wrist works in radial dorsiflexion and ulnar palmarflexion Restores wrist and MCP extension as well as thumb abduction/extension Boyle PT to ECRB FCR to EPB and APL FDS long finger to EDC FDS ring finger to EPL and EIP Green PT to ECRB FCU to EDC PL to rerouted EPL PT to ECRB FCR to EDC PL to rerouted EPL Alternative to Green to avoid FCU use Median nerve palsy Functional impairment Sensory component is very important and needs to be addressed Motor deficit low median N distal forearm o Opponens poll, APB and to varying extent FPB o 1/3 of patients have sufficient strength in FPB that opponens transfer is not required high median N o in addition to opponens, APB and FPB - entire FDS, FDP to index/long and FPL are lost o FCR not working but functional wrist flexion comes from FCU (ulnar N) Treatment Opponens function Try to see if opponens function can be preserved Residual FPB function in 1/3 patients Neurorrhaphy or nerve grafting If not then surgery Prerequisites are good skin and supple joints. May need pre-transfer release of 1st web space contracture if present Opponensplasty Much experience gained in polio patients Stronger donor must be selected if thumb adductor, 1st dorsal interosseus and EPL are functioning If combined lesions and above paralyzed, can use weaker donor Usual opponensplasty donors 1. PL – Camitz transfer o Test by opposing thumb and little finger and flexing wrist 2. FDS to ring (through FCU loop) 3. EIP or EDQP o Test by doing the Horn sign – 3rd, 4th fingers flexed, 2nd and 5th fingers extended Median N palsy Low median nerve palsy Antagonists of opponens are functioning so strong motor is required Line of pull for opponens function should be from the pisiform area Half of FCU tendon used to make a sling at the level of the pisiform Longstanding CTS with thenar wasting Ring finger FDS usually used for opponens plasty Harvested proximal to metacarpal A1 pulley Through FCU sling Subcutaneous to insert into tendon of APB or dorsoulnar base of 1MC (Alternative tendons are PL, EIP, EDQP, ECU) Camitz transfer After CTS release, can transfer PL to APB to provide palmar abduction of thumb (Or FDS4, EIP, EDQP, ADM) EIP, EDQP, ECU, Abd dig min for opponensplasty High median nerve palsy FDS, FDP2,3 and FPL gone FCU still functioning to allow wrist flexion Since FDS gone, cannot use FDS4 for opponensplasty use alternatives FDP2,3 side-to-side attached to FDP4,5 for long finger flexion – if more power needed, ECRL can be transferred to FDP 2,3 BR to FPL for thumb IPJ flexion Ulnar nerve palsy Functional impairment Loss of interossei and ulnar 2 lumbricals Loss of independant MCPJ flexion Difficulty in coordination of proper finger flexion without MCPJ flexion Because FDS and FDP cause flexion of IPJs first with only secondary MCPJ flexion later Gripping large objects a problem because unable to start grasp with MCPJ flexion Power grip severely impaired Loss of abduction and adduction of fingers impairs dexterity Loss of adductor pollicis Loss of key pinch ability Compensatory hyperflexion of thumb IPF (to increase mechanical advantage of EPL as secondary adductor) = Froment’s sign Clawing Usually seen in ulnar 2 fingers Again due to weak MCPJ flexion resulting in IPJ flexion with MCPJ extension Without exercise/splinting, fixed contractures can occur High ulnar N Loss of FCU for wrist flexion, and FDP 4,5 Paradoxically less clawing But significantly reduced powergrip now Sensation Significant but not as bad as median N sensory loss Treatment Aim to restore key pinch function and compensate for loss of active MCPJ flexion High ulnar lesions – replace FCU Ulnar N palsy Key Pinch grip Requires stable thumb MC, MCPJ and index finger Important to reproduce Adductor Pollicis function Static procedures Loss of active MCPJ flexion Used when full IPJ extension can be achieved when MCPJ extension is blocked BR or ECRB transfer free tendon graft sutured to ulnar base of thumb PP brought across adductor muscle and taken dorsally through 3rd web then secured to BR or ECRB which have been mobilised to create enough length Others consider thumb MCPJ or IPJ fusion ± transfer to improve index finger abduction Static procedures to prevent hyperextension of MCPJ bone blocks MCPJ arthrodesis Volar plate capsulorrhaphy None of these can increase power grip Ulnar N palsy High ulnar N Dynamic procedures Dynamic tendon transfers Fixed flexion contractures present Or Extensor mechanism already stretched and there is extension lag of IPJs when MCPJ hyperextension is prevented FDP4,5 weakness FCU weakness Mainly designed to produce primary flexion at MCPJ May improve power grip Originally FDS used but does not improve power grip Now extensor tendons can be used Usually transfer is passed through lumbrical canal, under transverse MC ligament into lateral band of finger (can cause PIPJ hyperextension) PP Or A2 pulley FDP2,3 attached side to side to improve FDP4,5 function 1/2 or all FCR transferred to FCU Combined nerve lesions Difficult because limited motors available for transfer Prevent contractures and deformity Often lack of donor muscle may mean increasing use of static procedures like tenodesis, fusion, etc