View/Open - Lirias
advertisement

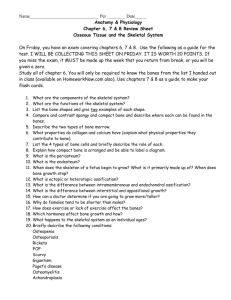
For submission to BONE Uncovering the Periosteum for Skeletal Regeneration: The Stem Cell That Lies Beneath Scott J. Roberts1,2,3#, Nick van Gastel2,4#, Geert Carmeliet2,4 and Frank P. Luyten1,2* 1Skeletal Biology and Engineering Research Center, KU Leuven, O&N 1 Herestraat 49 bus 813, 3000 Leuven, Belgium. 2Prometheus, Division of Skeletal Tissue Engineering, KU Leuven, O&N 1 Herestraat 49 bus 813, 3000 Leuven, Belgium. 3Institute of Orthopaedics and Musculoskeletal Science, Division of Surgery & Interventional Science, University College London, The Royal National Orthopaedic Hospital, Stanmore, Middlesex, HA7 4LP, UK. 4Clinical and Experimental Endocrinology, KU Leuven, O&N 1 Herestraat 49 bus 902, 3000 Leuven, Belgium. # These authors contributed equally to this work *Corresponding Author: Skeletal Biology and Engineering Research Center, O&N1 Herestraat 49 bus 813, 3000 Leuven, Belgium Tel: +32 16 34 25 45 Fax: +32 16 34 62 00 Email: frank.luyten@uzleuven.be Keywords: Periosteum, Stem Cells, Bone Development, Fracture Repair, Tissue Engineering 1 Abstract The cartilage- and bone-forming properties of the periosteum have long since been recognized. As one of the major sources of skeletal progenitor cells, the periosteum plays a crucial role not only in bone development and growth, but also during bone fracture healing. Aided by the continuous expansion of tools and techniques, we are now starting to acquire more insight into the specific role and regulation of periosteal cells. From a therapeutic point of view, the periosteum has attracted much attention as a cell source for bone tissue engineering purposes. This interest derives not only from the physiological role of the periosteum during bone repair, but is supported by the unique properties and marked bone-forming potential of expanded periosteumderived cells. We provide an overview of the current knowledge of periosteal cell biology, focusing on the cellular composition and molecular regulation of this remarkable tissue, as well as the application of periosteum-derived cells in regenerative medicine approaches. 2 1. Introduction The osteogenic potential of the periosteum, a thin vascular membrane that covers the external surface of bone except for the articular surfaces of the long bones, was described for the first time in 1742 by Henri-Louis Duhamel du Monceau[1]. His findings were later confirmed by Louis Xavier Ollier, who showed that upon treatment of bone fractures the integrity of the periosteum must be retained to achieve successful healing[2]. Subsequently, research has revealed that the periosteum consists of two layers (Fig. 1): an outer fibrous layer containing fibroblasts dispersed in between collagen fibers, and an inner cambium layer which contains skeletal progenitor cells and osteoblasts, and is highly vascularized and innervated[3]. The periosteum serves as an attachment site for tendons, ligaments and muscles. In addition, periosteal blood vessels deliver 70-80% of the blood supply to the bone cortex[4]. Furthermore, progenitor cells in the cambium layer continuously give rise to osteoblasts to allow appositional bone growth as well as cortical bone modeling and remodeling in concert with osteoclasts. The astounding potential of the periosteum is however mainly revealed after bone fracture, when periosteal progenitor cells undergo an impressive expansion, followed by differentiation into osteoblasts and chondrocytes, but predominantly the latter. This process forms the cartilaginous fracture callus that undergoes hypertrophy, followed by replacement by bone and eventual remodeling to restore the original shape of the bone[5, 6]. This remarkable property of the periosteum has elicited extensive research into the use of periosteum-derived cells for regenerative approaches, and preclinical studies demonstrating the potential of these cells in the treatment of non-healing bone fractures and large bone defects are becoming available. 3 In this review, we summarize recent findings expanding our insight into the cellular composition and molecular regulation of the periosteum, and provide an overview of regenerative medicine approaches using periosteum-derived cells, as well as clinical attempts to mimic the periosteum for improved fracture healing. 2. The periosteum during skeletal development, growth and aging Developmental origin of the periosteum Embryonic bone formation can proceed through either the intramembranous or the endochondral pathway. During intramembranous ossification, mesenchymal stem/progenitor cells will condense and differentiate into osteoprogenitor cells expressing runt-related transcription factor 2 (RUNX2) and osterix (OSX), which in turn give rise to osteoblasts, the mature bone-forming cells[7]. During this process, undifferentiated progenitor cells remain at the bone periphery, forming the periosteum. These cells will drive further appositional growth of the bones by giving rise to new osteoblasts[8]. The formation of an entire bone by the direct differentiation of progenitors to osteoblasts is rather the exception and is responsible for the formation of only a few bones, such as the flat bones of the skull. In contrast, most bones develop through endochondral ossification, a process in which initially a cartilage template is laid down, that is later replaced by bone[9]. More precisely, during the development of the long bones, mesenchymal stem/progenitor cells expressing paired-related homeobox gene 1 (PRX1) will condense and give rise to chondrocytes, which express the transcription factor sex determining region Y box 9 (SOX9)[10, 11], in the inner part of the condensation, while at the periphery undifferentiated cells remain to form a perichondrium. As the chondrocytes proliferate and the cartilage anlage grows, cells in the center will stop proliferating, enlarge and 4 become hypertrophic. These hypertrophic chondrocytes will mineralize their surrounding matrix and attract blood vessels, chondroclasts and osteoprogenitor cells[9]. In addition, they play an important role in directing adjacent perichondrial cells to become osteoblasts and form a mineralized bone collar, thus converting the perichondrium into periosteum. Several molecular signals have been shown to link the development of the cartilage anlage with that of the surrounding perichondrium/periosteum, including the Indian hedgehog/parathyroid hormonerelated protein, bone morphogenetic protein (BMP) and fibroblast growth factor (FGF) signaling pathways[9, 12-14]. The crucial role of the periosteum during further bone development is highlighted by the fact that the periosteal layer will not only serve as the source of osteoprogenitor cells that invade the cartilage template to form the primary ossification center[15], but it will also contribute to the radial growth of the long bones by continuously producing mature osteoblasts from periosteal progenitor cells[16]. The periosteum during skeletal growth and aging Periosteal bone apposition is a cardinal feature of skeletal growth. Long bones grow wider as they grow taller, and there is extensive individual variation in this process[16, 17]. One of the most striking determinants of periosteal apposition in humans is gender. There is little difference between the sexes in the extent of periosteal apposition until puberty, when periosteal expansion markedly accelerates, especially in men when sexual dimorphism appears[16-18]. The skeletal gender differences in radial bone growth are traditionally attributed to the actions of sex steroids. In the periosteum, estrogens promote the expansion of early osteoblast progenitors but inhibit their differentiation by osteogenic agents such as parathyroid 5 hormone (PTH) or BMP2, thus limiting periosteal bone expansion[19, 20]. Androgens in contrast stimulate both the proliferation of early periosteal osteoprogenitors and their differentiation to mature osteoblasts. Current evidence further indicates that in addition to differences in sex steroid secretion, skeletal sexual dimorphism also depends on gender-related differences in growth hormone/insulin-like growth factor 1 signaling and sensitivity to mechanical loading[18]. At the completion of longitudinal growth, periosteal apposition will decrease to no more than a few millimeters per year and, together with continued endosteal resorption, result in thinning of the cortical shell[16, 17]. Biomechanical analyses suggest that these changes in bone size have important implications for the determination of fracture risk in the elderly. In addition to many factors that affect adult periosteal bone apposition, including mechanical forces, nutrients, endocrine factors and lifestyle, an important gender difference remains during adulthood and aging. Men experience a greater rate of periosteal growth with aging, leading to a superior ability to maintain bone strength and protection against age-related fracture risk. This might again be related to differences in sex steroid levels, as orchidectomy reduces and ovariectomy increases periosteal bone formation in adults[21]. Since periosteal and endosteal/trabecular osteoprogenitor cells seem to respond differently to sex steroids as well as antiresorptive and anabolic osteoporotic drugs[3], targeting the periosteum with anabolic agents such as PTH or androgens may prove a potent approach for fracture risk reduction in osteoporotic patients or the elderly. 6 3. The periosteum as a central mediator of bone healing Bone repair: the cellular picture Bone is one of few tissues that can heal without forming a fibrous scar. The process of fracture healing largely recapitulates bone development, although it differs slightly due to the presence of inflammation and mechanical loading[22]. The bone healing process comprises 4 different phases: an initial inflammatory response and recruitment of skeletal progenitor cells, the formation of a cartilaginous callus, the replacement of cartilage by spongy bone and finally the remodeling of the immature bone into mature lamellar bone (Fig. 2). Immediately following bone trauma, as a result of rupture of blood vessels, a hematoma is generated that consists of cells from both peripheral blood and the intramedullary hematopoietic compartment. The injury also initiates an inflammatory response, necessary for the removal of necrotic tissue and debris from the fracture site and for the healing to proceed. During this phase, chemokines and inflammatory cytokines including tumor necrosis factor alpha (TNFα), interleukin 1 (IL1) and IL6 are secreted to recruit inflammatory cells while hypoxia at the fracture site will induce the production of VEGF and other angiogenic factors to stimulate neoangiogenesis[23]. In addition, a myriad of growth factors, including transforming growth factor beta 1 (TGFβ1), BMPs, FGFs, stromal-derived factor 1 alpha (SDF1α) and platelet-derived growth factor (PDGF), are released by platelets and inflammatory cells present in the fracture hematoma, triggering the activation and proliferation of skeletal progenitor cells in the periosteum[23-27]. 7 Depending on the biomechanics of the fracture site, periosteal cells will then differentiate into chondrocytes and/or osteoblasts. While strictly stabilized fractures (i.e. fractures in which the broken ends are closely opposed and mechanically stabilized) heal through intramembranous ossification, partially stabilized or nonstabilized fractures show the presence of large amounts of cartilage and heal through the endochondral pathway[28]. These observations might be related to the inability of blood vessels to develop properly in an unstable environment[29]. If the fracture is held stable, blood vessel bridging can occur, along with rapid union by periosteal and endosteal direct bone formation. In contrast, when motion is present at the fracture site, stable blood vessel formation is hampered and the periosteal cells near the fracture ends will differentiate into chondrocytes. In periosteal tissue further away from the fracture site, where less movement is present, periosteal cells can differentiate into osteoblasts, forming woven bone. As the endochondral callus provides new stability to the fracture site and as chondrocytes undergo hypertrophy, blood vessels and osteoprogenitor cells are attracted from nearby periosteal regions. The cartilage template is thus completely replaced by woven bone through mechanisms similar to those that govern embryonic bone development. In parallel a new cortical shell is formed by the bridging of the bony periosteal callus ends, providing the fracture with a semi-rigid structure which allows weight bearing[22]. In the final phase of fracture healing the woven bone is replaced by mature lamellar bone through the cooperation of osteoclasts and osteoblasts, gradually restoring the original bone shape including the establishment of a medullary cavity. Throughout all of these phases, the periosteum plays a central role. Several animal studies have shown that removal of the periosteum drastically affects bone repair[5, 6, 30], and cell tracing experiments have revealed that up to 90% of cartilage and 8 woven bone in the early fracture callus derives from the periosteum[30]. The tendency of periosteal cells to initiate endochondral ossification upon bone injury appears to be a distinctive periosteal characteristic, as endosteal or bone marrow injuries heal exclusively by intramembranous bone formation[5]. This difference in preferred bone formation pathway may furthermore represent an intrinsic difference between periosteal and bone marrow stromal progenitor cells, as it appears to be maintained even when cells have been expanded ex vivo[31]. Molecular signaling pathways controlling the periosteal response upon fracture The most studied signaling cascade with respect to bone fracture repair is the BMP pathway. During the early stages of endochondral fracture repair BMP2, 4, 5, 6, 7 and 8, as well the receptors BMPR1A and BMPR2, can be detected in activated periosteal cells and inflammatory cells in the granulation tissue[25, 27]. However, while different BMP ligands are expressed, some degree of redundancy and/or overlapping functions appear to exist, as fracture repair in mice in which Bmp4 or Bmp7 was deleted in the limb (Prx1-Cre) progressed normally[32, 33]. In contrast, in bones lacking Bmp2 (Prx1-Cre), the early steps of fracture healing are blocked and skeletal progenitors at the repair site are not able to differentiate into chondrocytes or osteoblasts[34]. Furthermore, two groups have further provided evidence that endogenous BMP2 signaling in periosteal cells is particularly important to initiate their osteochondrogenic differentiation and secure bone healing, although BMP2 seems not to be required for the initial periosteal expansion[35, 36]. Additional evidence for the importance of endogenous BMP signaling in human cells has been provided by 9 overexpressing the BMP antagonist Noggin in human periosteum-derived cells, which completely abrogates their in vivo bone-forming capacity[37]. In addition to BMPs, the role of FGF signaling in bone healing has been extensively studied. Expression of several FGF ligands, including Fgf2 and Fgf5, is markedly increased during the very early stages of callus formation[26]. Moreover, progenitor cells in the periosteum and the early periosteal callus have been shown to express FGFR1 and respond to FGF2 and FGF9[38-40]. In line with this, several studies have explored the use of FGF2 to promote bone healing, showing that administration of a single dose of this factor at the fracture site can stimulate callus formation by enhancing the proliferation of periosteal cells[41]. Recent work from our own group has furthermore provided evidence that FGF2 not only functions as a trigger for periosteal cell proliferation, but also primes the cells for their subsequent osteochondrogenic differentiation and increases their production of BMP2[31]. In line with its role during bone development, expression of Indian hedgehog can be detected in the early cartilaginous callus[42, 43]. A recent study has further highlighted the importance of periosteal hedgehog signaling for bone healing by deleting Smoothened, the receptor that transduces all hedgehog signals, in the periosteum of bone grafts[44]. Disruption of hedgehog signaling markedly reduced periosteal callus formation, suggesting that this pathway plays a significant role in adult bone repair via enhancing differentiation of periosteal progenitors[44]. Furthermore, the use of periosteal progenitor cells overexpressing sonic hedgehog significantly improves the healing of devitalized allogeneic bone grafts, demonstrating the therapeutic potential of targeting this pathway in periosteum-mediated bone repair[45]. 10 In addition, several other molecular pathways are emerging as regulators of periosteal cell function during bone healing. During the early stages of fracture healing, inflammatory mediators such as TNFα may influence periosteal cell fate[46]. The importance of the local inflammatory environment for periosteal cell activation and differentiation has further been proven by genetic studies targeting cyclooxygenase 2 (COX2), an enzyme with a central role in prostaglandin production, showing that expression of COX2 in the injury milieu is essential for successful periosteal progenitor cell-initiated bone healing[47, 48]. The Notch signaling pathway, which is known to control the maintenance of stromal stem/progenitor cells in bone marrow[49], has also been implicated in the activation of periosteal cells during the early stages after fracture[50]. Furthermore, Wnt signaling appears to play an important role in the osteogenic commitment of periosteal progenitor cells[37, 51, 52], similar to its role during bone development and homeostasis[53]. Taken together, it is clear that our understanding of the signaling pathways that are activated during fracture repair has increased substantially during the last few years. This provides hope for the development of therapeutic strategies that target the periosteum, or its resident progenitor cells, for the improvement of bone healing, including the treatment of non-unions and large bone defects. 4. The periosteum as a promising cell source for bone regeneration strategies Isolation and characterization of skeletal progenitor cells derived from the periosteum To isolate periosteal tissue from the bone of patients, a periosteum elevator is typically used. This tool, shaped like a curved chisel, is designed to maintain the 11 integrity of the periosteum by cutting the Sharpey’s fibers that anchor the periosteum to the bone[54]. Periosteum-derived cells (PDC) are then obtained by enzymatic digestion of the tissue or by spontaneous cell egression from the biopsy onto plastic cell culture dishes. It is currently not known whether these alternative isolation methods confer cells of identical functionality. For the isolation of animal PDC, either a similar technique is used or the periosteum is isolated by simply peeling off the periosteal layer from the bone. This method is particularly useful in young animals where the periosteal layer is relatively thick and only loosely attached to the bone[5559]. In adult mice, the periosteum is only a few cell layers thick and thus difficult to isolate by dissection. However, the use of murine PDC has several advantages in the study of periosteal biology, as variability between mice is much smaller than between human donors, and isolation of PDC from transgenic mice can provide unprecedented insight in the molecular regulation of periosteal cells. To overcome this limitation, we have recently developed a technique allowing the isolation of PDC from adult mice, using an enzymatic digest directly on diaphyseal bone after embedding the epiphyses in low-melting point agarose, which prevents the contamination of cell cultures with cells deriving from the growth plate or articular surface[60]. An alternative method to isolate murine PDC, proposed by Wang et al., employs a femoral bone grafting model[44]. The authors first performed a bone grafting surgery and 3 days later isolated the graft, scraped off the newly formed periosteal callus and performed an enzymatic digest to release periosteal cells. While the number of cells which can be obtained may be higher than those isolated from resting periosteum, this technique isolates cells which have been subjected to hypoxia and inflammation and are already in an active state, which can make the comparison with human PDC more difficult. However in the authors opinion, refined 12 microsurgery tools coupled to appropriate microscopy and “good” hands, should allow microdissection of the periosteum, even in adult mice. Regardless of differences in isolation method or species used, several features of the obtained periosteal cell populations are highly comparable between studies. In culture, PDC exhibit a fibroblast-like morphology, which is stably maintained over several passages. Culture-expanded PDC are negative for telomerase, but they do possess relatively long telomeres that may contribute to their stability in culture[61]. Furthermore, culture expansion of PDC appears to be STAT3 dependent as inhibition of this pathway, either through interference with JAK2 or STAT3 directly, abrogates proliferation induced by serum growth factors[62]. While PDC do not overtly express osteogenic or chondrogenic properties during expansion, they can be induced to differentiate along the osteogenic, chondrogenic and adipogenic lineage in vitro by subjecting them to specific differentiation conditions, confirming their multipotent nature[44, 57, 60, 61, 63]. Evidence for the presence of genuine skeletal stem cells in the periosteum has been delivered by single-cell lineage analysis, showing that the periosteum contains cells with mesenchymal multipotency (osteogenic, chondrogenic, adipogenic and myogenic) at the clonal level[61]. This concept is further underscored by the observation that expanded PDC possess the potential to form bone, cartilage and hematopoietic marrow upon in vivo transplantation[44, 60, 61, 64]. However, it is still unclear whether the skeletal progenitor cells in the periosteum also possess the potential to self-renew, a key feature of stem cell identity[65]. Characterization of PDC cultures by analysis of cell surface markers has shown that a high percentage of cells express the mesenchymal stem/progenitor cell markers CD73, CD90, CD105, CD146 and CD166 (humans) or CD51, CD73, CD90.2, CD105 13 and Sca1 (mice), while lacking the expression of markers associated with the hematopoietic and endothelial lineages[44, 60, 61, 64]. However, periosteal cell cultures have also been shown to contain preosteoblasts and committed osteogenic cells, underscoring the heterogeneous nature of the periosteum[54]. Although studies have been conducted with sorted CD45-CD9+CD90+CD166+ PDC, it is unclear whether this procedure of cell processing results in a pure population that represents all biological and functional characteristics of periosteal progenitors[66]. Indeed, there is currently a lack of specific markers for periosteal progenitors that allows their isolation from tissue digests. The ability of PDC to mobilize to fracture sites has prompted investigation into their ability to respond to chemokines. Subsequently, it has been reported that PDCs express chemokine receptors from the four chemokine subfamilies; CC, CXC, CX(3)C, and C. Furthermore, they are responsive to the chemokines CCL2 (monocyte chemoattractant protein-1, MCP1), CCL25 (thymus expressed chemokine, TECK), CXCL8 (interleukin 8, IL8), CXCL12 (SDF1α) and CXCL13 (B-cell-activating chemokine 1, BCA1)[67]. In addition, PDC respond to a number of growth factors and cytokines. Indeed, factors such as IL6, epidermal growth factor (EGF), TGFβ1 and BMP2 have been shown to play key roles in PDC osteogenic differentiation[68, 69]. Additionally, calcium- and phosphate-enriched culture conditions promote certain aspects of osteogenic differentiation in vitro, although this may be as a result of enhanced BMP2 expression[70, 71]. Although in vitro studies have clearly shown that the periosteum contains multipotent skeletal progenitor cells, their in vivo counterpart still remains elusive. However, recent lineage-tracing studies during fracture healing in mice have shed a first light on the markers that could be used to identify skeletal progenitor cells in the 14 periosteum in vivo. Grcevic et al. have used alpha smooth muscle actin(αSMA)CreERT2 transgenic mice to demonstrate that the majority of the cells in the fracture callus derive from perivascular αSMA-positive cells that presumably originate from the cambium layer of the periosteum [72]. Furthermore, when periosteal αSMApositive cells were isolated, they exhibited skeletal progenitor cell characteristics, including the expression of several mesenchymal progenitor cell markers and the ability to differentiate along the osteogenic, chondrogenic and adipogenic lineage[50, 72]. Following a similar approach with Prx1-CreER-GFP transgenic mice, Kawanami et al. showed that PRX1-expressing cells in the periosteum are osteochondroprogenitor cells that give rise to chondrocytes and osteoblasts in the fracture callus[73]. A recent study by Murao et al. further revealed that while no SOX9-positive cells are detected in resting periosteum, these cells quickly arise after bone fracture[74]. By tracing their progeny using Sox9-CreERT2 mice, the authors showed that these cells give rise to both chondrocytes and osteoblasts in the callus. How these different cell populations relate to one another, however, is currently unknown. The observation that periosteal progenitor cells express perivascular cell markers, including αSMA, CD146 and PDGF receptor beta[44, 50, 60, 61, 72], is in accordance with several studies that have shown a perivascular location for skeletal stem cells in bone marrow[75-77]. As the periosteum is highly vascularized and evidence exists that periosteal pericytes possess skeletal progenitor cell characteristics, this model could explain the high number of progenitors found in this tissue[39, 76, 78, 79]. The finding that PDC can enhance vasculogenesis by adapting a pericyte-like phenotype when they are implanted together with endothelial cells further supports this concept[60]. 15 Periosteum-derived cells in (pre)clinical bone tissue engineering approaches The feasibility of using periosteal cells for bone TE strategies was for the first time described by Nakahara et al. in 1991, who demonstrated in vivo bone formation by human PDC[80]. Since then, numerous studies have used PDC together with different scaffolds to enhance bone regeneration in critical-sized defects in a variety of animal models[56, 81-84]. The use of PDC together with a ceramic scaffold appears to represent an ideal combination as both natural and synthetic calcium phosphate carriers exhibit osteoinductive effects on PDC[37, 62, 85]. While the exact molecular mechanisms behind bone formation by PDC in TE transplants remain unknown, endogenous BMP and Wnt signaling in PDC have been shown to be crucial for their bone-forming potential on ceramic scaffolds, and exogenous addition of BMP2 can further enhance periosteal cell-driven bone regeneration[37, 86]. The central role of the periosteum in bone repair and the success of periosteal cells in preclinical animal models has also given rise to several exploratory clinical studies using ex vivo expanded periosteal cells for bone regeneration. The first of these studies was performed by Vacanti et al., who used culture-expanded periosteal cells derived from the radius in combination with a porous hydroxyapatite scaffold to replace the distal phalanx of the thumb of a 36-year-old man[87]. Although functional restoration was obtained, histological examination after 10 months revealed that only 5% of the construct was filled with lamellar bone and ossified endochondral tissue. Further studies using tissue engineered constructs containing expanded periosteal cells for maxillary sinus floor augmentation have however provided more compelling evidence that PDC can be used to regenerate substantial amounts of bone in 16 humans within 3-4 months after transplantation[88-90]. Taken together, these reports demonstrate the clinical potential of PDC for bone regeneration therapies. New, more extensive clinical trials will however be essential to provide irrefutable evidence for the efficacy of periosteal cells in different clinical applications. Periosteum-derived cells versus mesenchymal progenitor cells from other sources Although during postnatal fracture repair the tissue predominantly responsible for contributing tissue-forming progenitors is the periosteum, multiple adult progenitor cell populations can be induced into the osteogenic lineage in vitro, and hence their applicability for skeletal regeneration is being investigated. Consequently, it is important to define which of these cell populations are most suitable for this purpose, both for their ease of harvesting and their ability to contribute to tissue formation in vivo. A number of studies have attempted to directly compare mesenchymal progenitor populations from different tissues in a range of species including mouse, rat, pig, horse and human. The most commonly compared sources of mesenchymal progenitor cells are PDC, synovium-derived cells (SDC), bone marrow-derived mesenchymal stromal cells (BM-MSC), muscle-derived cells (MDC) and adipose tissue-derived cells (ADC). From these tissues it appears that the periosteum and synovium contain the highest quantity of stem/progenitor cells as they have the ability to produce a higher number of colonies when plated at low density[91, 92]. However, the large number of nucleated but non-adherent hematopoietic cells present in bone marrow aspirates may contribute to this finding. Cell surface markers appear to be similar in cells derived from each of the aforementioned tissues with only positivity for VEGFR-2 (Flk-1) being higher in PDC than in ADC and MDC[93]. However, this 17 analysis was carried out in passaged cells therefore it is conceivable that these cells have lost their tissue-specific profile during culture adaptation. When proliferative capacity of equine mesenchymal progenitors was compared, it was found that MDC, PDC and ADC proliferated significantly faster than BM-MSC[93]. Furthermore, in all published comparisons, PDC and SDC appeared to have the highest proliferative capacity when compared to BM-MSC across species, including rat[94], mouse[60] and human[92]. A high proliferative capacity is generally a prerequisite of cells intended for tissue engineering, as an in vitro cell expansion step usually forms part of this strategy. For analysis of in vitro differentiation capacity it should be noted that all mesenchymal progenitor cell populations, by definition, must have the ability to produce adipocytes, chondrocytes and osteoblasts[95]. However it is evident from comparative studies that cells isolated from specific tissues often have enhanced differentiation towards one of these lineages. Indeed, human PDC, BM-MSC and SDC display superior osteogenic differentiation when compared to MDC and ADC, however the authors did not speculate which of these three was the most osteogenic[92]. Indeed, studies that have specifically compared the osteogenic capacity of PDC, SDC and BM-MSC report conflicting data. For example, Hayashi et al. claim that rat BM-MSC have a higher osteogenic capacity when compared to PDC[91], while Yoshimura et al. report the opposite[94]. This contradiction may be explained by a number of technical differences between these studies including cell passage number and osteogenic conditions used. Interestingly, SDC reproducibly display the highest chondrogenic differentiation across species, followed by PDC[92, 94], indicating that in vitro differentiation capacity is in part reflected by the anatomical location of the parental tissue in vivo. 18 Limited studies have compared the efficacy of different cell populations for in vivo tissue formation. One study used an in vivo pig cranial defect model to compare the osteogenic potential of ADC, PDC and BM-MSC. In this study all the cell populations showed comparable osseous healing when implanted in a collagen scaffold and compared to an empty scaffold[96]. Our laboratory has previously compared the calcium phosphate-driven in vivo bone-forming capacity of human PDC, SDC, MDC (mesoangioblasts)[64] and BM-MSC (unpublished data) (Fig. 3). Using these assay conditions, including the use of specific scaffolds, only PDC and BM-MSC were able to form quantifiable bone spicules. Interestingly, BM-MSC formed larger hematopoietic compartments than PDC, thus providing further evidence for progenitor populations having tissue specific memory. 5. Tissue engineering strategies mimicking the periosteum in its absence The importance of periosteal integrity for fracture repair has led to the proposal of strategies to recreate this tissue for long bone repair. Indeed, this concept is currently being used clinically through the induction of a periosteal-like membrane in a technique proposed by Masquelet and colleagues[97]. This procedure involves the debridement of bone before implantation of a polymethyl methacrylate cement spacer within the fixated bone defect. The role of this spacer is to firstly provide mechanical support for the fracture, and secondly to act as a foreign body that allows the propagation of the periosteal like membrane on its surface. The membrane is highly vascularized and secretes a number of growth factors that are important in skeletal development and repair, such as BMP2, VEGF and TGFβ1[98]. This induced membrane enhances the repair of large long bone defects when combined with 19 cancellous autografts. Interestingly, it has recently been shown that the induced membrane contains progenitor cells which have the ability to undergo differentiation into chondrocytes, osteoblasts and adipocytes[99]. Upon comparison to PDC, the induced membrane-derived cells had a similar colony-forming and differentiation capacity; however they did express higher levels SDF1α, a protein that is known to be involved in the recruitment of progenitors to the site of injury. It is currently unclear what the origin of these progenitors is, however, the assumption that they may come from the periosteum is supported as induced membranes which were formed subcutaneously have no bone-forming capacity in conjunction with a calcium phosphate biomaterial[100]. In addition to this example of in situ tissue engineering, investigations are on-going that aim to produce an engineered periosteum in vitro[101]. It is proposed that growth factors and cells can be sequestered within hydrogels in a manner and at levels that mimic the native periosteum. The investigators envisage that this system will improve the healing and integration of allografts in vivo to levels that are seen with autografts. Engineered artificial periosteal tissues have previously been investigated, including the use of acellular human dermis as a substitute for periosteum for the repair of critical sized defects[102]. When this membrane was seeded with BMP2-expressing BM-MSC, it promoted heterotopic bone formation and could heal critical sized mandibular defects in mice. Although interesting, it is unclear whether this construct mimics the periosteum or simply provides a BMP2/cell delivery device. Indeed, it has also been documented that by seeding BMP2 modified cells directly onto an allograft, cartilaginous tissue and a new cortical shell was formed resulting in bridging of a segmental defect. However, this did not completely mimic an autograft as slower resorption of the graft was observed [103]. More recently it has been reported that 20 BM-MSC cell sheets can act as an engineered periosteum and promote bone callus formation during allograft healing[104], while PDC cell sheets may have applications in tendon-bone healing[105]. Evidently, the investigation of periosteum mimetics for skeletal regeneration and repair is gathering pace and further investigation is eagerly anticipated. 6. Concluding remarks and future directions As illustrated, it is clear that the periosteum plays an essential role in bone development, homeostasis and repair. As our insight into periosteal involvement in each of these processes grows, so does our ability to target it for skeletal regeneration. Indeed, during postnatal fracture repair the periosteum contributes the vast majority of progenitors for the cartilaginous callus and bone, in contrast to the bone marrow compartment, which appears to have only a minimal bone tissueforming potential. In cases where this repair mechanism fails, clinically described as delayed or non-union, the ability to specifically target periosteal stem cells in vivo would likely be a highly effective strategy. However, further characterization of the periosteal stem cell niche, including factors regulating stem cell quiescence and activation are required to make this possible. Furthermore, markers that robustly identify the resident periosteal stem cells in the cambium layer and allow their selection from the fibrous layer are urgently required. Current studies indicate that PRX1 expression may mark a population of progenitor cells, however it is not known whether this is the entire stem cell component or whether these cells are progeny of the periosteal stem cell. Once these factors have been determined, in vivo targeting of periosteal cells for skeletal repair will become a reality. In the meantime, the investigation of ex vivo-expanded PDC for tissue engineering strategies is ongoing. It 21 is envisaged that these studies, along with advances in periosteum mimetics, will lead to clinical translation of novel tissue engineered strategies for skeletal repair. In conclusion, it is the authors’ belief that with this review the uncertainty regarding which source of stem cells is most suited to skeletal regeneration has now been addressed, and we sincerely hope that this will invigorate more investigation into the periosteum in the future. Acknowledgements This work was funded by the ERC Advanced Grant REJOIND (294191-REJOIND), the BOF-KU Leuven GOA project (3M120209) and the Stem Cell Institute of LeuvenKU Leuven (PF/10/019). The work is part of Prometheus, the Leuven Research and Development Division of Skeletal Tissue http://www.kuleuven.be/Prometheus. 22 Engineering of KU Leuven: References [1] Duhamel HL. Sur le développement et la crue des os des animaux. Mem Acad Roy Sci Paris 1742:354-70. [2] Ollier L. Traite experimentel et clinique de la regeneration des os et de la production artificielle du tissu osseux. Paris: V. Masson; 1867. [3] Allen MR, Hock JM, Burr DB. Periosteum: biology, regulation, and response to osteoporosis therapies. Bone 2004;35:1003-12. [4] Chanavaz M. Anatomy and histophysiology of the periosteum: quantification of the periosteal blood supply to the adjacent bone with 85Sr and gamma spectrometry. J Oral Implantol 1995;21:214-9. [5] Colnot C. Skeletal cell fate decisions within periosteum and bone marrow during bone regeneration. J Bone Miner Res 2009;24:274-82. [6] Ozaki A, Tsunoda M, Kinoshita S, Saura R. Role of fracture hematoma and periosteum during fracture healing in rats: interaction of fracture hematoma and the periosteum in the initial step of the healing process. J Orthop Sci 2000;5:64-70. [7] Long F. Building strong bones: molecular regulation of the osteoblast lineage. Nat Rev Mol Cell Biol 2012;13:27-38. [8] Ochareon P, Herring SW. Cell replication in craniofacial periosteum: appositional vs. resorptive sites. J Anat 2011;218:285-97. [9] Kronenberg HM. Developmental regulation of the growth plate. Nature 2003;423:332-6. [10] Akiyama H, Chaboissier MC, Martin JF, Schedl A, de CB. The transcription factor Sox9 has essential roles in successive steps of the chondrocyte differentiation pathway and is required for expression of Sox5 and Sox6. Genes Dev 2002;16:2813-28. [11] Akiyama H, Kim JE, Nakashima K, Balmes G, Iwai N, Deng JM et al. Osteo-chondroprogenitor cells are derived from Sox9 expressing precursors. Proc Natl Acad Sci U S A 2005;102:14665-70. [12] Chung UI, Schipani E, McMahon AP, Kronenberg HM. Indian hedgehog couples chondrogenesis to osteogenesis in endochondral bone development. J Clin Invest 2001;107:295-304. 23 [13] Ornitz DM, Marie PJ. FGF signaling pathways in endochondral and intramembranous bone development and human genetic disease. Genes Dev 2002;16:1446-65. [14] Pathi S, Rutenberg JB, Johnson RL, Vortkamp A. Interaction of Ihh and BMP/Noggin signaling during cartilage differentiation. Dev Biol 1999;209:239-53. [15] Maes C, Kobayashi T, Selig MK, Torrekens S, Roth SI, Mackem S et al. Osteoblast precursors, but not mature osteoblasts, move into developing and fractured bones along with invading blood vessels. Dev Cell 2010;19:329-44. [16] Seeman E. Periosteal bone formation - a neglected determinant of bone strength. N Engl J Med 2003;349:320-3. [17] Orwoll ES. Toward an expanded understanding of the role of the periosteum in skeletal health. J Bone Miner Res 2003;18:949-54. [18] Callewaert F, Sinnesael M, Gielen E, Boonen S, Vanderschueren D. Skeletal sexual dimorphism: relative contribution of sex steroids, GH-IGF1, and mechanical loading. J Endocrinol 2010;207:127-34. [19] Almeida M, Iyer S, Martin-Millan M, Bartell SM, Han L, Ambrogini E et al. Estrogen receptoralpha signaling in osteoblast progenitors stimulates cortical bone accrual. J Clin Invest 2012;123:394-404. [20] Ogita M, Rached MT, Dworakowski E, Bilezikian JP, Kousteni S. Differentiation and proliferation of periosteal osteoblast progenitors are differentially regulated by estrogens and intermittent parathyroid hormone administration. Endocrinology 2008;149:5713-23. [21] Orwoll ES. Androgens: basic biology and clinical implication. Calcif Tissue Int 2001;69:185-8. [22] Marsell R, Einhorn TA. The biology of fracture healing. Injury 2011;42:551-5. [23] Al-Aql ZS, Alagl AS, Graves DT, Gerstenfeld LC, Einhorn TA. Molecular mechanisms controlling bone formation during fracture healing and distraction osteogenesis. J Dent Res 2008;87:107-18. [24] Barnes GL, Kostenuik PJ, Gerstenfeld LC, Einhorn TA. Growth factor regulation of fracture repair. J Bone Miner Res 1999;14:1805-15. [25] Cho TJ, Gerstenfeld LC, Einhorn TA. Differential temporal expression of members of the transforming growth factor beta superfamily during murine fracture healing. J Bone Miner Res 2002;17:513-20. 24 [26] Schmid GJ, Kobayashi C, Sandell LJ, Ornitz DM. Fibroblast growth factor expression during skeletal fracture healing in mice. Dev Dyn 2009;238:766-74. [27] Yu YY, Lieu S, Lu C, Miclau T, Marcucio RS, Colnot C. Immunolocalization of BMPs, BMP antagonists, receptors, and effectors during fracture repair. Bone 2010;46:841-51. [28] Thompson Z, Miclau T, Hu D, Helms JA. A model for intramembranous ossification during fracture healing. J Orthop Res 2002;20:1091-8. [29] Marsh DR, Li G. The biology of fracture healing: optimising outcome. Br Med Bull 1999;55:856-69. [30] Zhang X, Xie C, Lin AS, Ito H, Awad H, Lieberman JR et al. Periosteal progenitor cell fate in segmental cortical bone graft transplantations: implications for functional tissue engineering. J Bone Miner Res 2005;20:2124-37. [31] van Gastel N, Stegen S, Stockmans I, Moermans K, Schrooten J, Graf D et al. Expansion of murine periosteal progenitor cells with FGF2 reveals an intrinsic endochondral ossification program mediated by BMP2. Stem Cells 2014;10.1002/stem.1783 [doi]. [32] Tsuji K, Cox K, Bandyopadhyay A, Harfe BD, Tabin CJ, Rosen V. BMP4 is dispensable for skeletogenesis and fracture-healing in the limb. J Bone Joint Surg Am 2008;90:14-8. [33] Tsuji K, Cox K, Gamer L, Graf D, Economides A, Rosen V. Conditional deletion of BMP7 from the limb skeleton does not affect bone formation or fracture repair. J Orthop Res 2010;28:3849. [34] Tsuji K, Bandyopadhyay A, Harfe BD, Cox K, Kakar S, Gerstenfeld L et al. BMP2 activity, although dispensable for bone formation, is required for the initiation of fracture healing. Nat Genet 2006;38:1424-9. [35] Chappuis V, Gamer L, Cox K, Lowery JW, Bosshardt DD, Rosen V. Periosteal BMP2 activity drives bone graft healing. Bone 2012;51:800-9. [36] Wang Q, Huang C, Xue M, Zhang X. Expression of endogenous BMP-2 in periosteal progenitor cells is essential for bone healing. Bone 2011;48:524-32. [37] Eyckmans J, Roberts SJ, Schrooten J, Luyten FP. A clinically relevant model of osteoinduction: a process requiring calcium phosphate and BMP/Wnt signalling. J Cell Mol Med 2010;14:1845-56. 25 [38] Behr B, Leucht P, Longaker MT, Quarto N. Fgf-9 is required for angiogenesis and osteogenesis in long bone repair. Proc Natl Acad Sci U S A 2010;107:11853-8. [39] Coutu DL, Francois M, Galipeau J. Inhibition of cellular senescence by developmentally regulated FGF receptors in mesenchymal stem cells. Blood 2011;117:6801-12. [40] Rundle CH, Miyakoshi N, Ramirez E, Wergedal JE, Lau KH, Baylink DJ. Expression of the fibroblast growth factor receptor genes in fracture repair. Clin Orthop Relat Res 2002:253-63. [41] Du X, Xie Y, Xian CJ, Chen L. Role of FGFs/FGFRs in skeletal development and bone regeneration. J Cell Physiol 2012;227:3731-43. [42] Le AX, Miclau T, Hu D, Helms JA. Molecular aspects of healing in stabilized and nonstabilized fractures. J Orthop Res 2001;19:78-84. [43] Murakami S, Noda M. Expression of Indian hedgehog during fracture healing in adult rat femora. Calcif Tissue Int 2000;66:272-6. [44] Wang Q, Huang C, Zeng F, Xue M, Zhang X. Activation of the Hh pathway in periosteumderived mesenchymal stem cells induces bone formation in vivo: implication for postnatal bone repair. Am J Pathol 2010;177:3100-11. [45] Huang C, Tang M, Yehling E, Zhang X. Overexpressing Sonic Hedgehog Peptide Restores Periosteal Bone Formation in a Murine Bone Allograft Transplantation Model. Mol Ther 2014;22:430-9. [46] Gerstenfeld LC, Cho TJ, Kon T, Aizawa T, Tsay A, Fitch J et al. Impaired fracture healing in the absence of TNF-alpha signaling: the role of TNF-alpha in endochondral cartilage resorption. J Bone Miner Res 2003;18:1584-92. [47] Xie C, Ming X, Wang Q, Schwarz EM, Guldberg RE, O'Keefe RJ et al. COX-2 from the injury milieu is critical for the initiation of periosteal progenitor cell mediated bone healing. Bone 2008;43:1075-83. [48] Zhang X, Schwarz EM, Young DA, Puzas JE, Rosier RN, O'Keefe RJ. Cyclooxygenase-2 regulates mesenchymal cell differentiation into the osteoblast lineage and is critically involved in bone repair. J Clin Invest 2002;109:1405-15. [49] Hilton MJ, Tu X, Wu X, Bai S, Zhao H, Kobayashi T et al. Notch signaling maintains bone marrow mesenchymal progenitors by suppressing osteoblast differentiation. Nat Med 2008;14:306-14. 26 [50] Matthews BG, Grcevic D, Wang L, Hagiwara Y, Roguljic H, Joshi P et al. Analysis of alphaSMA-Labeled Progenitor Cell Commitment Identifies Notch Signaling as an Important Pathway in Fracture Healing. J Bone Miner Res 2013. [51] Komatsu DE, Mary MN, Schroeder RJ, Robling AG, Turner CH, Warden SJ. Modulation of Wnt signaling influences fracture repair. J Orthop Res 2010;28:928-36. [52] Minear S, Leucht P, Jiang J, Liu B, Zeng A, Fuerer C et al. Wnt proteins promote bone regeneration. Sci Transl Med 2010;2:29ra30. [53] Baron R, Kneissel M. WNT signaling in bone homeostasis and disease: from human mutations to treatments. Nat Med 2013;19:179-92. [54] Chang H, Knothe Tate ML. Concise review: the periosteum: tapping into a reservoir of clinically useful progenitor cells. Stem Cells Transl Med 2012;1:480-91. [55] Arnsdorf EJ, Jones LM, Carter DR, Jacobs CR. The periosteum as a cellular source for functional tissue engineering. Tissue Eng Part A 2009;15:2637-42. [56] Breitbart AS, Grande DA, Kessler R, Ryaby JT, Fitzsimmons RJ, Grant RT. Tissue engineered bone repair of calvarial defects using cultured periosteal cells. Plast Reconstr Surg 1998;101:567-74. [57] Declercq HA, De Ridder LI, Cornelissen MJ. Isolation and Osteogenic Differentiation of Rat Periosteum-derived Cells. Cytotechnology 2005;49:39-50. [58] Eyckmans J, Luyten FP. Species specificity of ectopic bone formation using periosteumderived mesenchymal progenitor cells. Tissue Eng 2006;12:2203-13. [59] Nakahara H, Bruder SP, Goldberg VM, Caplan AI. In vivo osteochondrogenic potential of cultured cells derived from the periosteum. Clin Orthop Relat Res 1990;259:223-32. [60] van Gastel N, Torrekens S, Roberts SJ, Moermans K, Schrooten J, Carmeliet P et al. Engineering vascularized bone: osteogenic and proangiogenic potential of murine periosteal cells. Stem Cells 2012;30:2460-71. [61] De Bari C, Dell'Accio F, Vanlauwe J, Eyckmans J, Khan IM, Archer CW et al. Mesenchymal multipotency of adult human periosteal cells demonstrated by single-cell lineage analysis. Arthritis Rheum 2006;54:1209-21. 27 [62] Roberts SJ, Owen HC, Tam WL, Solie L, Van Cromphaut SJ, Van den Berghe G et al. Humanized Culture of Periosteal Progenitors in Allogeneic Serum Enhances Osteogenic Differentiation and In Vivo Bone Formation. Stem Cells Transl Med 2013. [63] Nakahara H, Dennis JE, Bruder SP, Haynesworth SE, Lennon DP, Caplan AI. In vitro differentiation of bone and hypertrophic cartilage from periosteal-derived cells. Exp Cell Res 1991;195:492-503. [64] Roberts SJ, Geris L, Kerckhofs G, Desmet E, Schrooten J, Luyten FP. The combined bone forming capacity of human periosteal derived cells and calcium phosphates. Biomaterials 2011;32:4393-405. [65] Bianco P, Cao X, Frenette PS, Mao JJ, Robey PG, Simmons PJ et al. The meaning, the sense and the significance: translating the science of mesenchymal stem cells into medicine. Nat Med 2013;19:35-42. [66] Lim SM, Choi YS, Shin HC, Lee CW, Kim DI. Isolation of human periosteum-derived progenitor cells using immunophenotypes for chondrogenesis. Biotechnol Lett 2005;27:60711. [67] Stich S, Loch A, Leinhase I, Neumann K, Kaps C, Sittinger M et al. Human periosteumderived progenitor cells express distinct chemokine receptors and migrate upon stimulation with CCL2, CCL25, CXCL8, CXCL12, and CXCL13. Eur J Cell Biol 2008;87:365-76. [68] Eyckmans J, Roberts SJ, Bolander J, Schrooten J, Chen CS, Luyten FP. Mapping calcium phosphate activated gene networks as a strategy for targeted osteoinduction of human progenitors. Biomaterials 2013;34:4612-21. [69] Roberts SJ, Chen Y, Moesen M, Schrooten J, Luyten FP. Enhancement of osteogenic gene expression for the differentiation of human periosteal derived cells. Stem Cell Res 2011;7:13744. [70] Chai YC, Roberts SJ, Schrooten J, Luyten FP. Probing the osteoinductive effect of calcium phosphate by using an in vitro biomimetic model. Tissue Eng Part A 2011;17:1083-97. [71] Chai YC, Roberts SJ, Desmet E, Kerckhofs G, van GN, Geris L et al. Mechanisms of ectopic bone formation by human osteoprogenitor cells on CaP biomaterial carriers. Biomaterials 2012;33:3127-42. 28 [72] Grcevic D, Pejda S, Matthews BG, Repic D, Wang L, Li H et al. In vivo fate mapping identifies mesenchymal progenitor cells. Stem Cells 2012;30:187-96. [73] Kawanami A, Matsushita T, Chan YY, Murakami S. Mice expressing GFP and CreER in osteochondro progenitor cells in the periosteum. Biochem Biophys Res Commun 2009;386:477-82. [74] Murao H, Yamamoto K, Matsuda S, Akiyama H. Periosteal cells are a major source of soft callus in bone fracture. J Bone Miner Metab 2013;31:390-8. [75] Mendez-Ferrer S, Michurina TV, Ferraro F, Mazloom AR, Macarthur BD, Lira SA et al. Mesenchymal and haematopoietic stem cells form a unique bone marrow niche. Nature 2010;466:829-34. [76] Park D, Spencer JA, Koh BI, Kobayashi T, Fujisaki J, Clemens TL et al. Endogenous bone marrow MSCs are dynamic, fate-restricted participants in bone maintenance and regeneration. Cell Stem Cell 2012;10:259-72. [77] Sacchetti B, Funari A, Michienzi S, Di Cesare S, Piersanti S, Saggio I et al. Self-renewing osteoprogenitors in bone marrow sinusoids can organize a hematopoietic microenvironment. Cell 2007;131:324-36. [78] Diaz-Flores L, Gutierrez R, Lopez-Alonso A, Gonzalez R, Varela H. Pericytes as a supplementary source of osteoblasts in periosteal osteogenesis. Clin Orthop Relat Res 1992:280-6. [79] Simpson AH. The blood supply of the periosteum. J Anat 1985;140:697-704. [80] Nakahara H, Goldberg VM, Caplan AI. Culture-expanded human periosteal-derived cells exhibit osteochondral potential in vivo. J Orthop Res 1991;9:465-76. [81] Bakker AD, Schrooten J, van Cleynenbreugel T, Vanlauwe J, Luyten J, Schepers E et al. Quantitative screening of engineered implants in a long bone defect model in rabbits. Tissue Eng Part C Methods 2008;14:251-60. [82] Perka C, Schultz O, Spitzer RS, Lindenhayn K, Burmester GR, Sittinger M. Segmental bone repair by tissue-engineered periosteal cell transplants with bioresorbable fleece and fibrin scaffolds in rabbits. Biomaterials 2000;21:1145-53. 29 [83] Redlich A, Perka C, Schultz O, Spitzer R, Haupl T, Burmester GR et al. Bone engineering on the basis of periosteal cells cultured in polymer fleeces. J Mater Sci Mater Med 1999;10:76772. [84] Sakata Y, Ueno T, Kagawa T, Kanou M, Fujii T, Yamachika E et al. Osteogenic potential of cultured human periosteum-derived cells - a pilot study of human cell transplantation into a rat calvarial defect model. J Craniomaxillofac Surg 2006;34:461-5. [85] Srouji S, Ben-David D, Funari A, Riminucci M, Bianco P. Evaluation of the osteoconductive potential of bone substitutes embedded with schneiderian membrane- or maxillary bone marrow-derived osteoprogenitor cells. Clin Oral Implants Res 2013;24:1288-94. [86] Agata H, Asahina I, Yamazaki Y, Uchida M, Shinohara Y, Honda MJ et al. Effective bone engineering with periosteum-derived cells. J Dent Res 2007;86:79-83. [87] Vacanti CA, Bonassar LJ, Vacanti MP, Shufflebarger J. Replacement of an avulsed phalanx with tissue-engineered bone. N Engl J Med 2001;344:1511-4. [88] Schimming R, Schmelzeisen R. Tissue-engineered bone for maxillary sinus augmentation. J Oral Maxillofac Surg 2004;62:724-9. [89] Schmelzeisen R, Schimming R, Sittinger M. Making bone: implant insertion into tissueengineered bone for maxillary sinus floor augmentation-a preliminary report. J Craniomaxillofac Surg 2003;31:34-9. [90] Springer IN, Nocini PF, Schlegel KA, De SD, Park J, Warnke PH et al. Two techniques for the preparation of cell-scaffold constructs suitable for sinus augmentation: steps into clinical application. Tissue Eng 2006;12:2649-56. [91] Hayashi O, Katsube Y, Hirose M, Ohgushi H, Ito H. Comparison of osteogenic ability of rat mesenchymal stem cells from bone marrow, periosteum, and adipose tissue. Calcif Tissue Int 2008;82:238-47. [92] Sakaguchi Y, Sekiya I, Yagishita K, Muneta T. Comparison of human stem cells derived from various mesenchymal tissues: superiority of synovium as a cell source. Arthritis Rheum 2005;52:2521-9. [93] Radtke CL, Nino-Fong R, Esparza Gonzalez BP, Stryhn H, McDuffee LA. Characterization and osteogenic potential of equine muscle tissue- and periosteal tissue-derived mesenchymal 30 stem cells in comparison with bone marrow- and adipose tissue-derived mesenchymal stem cells. Am J Vet Res 2013;74:790-800. [94] Yoshimura H, Muneta T, Nimura A, Yokoyama A, Koga H, Sekiya I. Comparison of rat mesenchymal stem cells derived from bone marrow, synovium, periosteum, adipose tissue, and muscle. Cell Tissue Res 2007;327:449-62. [95] Dominici M, Le BK, Mueller I, Slaper-Cortenbach I, Marini F, Krause D et al. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006;8:315-7. [96] Stockmann P, Park J, von WC, Nkenke E, Felszeghy E, Dehner JF et al. Guided bone regeneration in pig calvarial bone defects using autologous mesenchymal stem/progenitor cells - a comparison of different tissue sources. J Craniomaxillofac Surg 2012;40:310-20. [97] Pelissier P, Martin D, Baudet J, Lepreux S, Masquelet AC. Behaviour of cancellous bone graft placed in induced membranes. Br J Plast Surg 2002;55:596-8. [98] Pelissier P, Masquelet AC, Bareille R, Pelissier SM, Amedee J. Induced membranes secrete growth factors including vascular and osteoinductive factors and could stimulate bone regeneration. J Orthop Res 2004;22:73-9. [99] Cuthbert RJ, Churchman SM, Tan HB, McGonagle D, Jones E, Giannoudis PV. Induced periosteum a complex cellular scaffold for the treatment of large bone defects. Bone 2013;57:484-92. [100] Catros S, Zwetyenga N, Bareille R, Brouillaud B, Renard M, Amedee J et al. Subcutaneousinduced membranes have no osteoinductive effect on macroporous HA-TCP in vivo. J Orthop Res 2009;27:155-61. [101] Hoffman MD, Benoit DS. Emerging ideas: Engineering the periosteum: revitalizing allografts by mimicking autograft healing. Clin Orthop Relat Res 2013;471:721-6. [102] Schonmeyr B, Clavin N, Avraham T, Longo V, Mehrara BJ. Synthesis of a tissue-engineered periosteum with acellular dermal matrix and cultured mesenchymal stem cells. Tissue Eng Part A 2009;15:1833-41. [103] Xie C, Reynolds D, Awad H, Rubery PT, Pelled G, Gazit D et al. Structural bone allograft combined with genetically engineered mesenchymal stem cells as a novel platform for bone tissue engineering. Tissue Eng 2007;13:435-45. 31 [104] Long T, Zhu Z, Awad HA, Schwarz EM, Hilton MJ, Dong Y. The effect of mesenchymal stem cell sheets on structural allograft healing of critical sized femoral defects in mice. Biomaterials 2014;35:2752-9. [105] Chang CH, Chen CH, Liu HW, Whu SW, Chen SH, Tsai CL et al. Bioengineered periosteal progenitor cell sheets to enhance tendon-bone healing in a bone tunnel. Biomed J 2012;35:473-80. 32 Figure Legends Figure 1. Histological analysis of the periosteum. H&E stained section of human fibular bone showing cortical bone with periosteum. The periosteum can be divided into an outer fibrous layer and an inner cambium layer, which is highly cellular and contains numerous blood vessels (arrows). Scale bar = 100µm. Figure 2. The different phases of fracture healing. Stage I: The physical disruption of the bone, blood vessels, and surrounding soft tissue causes the formation of a hematoma, associated with inflammation and hypoxia. Stage II: Growth factors present in the hematoma stimulate the proliferation of skeletal progenitor cells in the periosteum. Stage III: Progenitor cells differentiate into chondrocytes and osteoblasts, forming a soft callus that consists mainly of cartilage and woven bone. Stage IV: The initial woven bone is remodeled into mature lamellar bone by the cooperative action of osteoblasts and osteoclasts, gradually restoring the original shape of the bone. Figure 3. In vivo bone-forming capacity of human mesenchymal progenitor cells on calcium phosphate (CaP) scaffolds. (A-D) H&E staining of NuOss™ implants seeded with 1x106 periosteum-derived cells (PDC; A; [63]), bone marrowderived mesenchymal stromal cells (BM-MSC; B; unpublished data), muscle-derived cells (MDC; C; [63]) and synovium-derived cells (SDC; D; [63]), retrieved eight weeks after implantation. Bone formation (white arrows) was observed in PDC and BM-MSC implantations. Small (unquantifiable) bone spicules were observed with MDC (white arrow). Cell condensations (areas of increased cell density; black arrows) were observed next to CaP granules with SDC implantation. Hematopoietic compartments (white stars) were identifiable in both PDC and BM-MSC implants, however in larger quantities in the latter. Scale bars = 200µm. (E) Bone quantification of implants indicating the quantification of individual donors (black points) and mean (grey bar). Note variability in bone formation for PDC donors indicating that factors such as age and genetic background may play a role in the efficacy of the system. 33