(MS Word) (728 KB, doc) - Health Quality & Safety Commission
 (728 KB, doc) - Health Quality & Safety Commission")
PERFORMANCE IMPROVEMENT FRAMEWORK
Self-review of the
Health Quality & Safety Commission
1
September 2015
2
CONTENTS
SELF-REVIEW OF THE HEALTH QUALITY & SAFETY COMMISSION (HQSC) – SEPTEMBER 2015
INTRODUCTION: THE SELF-REVIEW PROCESS
3
The Minister of Health’s 2014/15 and 2015/16 Letters of Expectations noted that all health crown entities need to be constantly looking for ways to improve how they do their business and deliver value for the taxpayers’ investment in them. The Minister noted that the State Services
Commission’s (SSC) Performance Improvement Framework (PIF) was designed to do this and encouraged entities to use this PIF self-review methodology.
In November 2014, the Board and Senior Leadership Team approved draft terms of reference for a
PIF self-review. Initially the review was to be completed in July 2015, but was delayed to take account of the review of central agencies and refresh of the New Zealand Health Strategy.
The purpose of the review was to highlight ways we can improve the way we do our business and deliver value for taxpayers’ investment. The SSC is clear that this should not be seen as an audit, scientific evaluation, investigation of compliance or an accreditation process. Instead it is designed to form an integral part of an organisational continuous improvement programme.
The self-review had three main elements:
identifying the contribution that New Zealand needs from the Commission in the medium term
(a four year excellence horizon)
identifying any resulting changes to our strategy, role and the way we do our business that are needed to achieve the four year excellence horizon.
a generic review of those areas that the Commission needs to focus on or improve (from an organisational perspective) to ensure that it can continue to deliver results over time
As recommended by the SSC, the Commission engaged two external advisors to provide advice on the direction of the self-review and an independent perspective on the interim findings and final report. This has helped the Commission get the best out of the review and provide an addition level of assurance that the report is robust and fair. Dr Karen Poutasi, Chief Executive of NZQA and Debbie
Francis, who has completed numerous PIF reviews for the SSC, agreed to take on this role.
The external reviewers developed the high level four year excellence horizon through interviews with the Board, SLT, external agencies, SLT, and two focus group interviews with staff.
The review of the organisational management and results sections of the PIF framework was undertaken by an internal review team, Dr Iwona Stolarek (Medical Advisor), Carmela Petagna,
Senior Portfolio Manager, Deon York, Programme Manager – Patient Safety Campaign and Catherine
Gerard, Senior Analyst, Measurement & Evaluation.
The internal review team were responsible for the ratings and the recommendations in the report.
These were reviewed by the external advisors.
The Agency response is the Board and senior management response to this report and the recommendations.
SECTION A
HQSC response to the report and recommendations
4 SELF-REVIEW OF THE HEALTH QUALITY & SAFETY COMMISSION (HQSC) – SEPTEMBER 2015
5
COMMISSION RESPONSE TO THE REPORT AND
RECOMMENDATIONS
The Commission has found the PIF process and the insights to guide the next four years very helpful. We were pleased to hear the universally positive response from stakeholders and staff about the way we work and our achievements to date. We appreciate the informed and robust discussion that has taken place and the stimulus it has provided for improvement, both in relation to our focus over the next four years, and how we work internally.
Future focus
We agree with the views of stakeholders and staff that the Commission is at an ‘inflexion point’ in its development. Recognising this, the Board and SLT have been refreshing and reworking the Commission’s existing strategy over the past year, but were waiting for the findings and suggestions from this PIF process to further refine our thinking. So we are well on the way and plan to have a strategy for final review by February 2016 with a view to finalising it in March.
There is a strong base to work from. The Board and management were very pleased with the high rating for vision and purpose - and that staff so clearly understood and were able to articulate their roles in making the system safer (reducing harm and cost), improving quality and the experience of consumers and setting the direction for patient safety. Our task now is to clearly articulate our strategies for achieving this purpose, and to address the key strategic challenges raised by the external reviewers. These challenges include clarity about our ‘long-term system role’, a tighter system of prioritisation of activity/investment of effort and improved measurement and evaluation of impact. In addition, the Commission has also identified improving equity as a specific strategic challenge.
The strategy will provide clarity about what we plan to achieve in the next four years and what success will look like. The purpose of the Commission, articulated in the NZ Triple Aim, is to improve quality, safety and patient experience of care, improve health and equity for all populations and achieve best value for the public health care system. To help achieve these,
Government has set several strategic priorities for the Commission. These include playing an active role in working cooperatively with other agencies to support clinical leadership, build sector capability, improve patient experience and collect patient safety data and put it to its best use. They also include demonstrating the difference that we make.
Our work over the past year on reworking our existing strategy has more clearly identified some of the key principles that need to underpin the achievement of our purpose and strategy:
consumers being at the centre of the system – driving both the Commisison and the health sector
working hand in hand with stakeholders
‘being at the table’ at both at Ministerial and central agency level to contribute to strategic discussions, engendering a renewed sense of urgency for change
proactively using our information and knowledge as a catalyst for change
being relevant and adding value.
Internal focus
While staff considered the Commission to be a very positive workplace, with many opportunities to develop, the PIF review has provided valuable feedback on some areas for improvement. This is particularly important in the context of our reworked business model which we implemented over the last year. This has involved bringing previously outsourced functions in-house with a doubling of staff (including a significant increase in the number of improvement advisors and project managers). Not only does this mean that many staff have been with the Commission for less than a year, but also that previous internal systems and processes which were appropriate for a smaller organisation, are now under strain.
The key operational management areas we will focus on over the next year are:
more active orientation of new (and existing staff) which includes providing a clear understanding of: o the role of a Crown entity, how it differs from a government department and the private or NGO sector, the roles of governance and management and the relationship with Ministers. With so many new staff, many of whom have not work in the Crown entity environment before, this is particulalry important to ensure that the respective roles and responsibilities are understood. o the role of SLT, how it is made up (mixture of experts and management) and how it works, makes decisions and communicates.
re-developing our values
more formalised internal communication
refreshing our stakeholder engagement strategy
training and support for managers, particularly around providing feedback and managing performance
6 SELF-REVIEW OF THE HEALTH QUALITY & SAFETY COMMISSION (HQSC) – SEPTEMBER 2015
7
reviewing our internal budgeting and resources allocation processes.
Some of these are already in train. We have held a full day workshop for all staff on our values and have a second planned to finalise them. ‘Management toolbox’ sessions have commenced which include modules in areas such as recruitement, orientation of new staff and performance management. There are now also more extensive report-backs to staff after Board meetings.
We are planning a follow up PIF self-review in around 18 months to assess our progress and to identify further areas for improvement.
Professor Alan Merry, ONZM FRSNZ
Chair
Dr Janice Wilson
Chief Executive
SECTION B
Performance Improvement Framework
Report
Four year excellence horizon – Debbie Francis and
Karen Poutasi
Organisational management review – internal review team
8 SELF-REVIEW OF THE HEALTH QUALITY & SAFETY COMMISSION (HQSC) – SEPTEMBER 2015
FOUR YEAR EXCELLENCE HORIZON
To inform this section the external advisors, Debbie Francis and Dr Karen Poutasi asked external stakeholders and two staff focus groups: “What is the contribution New Zealand needs from the HQSC, and therefore what is the performance challenge? And if the HQSC is to be successful in meeting the challenge over the next four years, what would success look
like?” In their own words, this is what they found.
Environment
The Health Quality and Safety Commission (the Commission) is a small Crown entity operating within the complex landscape of the health system. Established in late 2010, its mission is to improve quality and safety across the across the health and disability sector, including reducing deaths, harm and waste from preventable errors in the health and disability system. It fulfils this mission by promoting a culture of continuous examination and quality improvement, coordinating quality interventions at a national level and promoting strong clinical engagement in quality and patient safety.
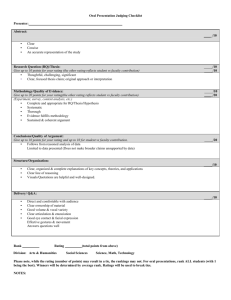
Given this mission, the Commission sits at the nexus of increasing customer expectation for quality care and the fiscal pressures facing our health system. Quality improvement is about getting better value from New Zealand’s healthcare spend as well as spending money on the right things, as reflected in the “Triple Aim” outcomes framework the Commission has set for itself below.
9
‘Doing the right thing, and doing it right, first time’
Thus the Commission undertakes simultaneous activity across the system in three dimensions:
Improved quality, safety and patient experience of care
Improved health and equity for all populations
Best value for the public health care system
Like all crown entities the Commission is guided by its annual letter of expectations from its
Minister. Specifically, the outputs the Commission is funded to deliver across these dimensions are:
1.
The provision of information, analysis and advice: Used wisely, measurement and reporting on quality and safety engages clinicians, managers and patients, and generates informed discussion and debate, which in turn should lift both efficiency and effectiveness.
2.
The provision of expert advice and informed comment – being an ‘intelligent’ commentator
3.
Tools and support for priority programmes: The Commission identifies and promotes examples of good practice across the system, and provides expert advice to the system.
4.
Sector and consumer capability: here the Commission is focussed on building the numbers of sector players with quality improvement capability and facilitating partnerships between providers and consumers.
These are bold ambitions for a small “independent” agency with an annual baseline of around $13.5 million and some 50 FTE staff. All of these outputs require system level leadership through light touch influence rather than through funding, policy instruments or other forms of hard power.
Although a young agency, the Commission is making measurable progress towards quality improvement across the three dimensions of individual, populations and system and all output areas. Notable achievements have included, inter alia:
The sustained near eradication of central line bacteraemia infections (CLAB) in intensive care units, with consequential avoided costs
Reductions in bed days in hospital associated with reduced perioperative harm
Reduction in serious harm from in-hospital falls
Reductions in rates of sudden unexpected death in infancy (SUID)
10 SELF-REVIEW OF THE HEALTH QUALITY & SAFETY COMMISSION (HQSC) – SEPTEMBER 2015
Improved reporting and review of adverse events in hospitals
Production of the Atlas of Healthcare Variation, which shows geographic variations in health care services and outcomes, designed to prompt debate amongst users and showcase best practice
Increased co design of services with customers and providers
Increasing numbers of improvement advisors in the sector
To date, most of the Commission’s effort has been deliberately focussed on the hospital sector, but delivery of outputs and outcomes requires connectedness with most parts of the health and disability system: from the Ministry and DHBs through, to the range of providers and peak bodies.
The Performance Challenge
This review was unusual in that all interviewees (no matter where they sat in the system), were universally positive about the work of the Commission to date. While most saw its early stage development as an object lesson in effective system leadership, they also believed the Commission was now positioned for a step change in value add.
Most believed that the Commission was at an inflexion point in its development and suggested that the things that had got it this far would not necessarily be the things that got it to the next level of performance.
There was no doubt amongst respondents with regard to the need for a quality body in the health and disability system. Respondents felt that should the Commission not continue to shine a light on quality improvement, such activity could be crowded out by business as usual, particularly in the DHB sector.
A consistent message was that the essence of the performance challenge now facing the
Commission was “how to make it matter more” in the wider system. Interviewees felt the
Commission had now earned widespread trust and respect, which gave it a right to lead, and to lead more assertively. There is less need to be reactive and sustainable strategy and implementation frameworks will be more important.
The heart of the performance challenge then, is the need to balance this impressive earned leadership with the slender resources available to the Commission.
We see five specific strategic challenges in this regard.
11
The first and most critical, is to gain greater clarity with respect to the Commission’s stewardship role in the system. Existential musings about whether it should exist or not as a separate entity have distracted it over the four years of its existence.
We asked respondents to provide us with a metaphor to describe this long-term role of the
Commission. These were mixed, as shown below:
A beacon
The conscience of the sector
An umbrella sheltering patients and end users
A mirror held to the system to help it see itself
An engine for driving change
The place you to benchmark yourself “like the Xero of the healthcare world”
A protective roadside barrier
A catalyst
A repository for best practice
Guerrilla evangelists
A fire starter
A matchmaker, broker or connector
A cuddly uncle
Yoda like
This system role needs to be surfaced more explicitly if it is to guide strategy and results over the next phase of the Commission’s existence. This should be done inclusively, with input from staff, other system players and end users.
The second strategic challenge is strategy itself. The Commission must further clarify its medium term purpose, vision and strategy. While respondents viewed the Commission positively they were unable to articulate its strategy. External stakeholders felt that what success looked like and how it should be measured was unclear. Staff felt the Commission was managing issues and events rather than building a strong institution for the future.
The third challenge the Commission faces is to develop a tighter system of prioritisation of activity and investment of effort. As it moves beyond the hospital sector and into the primary care to take a system view of quality (a move endorsed by stakeholders), the
Commission will need to be explicit and laser like in its focus if it is to apply its few resources to best effect. This is a highly fragmented system. The Commission’s prioritisation needs to be very explicit, both internally and within the sector. The risk of dilution of the
Commission’s effect is very high.
12 SELF-REVIEW OF THE HEALTH QUALITY & SAFETY COMMISSION (HQSC) – SEPTEMBER 2015
The fourth challenge relates to improved measurement and evaluation of impact.
Attribution is difficult and while the Commission has been working hard on improved output and outcome metrics, it needs to continue to lift the game in articulating both the quantitative and qualitative benefits it provides to the system.
The fifth challenge is more nuanced and relates to the future tone and operating style of the
Commission. There was difference of view on this. Many respondents talked about the
Commission having now earned the respect of the system to the extent it could afford to be a bit less ‘nice’. They wanted it to be edgier, more assertive and to show teeth from time to time. Others believed it should continue to build its role as a “trusted broker” with a quiet, respected voice, but widen its purview outside the hospital sector.
The Commission thus needs to be very clear and communicative about its long term kaitiakitanga 1 for the system, its medium term contribution and how to measure it, the specific interventions that will create most impact and its future spirit and character as an agency.
Acting on these matters will ensure that the gains made to date ‘stick’ and are resilient to changes in leadership, policy settings or priorities.
The Performance Challenge: Agency
1.
Purpose, targets and business strategy
Staff, while dedicated and positive, felt that strategic direction was uncertain and that their day to day work was more reactive and issues- based. There was a sense of being either
Continuous Improvement or servicing Mortality Review Committees They were hungry to know what the future state looks like and how success should be measured.
The Commission currently has three strategic priorities, as shown:
Shining a light – measuring and identifying areas for quality and safety improvement
Being an intelligent commentator and advocate for change
Lending a hand – providing expertise, guidance and advice to support improvement and spread good practice
1 Guardianship/protection
13
Its reputation is such that the Commission is now well placed to undertake inclusive work with stakeholders to sharpen these strategic priorities. The current priorities probably reflect the right areas of activity but they need to be more selective given the available resource base. With a $13.5 million baseline the agency must focus on the vital few things that matter most. It needs a disciplined strategy with strong safeguards against dilution.
The strategy system, or connectedness between the strategic priorities, should also be better articulated. Staff and stakeholders need to see a future direction that unifies the quality system the Commission operates: from the work of its Mortality Review Committees, through its intelligence and insight work, to its quality improvement activities. There is an opportunity to create a more joined up story.
The Commission’s vision could also be turned into an overall outcomes statement, or in PIF parlance, “a light on the hill”. The agency should articulate a singular collective ambition that is both intellectually and emotionally compelling. Its staff are passionate about their mission to lift system quality in service of patient safety and care and external stakeholders are highly receptive to its work. Some carefully facilitated work would quickly produce a more powerful articulation of agency ambition than currently exists. This would help staff find greater meaning in their work and signal the importance of the agency more strongly to the sector.
Above all, the current input and activity based performance metrics need to be much more output and outcome focussed, even if these are qualitative in nature. Many Crown entities struggle with attribution and assessment of impact within complex multi-agency ecosystems but it must be even further developed here. Improved strategic clarity and a clear light on the hill will assist with this.
2.
Operating Model
Once strategy is more tightly defined, the next step for the Commission is to articulate more explicitly the operating model through which it will deliver the required outputs and outcomes. In particular, this is likely to require attention to:
leadership and governance
prioritisation
product and service development
the stakeholder engagement model
the customer voice
knowledge management
14 SELF-REVIEW OF THE HEALTH QUALITY & SAFETY COMMISSION (HQSC) – SEPTEMBER 2015
culture and behaviours
The changes required in leadership and governance do not reflect weakness here, but are rather a function of the need to move out of ‘start up’ mode into a more mature and sustainable way of working. Some respondents also saw a need to tilt the balance away from ‘expert led’ (i.e. health academic or clinician led) leadership and governance, toward a more conventional model of management. This is a challenge in a quality agency where both are important.
The Board is well respected, and can now fix its vision more outwardly and long-term than it has had the luxury of doing to date. It should focus on lifting performance to the next level, building deeper succession around the CEO and management and operating in a more networked away across the system.
Strong and effective leadership by the Chief Executive (CEO) was a consistent message from stakeholders, though some felt that the wider senior leadership team could benefit from team building activity and targeted development in leadership and management.
Management’s decision making processes were sometimes not transparent to staff. Where
“busyness” was articulated as being the pervasive modus operandi.
With regard to the need for more effective prioritisation discussed above, we suggest that the Commission will need to manage its activities on more of a portfolio basis, with clear time horizons across initiatives as well as differentiation between top priority investments, more speculative investments and so on. This prioritisation needs to be clear to the sector and staff in order to manage the high expectations both have of the Commission.
The Commission is strong on implementation and project /programme rigour and we suggest it might now be useful to adopt some of the 90 day planning approaches that are used to good effect in other small public agencies. These give momentum to priority initiatives and enhance accountability for outputs and outcomes.
We suggest that given the array of possible quality improvement opportunities across the sector, the Commission should explore a new product/service triaging and development model. It needs to guard against the temptation to over diversify, understand the cost to serve of each product or service and their return on investment in both qualitative and quantitative terms.
Co-creation with the sector will become even more important and requires a special skill set.
The Commission has developed a range of trusted advisor relationships across the system.
However, too many of these relationships could be dependent on Board members and the current CEO. In order to move them to a more sustainable basis, a strategic stakeholder
15
management plan should now be developed and implicit understandings made more explicit.
In a health and disability system which sometimes struggles to focus on the customer or patient as opposed to provider delivery and expert opinion, the Commission is refreshingly direct in its commitment to bring customer voice to the wider system, including the voice of disadvantaged populations.
Whereas health care providers ask a patient: “what is the matter with you?” the role of the
Commission is to ask “what matters to you?” and to bring those answers into the system. It is focussed on improving safety and quality of our health and disability services so that fewer patients are harmed and more patients get care they actually need and value, wherever they live and regardless of ability to pay, age or ethnicity.
The culture of the Commission is strongly centred on the consumer. Thought needs to be given by both the Commission and the Ministry as to how to spread this commitment across the wider system given the slim resources the Commission has access to and the indirect nature of its system leadership. Success in the quality field lies in securing ownership of quality at the point of delivery.
The Commission has deep in-house analytical expertise relative to its size and gathers rich data in a range of areas. It will be challenging to operate knowledge management systems of any sophistication given the size of its resource base. As it continues to convert data into intelligence and insight for the system it might wish to consider some shared investments in this area with other system players.
Staff are attracted to the Commission because of its role in the system and mission to make things better for patients. New staff believe that the Commission has delivered on the recruitment promise and are enjoying it as a place to work. They feel the Commission is collegial and that this reflects in the quality of relationships with stakeholders. They are excited about becoming more and more data driven and about the respect they are earning in the system.
Longer serving staff described internal culture as vibrant and had a palpable sense of achievement. They feel they are ‘credible and listened to’ by the system and enjoy it when they are asked for advice by system players. Their joy lies in the fact that the system is starting to come to them, rather than a sense of having to push things onto the system.
Staff and leadership are conscious that they need to model internally the quality and qualities that they are asking for from the system. This could be enhanced by more positive story telling and celebration of success. Staff also felt that sometimes performance conversations didn’t happen soon enough and that non performers should be acted on more forcefully.
16 SELF-REVIEW OF THE HEALTH QUALITY & SAFETY COMMISSION (HQSC) – SEPTEMBER 2015
The negative aspects of culture are some ‘expert’ led behaviours butting up against the data, or expert behaviours in tension with customer voice. In this the Commission is probably a microcosm reflective of its sector, but it might be worth surfacing the internal tensions to stimulate more open discussion in this area.
3.
Implementation (including change capability)
The Commission implements effectively and has some real agility in change management, perhaps because of its small size, the capability of its staff and the high visibility, high touch style of the CEO.
There is real discipline around programmatics for campaigns and projects. However, as suggested above, we believe that an ongoing framework for fast paced performance execution such as a 90 day planning approach would reduce dependence on key personalities and sharpen accountability for results. Given the Commission is now entering a more mature phase of development more attention needs to be paid to repeatable systems and frameworks, rather than change being reliant on the discretionary efforts of a few key individuals.
4.
Organisational Agility
Agility and responsiveness to customers and stakeholders have been distinctive features of the Commission to date. It is a small and nimble gem of an agency within a large and sometimes slow moving system. As it focuses and specialises, it may find it challenging to recruit some of the specialist skills it needs in the local labour market. Workforce agility might be enhanced by adopting a more porous approach with staff coming in and out from the wider sector. The alumni network created by this approach would help spread quality improvement skills and attitudes around the system.
At present the Commission gains many benefits from its small size and relative independence from the rest of the sector. It is lightly monitored by the Ministry of Health.
Some likened it to a catalytic molecule in the health and disability system. It needs to take care not to ossify, bureaucratise or lose its current attributes of innovation, dynamism and speed.
What success will look like?
Views amongst stakeholders on what success would look like over the four year horizon were very disparate. For some it was to expand the Commission’s ambit and become “the place to turn to build quality, in any sense”. Some felt the agency was to some degree filling a vacuum created by other system players and that if the system as a whole was performing better, its role might be different.
17
While currently collegial in the tone of its sector relationships, many expected the
Commission to step up and “hold us more firmly to account”. They felt it had now earned the right to be more of a friendly critic. They want the agency to have louder voice in a more transparent era. One said: “it should not be a stick but a beacon for the patient”.
Most believed there needed to be demonstrable added value by the Commission to the outcomes of the health sector. For example, mortality review committees should have a tangible expectation that mortality rates are down as a result of their work.
Some suggested there should also be well understood benchmarking with other jurisdictions and that the Commission should be aiming for a top placing. In a small and unified country it should be possible for it to perform strongly in comparative terms.
Most felt that if the Commission did not exist, quality would fall back to being a nice to have in DHBs, given lack of system maturity in this space.
In future the Commission will need to continue to attract and retain both senior clinicians and professional experts in the quality improvement area. Stakeholders noted that quality improvement programme design is a rare skill and that the Commission is uniquely placed to offer this capability to the system.
Most wanted the Commission to move more to a whole of system approach (i.e. not just hospitals). This will place a further premium on the need to prioritise and operate on more of a portfolio basis.
As the Commission formulates these future priorities, it will need to be crystal clear about allocative efficiency: that is, to examine and evaluate the best return for the resources available to it. This will entail being comfortable to stop programmes that may have lower returns than others or which are not performing to targets.
When we asked what the Commission should NOT become in five years, respondents suggested:
The same
All things to all subsectors
A behemoth
Expert led rather than patient led
Apologetic
Hidden
Focussed only on its own data
18 SELF-REVIEW OF THE HEALTH QUALITY & SAFETY COMMISSION (HQSC) – SEPTEMBER 2015
In other words, most saw it as needing to exist, remaining small and tightly focussed, moving up the maturity curve from data gatherer and score keeper to predictive analytics, developing its brand and visibility and speaking more loudly on quality as the voice of the patient and in particular, disadvantaged populations.
The body of PIF work gives the ‘recipe’ for the next phase of the Commission’s development and the Commission’s Board and leadership are well placed to lift the game. Staff believe in it, the sector values it, trusts it and wants it to succeed. The Commission is perfectly placed to make the move from good to great.
Debbie Francis
External Advisor
Dr Karen Poutasi
External Advisor
19
SUMMARY OF RATINGS
What do the ratings mean?
Ratings help to clarify what are the agency’s relative strengths (or developing strengths) and the priority areas on which to focus to lift performance, given the challenges, risks and opportunities in the medium term. It is important to note that ratings are applied in terms of the future the agency is preparing for rather than as an assessment of current performance or of improvements in performance achieved to date.
Rating Judgement What it means
Strong
(Excellent)
Well placed
Developing
(see note below)
Weak
Unable to rate/not rated
Best practice/excellent
High level of capability and sustained and consistently high levels of performance
Systems in place to monitor and build capability to meet future demands
Organisational learning and external benchmarking used to continuously evaluate and improve performance.
Capable
Delivering to expectations with examples of high levels of performance
Evidence of attention given to assessing future demands and capability needs
Comprehensive and consistently good organisational practices and systems in place to support effective management.
Developing
Adequate current performance – concerns about future performance
Beginning to focus on processes, repeatability, evaluation and improvement and management beyond and across units
Areas of underperformance or lack of capability are recognised by the agency
Strategies or action plans to lift performance or capability, or remedy deficiencies are in place and being implemented.
Unaware or limited capability
Significant area(s) of critical weakness or concern in terms of delivery and/or capability
Management focuses on tasks and actions rather than results and impacts
Agency has limited or no awareness of critical weaknesses or concerns
Strategies or plans to respond to areas of weakness are either not in place or not likely to have sufficient impact.
There is either:
No evidence upon which a judgement can be made; or
The evidence available does not allow a credible judgement to be made.
Note: The SSC framework uses to term ‘needing development’ to describe this rating. The internal review team has used ‘developing’ as it considered that this is more consistent with a performance improvement approach.
20 SELF-REVIEW OF THE HEALTH QUALITY & SAFETY COMMISSION (HQSC) – SEPTEMBER 2015
Results
Government Priorities Rating
Government priority 1: delivering better value for money for government investment in the health and disability sector and demonstrating the difference that we make
Developing
Government priority 2: collecting good-quality, safety related data and putting the data to its best use Well placed
Government priority 3: working cooperatively with other agencies at topic and strategic planning level to influence sector wide results
Well placed
Government priority 4: : building clinical leadership and capability of the sector to improve and sustain improvement
Developing
Government priority 5: supporting partnerships with consumers at all levels Developing
Core Business
Rating
Core business 1: Shining a light
Strong
Core business 2: intelligent commentator and advocate for change Developing
Core business: Lending a hand
Strong
21
Organisational Management
Leadership, Direction and
Delivery
Rating
Purpose and Vision
Strategy
Leadership and Governance
Values, Behaviour and Culture
Review
Delivery for customers
Strong
Developing
Developing
Developing
Well placed
Rating
Customers
Operating model
Collaboration and partnerships
Developing
Well placed
Strong
Well placed
Experiences of the public
Relationships Rating
Engagement with Ministers
Sector contribution
People Development
Strong
Well placed
Rating
Leadership Development
Developing
Workforce Development
Strong
Management of People Performance
Developing
Developing
Engagement with Staff
Financial and Resource
Management
Rating
Asset Management
Information Management
Financial Management
Using financial resources to drive efficient and effective delivery
Risk Management
Developing
Strong
Strong
Developing
Developing
17
RESULTS
Part One: Delivery of Government Priorities
This section reviews the agency’s ability to deliver on its strategic priorities agreed with
Government.
Government priority 1: delivering better value for money for government investment in the health and disability sector and demonstrating the difference that we make
Performance Rating: Developing
This priority area has two parts:
Delivering value for money
Being able to demonstrate this
There is a clear indication from the interviews with external stakeholders and staff alike, that the Commission is using its money wisely and has delivered an impressive programme of work.
Being able to demonstrate value for money is another matter. Interviews with external stakeholders and staff highlighted that improved measurement and evaluation of impact as one of five key challenges for the Commission. In particular, interviewees noted that attribution is difficult (as it is with most agencies) and while the Commission has been working hard on improved output and outcome metrics, it needs to continue to lift the game and articulate both the quantitative and qualitative benefits it provides to the system.
There have been some promising quantitative indications that the work of the Commission with the sector is already starting to have measurable benefits. This is demonstrated in various Commission reports such as Window on Quality (as yet unpublished), the quality and safety markers reports, indicators report, mortality review committee reports, etc. In addition, the draft Victoria University/Otago University evaluation of the Commission noted that “with respect to the quality and safety markers there is evidence of strong and sustained improvements in most areas addressed by the Open Campaign over the period
2012-2014.”
The need for the Commission to articulate qualitative benefits from its work was also identified e.g. better use of information, culture shift and improved consumer involvement.
The draft Victoria University/Otago University evaluation of the Commission has noted that a culture shift was already evident – toward “no blame” and open reporting of adverse
18
events’. It also noted that the qualitative results demonstrated that the
Commission had already achieved a great deal on a small budget.
An example of a qualitative benefit would be bringing/influencing cohesion and focus in areas of high harm e.g. falls.
Whilst it is clear we are doing well as a relatively new agency, our performance has been rated as ‘developing’ in relation to where we need to be over the next four years. The four year excellence horizon notes that to be able to meet future needs, more clarity is needed about the medium term purpose, vision and strategy alongside a tighter system of prioritisation of activity and investment of effort.
It also notes that we need to be able to measure our impact across the whole organisation
(including mortality review) – both quantitative and qualitative.
The Commission has started to benchmark performance against other jurisdictions. Some people interviewed suggested that the Commission should be aiming for a top placing, noting that in a small and unified country it should be possible for it to perform strongly in comparative terms.
Government priority 2: analysing and reporting quality and safety related data and putting the data to its best use
Performance Rating: Well placed
In the drive for Better Public Services, government agencies should consider how to better use the diverse databases and information they hold. The Commission is already acknowledged as an agency with considerable expertise and capability in health quality and safety data (local, regional and national), making sense of it and presenting it in a variety of useful ways. There is an opportunity to build on this and take our place as a leader in the provision and use of data and information for quality improvement.
The Commission is increasingly becoming a trusted agency in relation to oversight and use of quality and safety data. As we increase our role in this area it will be important to that we safeguard our use of information for quality improvement, not for accountability or quality assurance purposes.
The interviews identified that the Commission has deep in house analytical capability relative to its size and rich data is gathered in a range of areas. However, given our resources, it could be challenging to grow this function without partnering with other system players.
The Commission goes well beyond simply analysing and publishing data. For each of our products, a real focus is on producing the information in a way that can be used by relevant stakeholders. There are established mechanisms for encouraging the sector to use the
19
information in ways to improve performance e.g. the Atlas of Healthcare Variation’s ‘find my patient’. This is an ongoing area of development.
Data that the Commission collects and analyses is used to put a spotlight on particular areas of health quality and safety such as specific topics (e.g. reducing harm from falls) or applying national data sets across regions (e.g. Atlas of Healthcare Variation). The Commission’s national reporting has demonstrated progress in the areas in which the Commission ‘shines a light’. By presenting data in an accessible way to the health and disability sector, its utility has been more apparent and therefore has contributed to highlighting areas for the system to focus on.
Government priority 3: working cooperatively with other agencies at topic and strategic planning level to influence sector wide results
Performance Rating: Well placed
The Commission is a small organisation pursuing and reaching our goals through working in partnership with the sector and with other agencies relevant to our work. We already do this well through (to name a few):
The sector
our expert advisory groups with clinical leaders, consumers, and other expertise as needed for each of our programmes. These expert advisory groups are an important way to link with the sector and play a major role in guiding the direction of programmes and providing independent clinical, consumer and/or technical advice
partnerships with DHBs
working with PHOs and ARC providers
Other government agencies
joint work programmes with other agencies, sometimes with joint funding arrangements. This includes (to name just a few) o working with ACC and the Ministry of Health on falls and fracture prevention o working with the Ministry of Health on the iPIF o Contributing to DHB Annual Plan and Regional Plan processes with the
Ministry of Health
active participation in various national strategic forums relating to health quality and safety such as the quality forum and national health information forum.
Interviews included the following observations about the Commission’s style and success in working cooperatively across the sector:
collegial in the tone of its sector relationships
have earned widespread trust and respect – listened to and asked for advice
stakeholders are starting to come to us
20
have developed trusted advisor relationships across the system
agile and responsive
Our success is also demonstrated by increased demand from across the sector to lead and guide work relating to quality and safety data collection and information, improvement capability and leadership, consumer engagement and partnerships and expanding our programme work into new areas. We are also experiencing significant demand from other government agencies and professional bodies for expert quality improvement advice. Of course this success brings its own challenges especially in relation to prioritising resources
(this is covered in other parts of this document).
When it comes to working at a strategic planning level across the sector, the picture is not quite as clear. The quality and safety forum (Ministry of Health, HDC, ACC and the
Commission) is not functioning yet as expected and there is a clear opportunity to develop this further.
To move to the next phase of the Commission’s development, some areas for development in the area of collaborative work were suggested:
working at a more strategic level with the sector and across government
Moving relationships to a more sustainable basis through development of a strategic stakeholder management plan.
There was a strong theme coming through that the Commission had now earned the right to be more of a friendly critic.
Government priority 4: building clinical leadership and capability of the sector to improve and sustain improvement
Performance Rating: Developing
Building sector capability and leadership in quality and safety is a key strategy for improving health care in NZ. The Commission is well recognised for its work in this area to date which has included the patient safety campaign, improvement programmes, organisation of visits by international experts and a variety of conferences, workshops, training and other events targeted across the spectrum of the health system. The Commission has also provided sponsorship of APAC forums and IHI Improvement Advisor training.
The Commission has acknowledged that there is an opportunity to support the sector in a more structured and comprehensive way. To this end it appointed an expert advisory group including representatives from Health Workforce NZ, the Ministry of Health, the broader sector and consumers and jointly developed a three year health quality and safety capability and leadership building programme. Some of the key challenges for the Commission over the next four years identified in this programme include ensuring all health and disability workers have minimum levels of the basic concepts and tools for quality improvement; ensuring there are sufficient numbers of quality improvement experts in the sector to lead and manage projects at local, regional and national levels, and that educational institutions
21
preparing people for careers in health and disability include quality improvement and patient safety education in their curriculums.
Government priority 5: supporting partnerships with consumers at all levels
Performance Rating: Developing
There is an increasing consumer voice and greater expectations from consumers that they will receive the best care possible and for this to be reflected in their experiences in the health care system and in partnerships with providers. There is growing evidence that partnerships between health service organisations/health professionals and patients and their families and carers results in improved health, better experience of care, more appropriate care, lower health costs and increased worker satisfaction. The Commission is already acknowledged as having expertise and capability in promoting and supporting consumer partnerships and there are good intentions in the sector that can be harnessed and built on. The Commission is seen as the only government agency championing this as a key strategic priority.
The external interviews identified that ‘in a health and disability system which sometimes struggles to focus on the customer or patient as opposed to provider delivery and expert opinion, the Commission is refreshingly direct in its commitment to bring customer voice to the wider system, including the voice of disadvantaged populations’.
The Commission has considerable strengths and has been proactive and innovative in this area since its establishment. However, the work is still on a small scale and with limited resources, and its influence in the sector is growing gradually.
Examples which demonstrate the proactive and innovative approach include (to name a few):
Co-design programmes
Guidance to DHB Boards on good practice
A commitment to consumer partnership internally through involvement of consumers in all our programmes - with consumer representation on all expert advisory groups and a consumer network.
work on health literacy in the primary care and pharmacy sector
taking a patient centred approach in all our work - which can be a conversation changer when there is a tension around funding and boundaries of responsibility. When we put the patient at the core of the conversation, it can break down all the silos.
The next four years offers an opportunity to expand our efforts in this area and confirm our place as leaders for the sector – especially to ensure that co-design becomes a mainstream activity. There is a need to challenge the systematic issues to create and embed partnership and sustain the relationships needed for true consumer engagement. We will also need to work with consumers to increase their capability to lead in this way. To measure our
22
progress/success in this area, it might be useful to consider a quality and safety marker or some other method for measuring progress.
There is also still a long way to go in the challenging area of health literacy - acknowledging that ‘every health care presentation is a health literacy opportunity’. Other priorities include the challenging conversations around end of life care (including advance care planning), and broadening into the NGO sector and community.
As one of the Commission’s three key strategic priorities, the challenge will be to ensure that this work is appropriately prioritised, both as work in its own right, and as an integral part of the existing work of improvement programmes.
23
Part Two: Delivery of Core Business
This section reviews how well the Commission delivers its core business.
Core business 1: Shining a light – measuring and identifying areas for quality and safety improvement/using information for quality improvement
Performance Rating: Well placed
Measurement and evaluation are essential for setting the quality and safety agenda, providing a catalyst for improvement and monitoring progress. Used wisely, monitoring and reporting on quality and safety can generate engagement by clinicians and consumers, and inform conversations about where problems and key opportunities for improvement exist.
The Commission’s measurement products are well regarded in the sector, as evidenced by the external interviews, their high use in the sector and the initial findings from the draft
Victoria University/Otago University evaluation of the Commission. We have consistently met our deliverables for this area of core business - which include the quality and safety markers, Atlas of Healthcare Variation, quality and safety indicators (including patient experience indicators), serious adverse events reporting and mortality reviews.
The external interviews confirmed that the Commission is acknowledged in the sector as an agency with considerable expertise and capability in health quality and safety data collection
(local, regional and national), making sense of it and presenting it in a variety of useful ways.
We are also increasingly becoming a trusted agency in relation to oversight and use of quality and safety data.
There is an opportunity to build on this and take our place as a leader in the sector in provision and use of data and information for quality improvement.
Core business 2: Being an intelligent commentator and advocate for change
Performance Rating: Developing
Whilst the Commission has always provided a level of intelligent comment and has consistently advocated for change, this has been carried out on an ad hoc basis until
2014/15 when it became one of the Commission’s three output classes. As a result it now has specific deliverables, resources (including staffing) and greater focus. This includes providing advice to government, contributing to cross government agency strategy and programmes, as well as providing advice to other agencies on issues such as consumer engagement and partnership, collection and use of quality and safety-related data, improvement education and training, family violence, child and youth mortality, methodologies and specific programme areas.
A new and developing part of this function has been publishing peer reviewed papers and opinion pieces. In the short space of 18 months since the first paper was published, three articles have been published in the NZ Medical Journal, one in the Australia NZ Journal of
Surgery and several opinion papers published in popular magazines. The Commission now has in place a dedicated resource and budget for continuing this role.
24
The external interviews identified that there is clear sector support for the Commission to play a much stronger role and to speak more loudly on quality as the voice of the patient and in particular, disadvantaged populations. They also identified that the Commission having now earned the respect of the system, can now afford to be a bit less ‘nice’. Many of those interviewed wanted the Commission to be edgier, more assertive and to ‘show teeth from time to time’. On the other hand, some believed the Commission should continue to build its role as a “trusted broker” with a quiet, respected voice, but widen its purview outside the hospital sector. These two approaches may be able to work together well.
In summary, although the intelligent commentator/advocate for change function is still developing, there is clearly a strong base in place, both in terms of internal resources, and external readiness, for the Commission to further build this area of core business.
Core business 3: Lending a hand – providing expertise, guidance and advice to support improvement and spread good practice
Performance Rating: Well placed
The Commission’s key deliverables since its inception have included the delivery of programmes which provide expertise, guidance and advice to support improvement and spread good practice.
The Commission has consistently delivered on its deliverables (as attested by our audits).
The external interviews also identified that the sector considers the Commission is strong on implementation and project /programme rigour. To move to the next level, the external reviewers suggest it might now be useful to adopt some of the 90 day planning approaches that are used to good effect in other small public agencies to give momentum to priority initiatives and enhance accountability for outputs and outcomes.
Our strength in implementing programmes is further confirmed by the findings of the draft
Victoria University/Otago University evaluation of the Commission. The draft report notes that ‘the qualitative results demonstrate widespread support for the work of The
Commission and acknowledgement that although a relatively young organisation they have achieved a great deal on a small budget and with a limited number of staff responsible for a national programme of health quality and safety improvement’. The evaluation also notes that ‘DHB staff at the three case study sites, CEOs of DHBs and Senior Managers all spoke highly of the work of The Commission and in particular the approachability and professionalism of the staff working at the Commission’.
As noted in the four year excellence horizon narrative, interviewees identified that the
Commission would need to continue to attract and retain both senior clinicians and professional experts in the quality improvement area. Stakeholders noted that quality improvement programme design is a rare skill and that the Commission is uniquely placed to offer this capability to the system.
25
Over the past 18 months, the Commission has put in place a new strategy to develop more flexible staff capability. Until recently, the Commission largely contracted lead agencies
(often DHBs) to deliver its time-limited projects. This approach was designed to encourage leadership and capability in the sector and leave us free to take an overview and focus on other core business. For a number of reasons this approach did not always achieve the intended results and was not achieving our objective of developing sector based capability.
As a result, the Commission shifted to retaining in-house expertise for its improvement programmes, in particular in-house expertise in quality improvement and patient safety and in project management. These generic roles allow greater flexibility and ability to manage change within the organisation. We also employed a medical advisor to provide medical leadership and advice to the Commission Board and staff, and be part of a broader network of clinical and improvement experts across the health sector to support the Commission’s work.
Given our strong record of success, and our strengthened and more flexible staffing position, the Commission is well placed to move to the next phase of development, and in particular, to be a hub for improvement programme design excellence.
In our ‘lending a hand’ capacity, internal and external stakeholders noted the need for the
Commission to develop a tighter system of prioritisation of activity and investment of effort.
The need to focus on less and be more concentrated on a particular area both was brought up by a number of staff. The review identified that there is already a well-established prioritisation process for new improvement programmes, and that there is an opportunity to review this and extend it to cover the totality of the Commission’s activities.
26
ORGANISATIONAL MANAGEMENT
This section reviews the Commission’s organisational management.
Leadership and Direction
Purpose, Vision and Strategy
How well do the staff and stakeholders understand the Commission’s purpose, vision and strategy?
How well does the Commission consider and plan for possible changes in its purpose or role in the foreseeable future?
Performance Rating (Purpose and Vision): Strong
Performance Rating (Strategy): Developing
Leadership and Governance
How well do the Board and Senior Leadership Team provide collective leadership and direction to the Commission?
Performance Rating: Developing
Values, Behaviour and Culture
How well does the Commission develop and promote the organisational values, behaviours and culture it needs to support its strategic direction?
Performance Rating: Developing
Review
How well does the Commission encourage and use evaluative activity?
Performance Rating: Well placed
27
This review deliberately separated ‘strategy’ from ‘purpose and vision’ as the reviewers considered it important to acknowledge the strong performance in relation to ‘purpose and vision’.
A collective purpose and vision
The purpose and vision of the Health Quality & Safety Commission was articulated clearly by staff: to make the health system safer, improve the quality and experience of health care and set the direction for patient safety. Comments were spontaneous and well beyond simply reciting the Commission’s strategic documents.
A strong theme to emerge in virtually all interviews was the importance of the Commission developing and sharing knowledge. This was noted as a particular position of strength.
According to many staff, the Commission provides a ‘national lens on health quality and safety’, connects the system and is a ‘knowledge hub’ that, depending on the context, develops, contributes to, or leads a national conversation.
Staff feel that the Commission is well positioned to increase its role as a leading commentator and opinion leader to keep a focus on quality and patient safety, providing a linking and facilitating role for the health and disability sector. Others also noted the
Commission’s role as challenging the status quo. The vision of being a ‘conscience for the sector’ in the health quality and safety arena was also mentioned.
Linking purpose and vision to strategy
The Commission’s strategy was not always well understood, despite a clear purpose and vision.
The external advisors noted in the four year excellence horizon that to move to the next phase, the Commission needs to:
develop greater clarity with respect to our role in the system and how to make the
Commission ‘matter more’ in the wider system.
clarify/sharpen the Commission’s medium term purpose, vision and strategy including what success looks like and how it should be measured. Develop a vision statement that is a ‘light on the hill’. Articulate a future direction that unifies the quality system the Commission operates; from the work of its Mortality Review
Committees, through its intelligence and insight work to its quality improvement activities – there is a chance to create a more joined up story.
Flexible and responsive
Overall, internal interviews revealed a work force that clearly identified and anticipated the need to be flexible in an ever-changing healthcare environment. It was readily acknowledged that improvement programmes do not continue indefinitely, tempered with the importance of allowing them to be sufficiently embedded to ensure a sustainable change can occur in any of the Commission’s improvement programme areas. Staff consider that while the
Commission’s core purpose and role may not change substantially, the needs of the health and disability sector are likely to and this will require the organisation to be responsive to external realities and needs.
The Commission staff interviewed noted that they have delivered ‘everything asked of us’ to date and have recognised the need to be an agency that keeps promises. The staff motivation was evident from the interviews. Staff perceive this has built a reputation of an
28
agency that ‘gets things done’. Legacy projects inherited from the Ministry of Health have been delivered well – the Commission is now poised to build on its place and voice beyond its inheritance. The idea of focusing on less and being more concentrated on a particular area was raised a number of times.
These findings were reflected in the findings of the external advisors, who noted, that to move forward, the Commission needed to develop a tighter system of prioritisation of activity and investment of effort. As noted under core business area 3 (Lending a hand), the review identified that there is already a well-established prioritisation process for new improvement programmes, and that there is now an opportunity to review this and extend it to cover the totality of the Commission’s activities.
Building an internal strategy/operational model
The Commission is at a tipping point as an organisation that has grown. The informal networks that have worked to date now require reinforcement with formal policies, systems and an internal focus on the business. Staff felt that this, in turn, would allow a clearer strategy to emerge.
The Commission’s Senior Leadership Team (SLT) was spoken of positively by staff. Many, however, were not always aware of SLT decisions or understood the group’s role (e.g. responsibility for leadership and performance versus being an expert group). The CEO was described as approachable and supportive. While leadership and the direction set were not overtly questioned, the need for better internal communication was a strong theme that emerged.
It was consistently noted that managers and SLT need to be more visible – this mainly refers to the organisation communicating better internally, especially in its growth and development phase. This was further emphasised by many in reference to the physical and geographical isolation felt by some staff.
It was acknowledged that the Commission provides good opportunities for continuous development of its leaders. These have included the LDC programme, leadership in practice, change management and an internal programme run by the principal improvement advisor.
All staff, including leadership have had regular opportunities to learn from acknowledged international change leaders.
Working with the Board
Staff recognised the credibility of its Board in the health sector, particular the Chair. It was noted that a number of accomplishments of the Commission could be attributed to the
Board chair’s credibility in the sector as well as international reputation. Staff felt that the connections of the Board could be better leveraged overall.
Board decision-making was described by staff as being oblique in that few staff had direct contact with members of the Board or knowledge of how Board decisions are made. While it is not unusual for a smaller group of staff to have more contact with Board members in any organisation, there was a clear willingness from all staff to better understand the type of information the Board is particularly interested in receiving that could assist with governing the Commission.
29
Many staff mentioned the possibility of developing ‘Board champions’: particular members of the Board that have governance oversight of particular strategic priorities or work programmes of the Commission.
There was some disconnect between various views about governance – from those preferring a more ‘pure’ governance approach to those preferring a more active role for
Board members e.g. as champions for particular strategic priorities or work programmes.
This demonstrated a clear need for more active orientation of staff about the role of a
Crown entity and the respective roles of governance and management.
Open for better communication
Be it SLT, management or the Board, it was widely acknowledged that now the Commission is no longer a ‘new agency’ and is now in its teenage years - so to speak - a more structured approach to internal communication would be an important improvement.
When considering collective leadership and direction for the Commission, the importance of the established clinical networks, particularly in the form of Expert Advisory Groups, was noted by staff. An opportunity was noted to further develop the Commission’s leadership, broadening this to include clinical leaders and networks that have been essential to the
Commission’s objectives to date. Although the Commission has made many external links and facilitated many relationships, a focus on communication between our internal networks could be an important focus for the next stage. This ensures that skills are shared across highly specialised teams.
Expressing our values
Similar to the Commission’s purpose and vision, staff responses demonstrated a surprising degree of uniformity in terms of the values, behaviour and culture that they experience and practice within the Commission – even if these are not well described in any formal sense.
There is an appetite to arrive at an agreed set of values that are easily understood and
‘actionable’ as part of the way we do business. With a number of new staff joining the
Commission in the past year, the recent workshop to discuss core values is timely.
The interviews by the external advisors reflected in the four year excellence horizon narrative, identified that new staff believe that the Commission has delivered on the recruitment promise and are enjoying it as a place to work, and that longer service staff experience a vibrant culture where they experience a sense of achievement.
Encouraging and using evaluating activity
The Commission’s improvement programmes have a long record of both evaluation of results and development of value for money analyses before any new programmes are implemented. The existing prioritisation process for proposed initiatives includes a requirement for any new proposal to include not only the proposed strategy to be tested but also how outcomes will be measured.
In the last few years, the SOI and SPE deliverables for most major reports, conferences and workshops, have included a requirement to measure their impact, for example through surveys to analyse usefulness and application of learnings to practice.
30
Delivery for Customers and New Zealanders
Customers
How well does the Commission understand who its customers are and their short and longer term needs and impact?
Performance Rating: Developing
Operating model
How well does the Commission’s operating model (the ‘how’) support delivery of government priorities and core business?
How well does the Commission evaluate service delivery options?
Performance Rating: Well placed
Collaboration and Partnerships
How well does the Commission generate common ownership and genuine collaboration on strategy and service delivery with partners and providers?
Performance Rating: Strong
Experiences of the Public
How well does the Commission employ service design, continuous improvement and innovation to ensure outstanding customer experiences?
How well does the Commission continuously seek to understand customers’ and New
Zealanders’ satisfaction and take action accordingly?
Performance Rating: Well placed
Knowing our customers
There was general agreement among the staff about who the Commission’s customers are, but divergent views about who the main customer should be, or where the Commission should put most of its energy to best serve its customers. Staff generally divided customers into the New Zealand public, the ‘health system’, and the Minister and Ministry of Health as well as other central agencies such as ACC. The Commission’s partnership and codevelopment with clinicians and the sector more broadly was noted many times. The focus on customers has been mostly external. Some voiced the importance of increasingly viewing the Ministry of Health and other crown agents as a customer.
31
Many identified the New Zealand public (consumers of health care) as one of the
Commission’s main customers. Views differed concerning the focus. For instance, it was debated whether it is important that the public are aware of the Commission more specifically or simply have a general awareness there is an agency ‘working for the public’ focusing on health quality and safety.
It was evident that customer focus to date has centred more on the hospital setting and that the Commission is now at an expansion phase, developing stronger links with District Health
Boards more broadly, primary care, aged residential care and the community.
The broadening customer base was noted in the draft Victoria University/Otago University evaluation of the Commission which noted that “the early work of the Commission focused on the DHBs, more recently the Commission has widened its focus and moved into primary health care, aged residential care and consumer engagement and is closer now to realising its mandate of working sector wide. It is generally acknowledged by stakeholders that this is a considerable challenge for a small organisation (approximately 50 staff) with limited resources. Harnessing the resources of the wider sector and achieving successful engagement will be pivotal to addressing real shifts in the provision of quality and safe service in the health sector”.
A few staff noted the different needs of internal versus external customers. Internal customers were referred to as funders such as the Ministry of Health and government.
External customers included hospitals and health care and the New Zealand public. A few staff commented that for the Commission’s further development of its relationships, the key question to ask with every interaction is ‘who is this message for’?
There was general agreement that customer needs are particularly well understood at the level of senior sector governance (e.g. DHB CEO, Chief Medical Officer,, Director of Nursing etc.) but less understood at the level of frontline staff. This could lead to a particular view of the system being formed that does not incorporate the views of the frontline adequately.
The same applied to incorporating the consumer voice.
Collaboration and partnerships - a friend of the sector
Relationships with our partners, central agencies, Ministers and Ministry of Health and consumers) were generally described very positively overall. The Commission’s focus on stakeholder relationships was clear. There are still some agencies where relationships could be further developed and deepened. This was also suggested by the external advisors in the four year excellence horizon, who recommend the development of a strategic stakeholder management plan.
The Commission has built a reputation as being a trusted and credible source of information and expertise and staff noted that partners they work with had described staff as ‘trusted’,
‘approachable’ and ‘knowledgeable’. Overall, the Commission is viewed as a ‘friend to the sector’. It was acknowledged that this is more readily achievable when positioned as a partner, rather than a regulator.
This concept of partnership was confirmed by the recent draft evaluation of the Commission carried out by Victoria University/Otago University which noted in its draft report that ‘the qualitative data involving interviews with CEOs of the DHBs, Senior Managers, Quality
Improvement Advisors and staff at the three DHB case study sites overwhelmingly supported
32
the idea that the Commission should be independent and remain as a Crown entity. In particular it was asserted that the Commission should remain independent of the Ministry of
Health and that this was an advantage in pursuing a health quality and safety improvement agenda and avoiding a focus on compliance. Further, it was believed that this would lead to a culture shift that was already evident – toward “no blame” and open reporting of adverse events’.
Staff also focused on the DHB as a customer of the Commission. While the Commission is well placed, there are many priorities across the health and disability sector, and it will be important for Commission priorities to complement local initiative. This does not preclude the Commission refining its position as an opinion leader. It was noted that smaller DHBs could welcome more support from the Commission and a different strategy might be required for larger DHBs.
The Commission has developed a number of programmes relatively quickly and maintaining engagement will be crucial in the next phase of the Commission’s development. A few commented that we need to plan in a way that ‘reaches past the fatigue and truly supports people to perform’. We also must continue to offer engaging events and programmes to maintain the momentum and ‘excite the sector’.
An area for growth is moving more beyond ‘working with the willing’ and developing a strategy to ensure that wider voices are gathered. This was echoed in an earlier section in terms of working with frontline staff.
Operating model
This is covered in some detail in the four year excellence horizon narrative which notes that once the strategy is more tightly defined, the next step is for us to articulate more explicitly the operating model through which we will deliver the required outputs and outcomes. It notes seven areas that need to be considered: leadership and governance; prioritization; product and service development; the stakeholder engagement model; the customer voice; knowledge management; and culture and behaviors. The narrative notes many strengths and also identifies areas for that need further development.
Experiences of the public.
Through the Patient Experience Survey, our consumer network, and consumer representation in all Commission programmes, the Commission is well placed to build on understanding the experiences of consumers of the health system. While this is positive, it was highlighted that the resources available to the Commission to build on this knowledge base are limited. Many staff emphasised that truly involving consumers into all aspects of how we design programmes or provide advice would take us from ‘well placed’ to ‘strong’.
33
Relationships
Engagement with Ministers
How well does the Commission provide advice and services to Ministers?
Performance Rating: Strong
Sector contribution
How effectively does the Commission work across the sector?
Performance Rating: Well placed
Engagement with Ministers
The strong rating is in relation to the question ‘How well does the Commission provide advice and services to Ministers?’ It would be ‘well placed’ or possibly even ‘developing’ if we were to answer a different question “How effectively does the Commission engage with
Ministers? We will discuss these two questions separately.
In relation to providing advice and services, the Commission’s primary engagement is with the Associate Minister of Health who has responsibility for the Commission. There have also been interactions with the Minister of Health and Minister for ACC. The relationship between the Minister’s offices and the Commission is strong and reporting from the
Commission is regular and transparent. The Chair, Chief Executive and other senior staff meet regularly with the Associate Minister and have developed a constructive working relationship.
Ensuring there is a link between advice from the Commission and advice from the Ministry of Health and other agencies needs to remain an important focus. Although the Commission can present independent advice, it is well recognised that the impact of the advice is dependent on working with other central government agencies. The relationship with the
Ministry of Health was particularly emphasised by staff. This was in reference to aligning priorities.
The effectiveness of our relationships with Ministers is less clear. We value our primary relationship with the Associate Minister of Health, but this may inevitably mean that we are likely to be missing opportunities to impact on broader health and disability sector discussions at Ministerial level. Our vision is to be ‘sitting at the table’ for cross-cutting strategic discussions (both at Ministerial and central agency level), and this is not always the case at this stage. It is an area where the Commission plans to place much greater emphasis in future.
Sector contribution
The Commission’s work across the sector has been noted in the previous section (under
‘collaboration and partnerships: a friend of the sector’). As previously described, the
34
Commission effectively uses the resources it has to work across the health and disability system and with consumers. The Commission is now looked to as the connector of people, agencies and systems to raise the profile of health quality and patient safety and contribute to affecting and sustaining change.
The Commission is increasingly working beyond traditional health care settings and engaging with the social sector, particularly in the area of family violence prevention, child and youth and suicide mortality. An area of development for the Commission is in building on its relationship with Treasury to further understand the economics of the health system (i.e. the aspect of New Zealand’s Triple Aim to have ‘best value for public health resources’).
People Development
Workforce development
How well does the Commission develop its workforce?
How well does the Commission anticipate and respond to future capacity and capability requirements?
Performance Rating: Strong
Leadership development
How well does the Commission develop its leadership?
Performance Rating: Developing
Management of people performance
How well does the Commission encourage high performance and continuous improvement amongst its workforce?
How well does the Commission deal with poor or inadequate performance?
Performance Rating: Developing
Engagement with staff
How well does the Commission manage its employee relations?
How well does the Commission develop and maintain a diverse, highly committed and engaged workforce?
Performance Rating: Developing
35
A developing workforce
Staff were very positive about the workforce development opportunities offered by the
Commission. The organisation is strong in this area. Career development opportunities and access to senior leaders and mentors both within and outside the Commission was noted as not being possible in larger organisations.
Staff felt very well supported to pursue career development and noted the internal capacity and capability of staff has grown exponentially as a result. However, these views need to be balanced with those that identified ‘a limited career path/progression’. The risk is the loss of institutional knowledge, so the importance of sharing and spreading knowledge came though strongly as well.
Leadership development has been deliberately separated for the purpose of this internal review. With the Commission’s growth, keeping pace with the necessary leadership development has been a challenge. ‘Leadership’ here refers to a range of aspects such as managers receiving appropriate training in human resources, policy advisors receiving
‘thought leadership’ and ensuring the transference of knowledge and skills. It was acknowledged that this is emerging but requires more development.
Staff felt that there could be more sharing of skills across the Commission as well as a way for staff to better know the knowledge and skills that reside within the Commission, particularly as there are a number of new staff. A lack of succession planning was highlighted as a risk.
As a small agency that is virtually at capacity, people employed here are technically ‘at the top of their game’ and opportunities for job growth are limited. Staff have commented however, that they have a high degree of autonomy in their jobs and that it is possible to establish a trusted and respected reputation amongst leaders in the sector. They also noted the opportunities to work with some of the ‘best of the best’ from both New Zealand and internationally.
Dealing with the family
Managers described a workforce that is ‘high performing’ overall. The organisation is described as caring, family-oriented and health-focused. This is beneficial for staff and leads to a positive workplace. As the Commission has grown and developed, so too has staff loyalty and an environment of mutual respect and support.
While this is a very positive endorsement from staff, the flipside is that when poor performance does occasionally arise, it can be a challenge to implement the correct steps in such an environment. Human Resource policies were described as ‘patchy’ and many of the core systems that worked well when the Commission was established can no longer serve an organisation of this size.
Managers in particular noted the need to have better access to HR support and need upskilling on how to manage poor performance.
36
Integration
A key word mentioned by virtually all staff interviewed was ‘integration’: having a better connection within and across teams including how staff work together and how effectively internal capacity is used.
Many staff commented that the mortality review committees in particular needed to be better integrated across the entire organisation. It was acknowledged that the unique legislation under which the committees operate and the ‘dualistic reporting’ to committee chairs as well as the Commission contributed to the production of this silo. Staff also noted the need for more integration with the Commission’s consumer engagement, measurement and evaluation and leadership and capability building strategic programmes as they are essential to ‘everything that we do’.
Improvement programmes were emphasised as the ‘effector arm’ of the Commission and this requires better use of data developed in house. For example, the use of recommendations from mortality review committee reports, the use of the atlas, or other measurement and evaluation data.
Better use could be made of team meetings and this would contribute to the Auckland office feeling more integrated with the rest of the Commission. The team meeting was identified multiple times as an area for improvement. One suggestion was to use the monthly reports to fill the information gap and to, instead, have staff catch ups to get the opportunity to connect with each other without the need for any particular structure and include internal
‘guest speakers’.
Our workforce was noted to not be particularly diverse. The diversity exists more in the
Commission’s networks than it does internally. This was highlighted as an important area of development. The population that the Commission serves needs to be better reflected in the staff employed.
37
Financial and Resource Management
Asset Management
How does the Commission manage agency and Crown assets, and the agency balance sheet, to support delivery and drive performance improvement?
Performance Rating: Developing
Information Management
How well does the Commission manage and use its information as a strategic asset?
Performance Rating: Strong
Financial Management
How well does the Commission plan, direct and control financial resources to drive efficient and effective output delivery?
Performance Rating (financial management): Strong
Performance Rating: (Driving efficient and effective output delivery): Developing
Risk Management
How well does the Commission identify and manage agency and Crown risk?
Performance Rating: Developing
Asset management
This section was interpreted in a broad sense, covering not only our responsibility to manage our money and property responsibly, but also our knowledge, knowhow, methodologies and such like. There was general agreement that our physical assets are well managed.
Those specifically asked this question noted that we have important assets in relation to our products and people. They suggested the need to ensure ‘knowledge transfer’ and to build our new talent pool of people. They noted that we are somewhat light on succession planning – which is a risk when a lot of knowledge resides in the few people.
Information management
The Commission’s data and information is strong: high quality data reporting was noted as a position of strength for the Commission. As a ‘strategic asset’, this is managed well. As
38
previously noted, the Commission’s role and reputation as a ‘knowledge hub’ continues to grow. This was also referred to as being a ‘curator for the sector’. Users see the value in the data and information that the Commission provides.
The use of information for performance improvement and measuring progress has been outlined in other parts of this report – most significantly under Government Priorities 1 and
2 and Core Business 1.
Financial management
Financial Management
The Commission delivers on its objectives within its annual allocation and this has been the case since the Commission’s inception. Overall budget management and external reporting was described as strong by both staff and the Board and particular mention was made of the
CFO in this regard.
Audit NZ rates the Commission as ‘very good’ on financial management.
Using financial resources to drive efficient and effective delivery
Communication about internal budgeting was noted as an area of development. Although the Commission works within its allocation and remains within budget, it is not always straightforward to track expenditure over budget and this tends to be aligned towards the end of each financial year. A way to track budgets in ‘real time’ was recommended by many staff.
Staff were also asked, at a broader level, about how well we plan, direct and control financial resources to drive efficient and effective output delivery i.e. how our financial resources are allocated to ensure they are being used in the best way. There was a sense from a number of people interviewed, that the Commission’s high level strategic priorities were constrained by historic budget allocations instead of driving budget allocations. In other words, budgets tend to follow historical patterns rather than being a bottom up process based on
Commission wide priorities. Considering a shift in approach would also enhance the
Commission working at a strategic level with other agencies.
Risk management
Staff interviews identified that risks were well managed. Strategic risks are a regular Board agenda item and there is a regular risk management process at individual programme level.
With increased staff in programme areas, a more structured programme management approach is emerging with regular reporting on progress, including risks.
39
However, the existing organisation wide risk management register is not being used or updated in the intended way for regular reporting of operational risks. This process needs to be reviewed and any resulting recommendations put into practice.
40
APPENDIX A
Draft upgrade as at 30 March 2015
Version 8
Four-year Excellence Horizon
What is the agency’s performance challenge ?
Delivery of Government Priorities
How well is the agency responding to government priorities?
Delivery of Core Business
In each core business area, how well does the agency deliver value to its customers and New Zealanders?
In each core business area, how well does the agency demonstrate increased value over time?
How well does the agency exercise its stewardship role over regulation?
Leadership and
Direction
Purpose, Vision and Strategy
Leadership and
Governance
Values,
Behaviour and
Culture
Review
Organisational Management
How well is the agency positioned to deliver now and in the future?
Delivery for
Customers and
New Zealanders
Customers
Operating
Model
Collaboration and
Partnerships
Experiences of the Public
Relationships
Engagement with Ministers
Sector
Contribution
People
Development
Leadership and
Workforce
Development
Management of People
Performance
Engagement with Staff
Financial and
Resource
Management
Asset
Management
Information
Management
Financial
Management
Risk
Management
41
Lead Questions
42
APPENDIX B
List of Interviews
This review was informed by input provided by two staff focus groups, 25 individual staff interviews and 13 interviews with the following external stakeholders.
Agency/Organisation
Associate Minister of Health
Director General of Health
ACC CEO
The Treasury
Chair of the DHB Chair’s group
Senior DHB staff including CEs, General Managers, a Chief Medical Officer, a Director of
Nursing and other staff responsible for clinical governance
President of the NZ Royal College of GPs
Chair of Council of Medical Colleges
43