Main_Document
advertisement

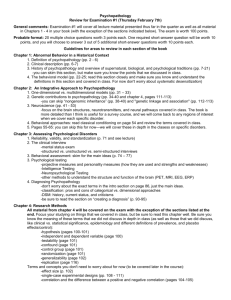
Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 1 Abstract To establish which social interactive behaviours predict later psychiatric diagnosis, we examined 180 videos of a parent-infant interaction when children were aged one year, from within the Avon Longitudinal Study of Parents and Children (ALSPAC) cohort. Sixty of the videos involved infants who were later diagnosed with a psychiatric disorder at seven years, and 120 were a randomly selected sex-matched control group. Interactive behaviours for both the caregiver and the one year old infant were coded from the videos according to eight holistic categories of interpersonal engagement: Well-being, Contingent Responsiveness, Cooperativeness, Involvement, Activity, Playfulness, Fussiness, and Speech. Lower levels of adult activity and speech in interaction at one year significantly predicted overall diagnosis of child psychiatric disorder. Keywords: Autism, conduct disorder, ADHD, disruptive behaviour disorder, depression, anxiety, developmental, infancy, mother-infant interactions; parenting; parent-child; parent psychopathology. Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 2 Introduction Atypicalities in interpersonal behaviours in early adult-infant interaction have been associated with childhood diagnosis of psychopathology, including disruptive behaviour disorders (DBDs), pervasive developmental disorder (PDD) and emotional disorders (Field, Healy, Goldstein, Perry, Bendell, Schanberg et al., 1988; Kubicek, 1980; Trevarthen & Aitken, 2001; Morrell & Murray, 2003; Halligan, Murray, Martins, & Cooper, 2007; Webb & Jones, 2009; Murray, Marwick, & Arteche, 2010; Saint-Georges et al., 2011). Parenting styles and environment are indicated, in addition to genetic vulnerabilities, to be risk markers in relation to the development of DBDs, including attention deficit hyperactivity disorder (ADHD), Oppositional Defiant Disorder (ODD), and Conduct Disorder (CD) (Zahn-Waxler, Iannotti, Cummings, & Denham, 1990; Campbell, Pierce, March, & Ewing, 1991; Latimer et al., in press). Bidirectional influences between observable child behaviour problems and parent-child interactions are reported (Lifford, Harold, & Thapar, 2008), with early infant ‘difficult’ temperament found to contribute to irritable parenting style, and low maternal responsiveness in combination with infant temperament predicting conduct problems (Shaw, Owens, Vondra, & Keenan, 1996; Guerin, Gottfried, & Thomas, 1997; Lahey et al., 2008). Children with ADHD are more likely to be reported by their mothers to have been fussy, irritable and active as infants (Weiss & Hechtman, 1993), with higher activity levels seen as early as the first months of life (Rothbart, 1989; Auerbach et al., 2005) and within the first year (Auerbach, Atzaba-Poria, Berger, & Landau, 2004; Auerbach et al., 2008). Compared to controls, mothers of children with ADHD are found to be generally more directive, negative and less socially interactive, and children with ADHD less compliant and more negative (Cunningham & Barkley, 1979; Barkley, Karlsson, & Pollard, 1985; Campbell, Breaux, Ewing, Szumowski, & Pierce, 1986; Jacobvitz & Sroufe, 1987; DuPaul, McGoey, Eckert, & VanBrakle, 2001; Olson, Bates, Sandy, & Schilling, 2002). Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 3 Early intervention can support parenting behaviours and environmental adaptations to help to optimise positive developmental outcomes for infants (Guralnick, 2004; Landry, Smith, & Swank, 2006; Dawson, 2008), and intervention at a later point can be ineffective (Shaw, Bell, & Gilliom, 2000). Reliable identification of predictors in early care-giver and infant interactions of later child psychopathology are likely to be of value in the targeting of early intervention and support but research into the relations between psychopathology and the parent–infant relationship within a longitudinal non-clinical context has been sparse (Thompson et al., 2010). Additionally, previous studies have been disorder specific, often using an ‘at risk’ group, which has not enabled comparison between disorders, nor consideration of early risk markers of cooccurring disorders. Several studies have used adult or child reported perceptions as their assessment measure, which does not have the objectivity of independent or prospective observation. A longitudinal population based cohort study affords prospective analysis, using systematic observational assessment, of early interactive behaviours for both adults and infants in relation to a range of later diagnosed disorders, and based on a contemporary birth cohort, we examined whether there are particular social interactive behaviours which predict later diagnosis of a range of psychiatric disorders. Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 4 Method Participants The sample consists of participants from the Avon Longitudinal Study of Parents and Children (ALSPAC). ALSPAC is an ongoing population-based study investigating a wide range of environmental and other influences on the health and development of children. Pregnant women resident in the former Avon Health Authority in south-west England, having an estimated date of delivery between 1 April 1991 and 31 December 1992 were invited to take part, resulting in a ‘core’ cohort of 13,988 singletons/twins alive at 12 months of age (Golding, Pembrey, Jones, & the ALSPAC Study Team, 2001). Ethical approval for the study was obtained from the ALSPAC Law and Ethics Committee and the Local Research Ethics Committees. All adult participants gave their informed consent prior to their inclusion in the study. The present study examined video footage from a sub sample of the core ALSPAC cohort who were invited to attend Children in Focus clinics after birth. A range of measures was collected at the clinic visits, including regular questionnaires completed by the parents, medical assessments and biological samples collected for biochemical and genetic analyses. When the children were 12 months old the clinic session for the 1240 participating families (usually mother/infant dyads) included the Thorpe Interaction Measure (TIM) (Thorpe, Rutter, & Greenwood, 2003). The TIM involves a caregiver and child sharing a picture book, and the adult is asked to engage the child in this activity as they would at home. The same ‘living room’ style environment in the clinic was used for all interactions, and the interaction was video-recorded. Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 5 Sixty of the infants from the Children in Focus cohort later received diagnoses of one or more psychiatric disorders using the Development and Wellbeing Assessment (DAWBA) (Goodman, Ford, Richards, Gatward, & Meltzer, 2000) which was administered to all children remaining in the cohort at 91 months of age. The DAWBA is a structured diagnostic assessment which relies on parental report as well as teacher reports (Goodman et al., 2000), but final diagnoses are assigned by a child psychiatrist. The TIM videos of these 60 case infants were analysed in the current study, and the TIM videos of a further 120 infants from the cohort were randomly selected for analysis to comprise a sex-matched control group. Within the case infant group there were 26 cases of any oppositional-conduct disorder (of which there were 19 “pure” cases without ADHD comorbidity), 35 cases of disruptive behaviour disorders (28 without comorbidity), five cases of conduct disorder alone (3 without comorbidity), six cases of pervasive developmental disorder (autism), and 25 and five infants diagnosed respectively with any anxiety (15 without comorbidity) or any depressive disorder (1 without comorbidity). There were 16 infants diagnosed with any form of ADHD (nine without comorbidity), of which five had inattentive ADHD. The majority (89%) of the caregivers in the videos analyses were mothers. The mean duration of these caregiver-infant interactions was 211 (SD 84.5) seconds with a range from 60 to 510 seconds. Procedure Assessors were blind to the case or control status of the children in the videos. Interactive behaviours for both the caregiver and the one year old infant were coded from the videos according to a holistic measure using eight categories, namely: well-being, contingent Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 6 responsiveness, cooperativeness, involvement, activity, playfulness, fussiness and speech. All parent and child scores in each category are on a scale of 1 to 5 of overall extent of occurrence (see Appendix A for Holistic Measure). This system is adapted from the categories of interpersonal interaction developed by Marwick and Trevarthen (1982, 1986), to reflect elements of mood, engagement, attentional focus, interpersonal supportiveness, and expressiveness in adult-infant interaction, which are key in typical social communicative development, concordant inter-subjectivity, and interpersonal well-being (Trevarthen, 2001; Marwick & Murray, 2008; Marwick, in press), and which encompass the altered interpersonal behaviours noted previously to be associated with later diagnosed psychiatric disorder. Statistical Methods All subjects with available holistic interaction scores were used in the analyses. Initial descriptive statistics were generated across the eight holistic categories for both caregiver and infant, with all scores on a scale of 1 to 5. Inter-rater reliability tests using weighted kappa statistics and rank correlations were carried out for all holistic measures, from a randomly selected sample of n=29 adult-infant pairs. To check that the reliability sample was representative of the whole group, Wilcoxon tests were used to compare holistic categories between adult-infant pairs with and without reliability records. To reduce the variable set into smaller meaningful groups of holistic measures, a scree plot was used to assess the number of latent factors to pursue, after which maximum likelihood factor analysis was applied. Varimax rotation was used, though similar results were obtained when using a promax rotation. Factor scores were derived by summing those holistic scores with an absolute factor loading of more than 0.5 (after reversing any measures with a large negative loading). These factor scores were then used in predictive models of case and control status overall and within the following sub-diagnostic groups; any ADHD; inattentive ADHD; any emotional disorder (anxiety and depression); PDD; DBD; any Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 7 oppositional conduct disorder; conduct disorder alone; oppositional defiant and/or DBD-NOS; pure oppositional conduct disorder. The low prevalence seen for some of the outcomes made it necessary to use Firth's penalised-likelihood logistic regression method (Frith, 1993) for odds ratio (OR) estimates and corresponding 95% confidence intervals (CI) and p-values, implemented using the “logistf” package for R (Ploner, Dunkler, Southworth, & Heinze, 2010). Models were adjusted either for the sex of the infant alone, or for the sex of the infant and the depression and anxiety scores of the mother at 32-40 weeks gestation and 8 months postnatal. Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 8 Results Holistic assessments were made on 178 infants and their parents’ behaviour during the videos, with two videos excluded due to poor video quality. Table 1 shows the mean and standard deviation of each holistic interaction score, for caregivers and infants, overall and for the cases and controls separately. Appendix Table B.1 provides the number and percentage of videos with each possible score from 1 to 5, for cases and controls. Many scales showed little variation with the majority of videos given the same score. (Table 1. to be inserted here). No significant differences were observed between adult-infant pairs with and without reliability records (data not shown). Appendix Table B.2a shows reliability statistics for the 16 individual variables. Adult involvement and fussiness scores showed little variability and were therefore removed from subsequent factor analysis. Despite high proportions for agreement levels for most individual scores, scales with little variation resulted in low weighted kappa statistics. A scree plot derived from the 14 remaining scores (Appendix Figure B.1) suggested four latent variables. Factor loadings are shown in Table 2, with items grouped according to the factor to which they were most strongly loaded. With the exception of infant wellbeing, no item had a loading of more than ±0.5 on more than one factor. Four items (adult contingency and infant involvement, speech and activity) did not load highly on any factor. Intuitively, factors 1, 3 and 4 are comprised largely of variables paired on adult and infant scores for cooperativeness, wellbeing and playfulness respectively. Factor 2 comprised adult speech and activity. Reliability statistics for factor scores derived from these four groups of items, shown in Appendix Table B.2b, showed improved reliability compared to that of scores on individual measures. (Table 2 to be inserted here). Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 9 Table 3 shows summaries of the case sub-diagnostic groups, with low prevalence noted for inattentive ADHD, pervasive development disorder, depression and conduct disorders. (Table 3 to be inserted here). Table 4 shows means (SD) for factor analysis derived scores, Factor 1 and Factor 2, and ORs for caseness and all case subgroups with 95% CIs and p-values, adjusted for the sex of the infant and maternal depression and anxiety at 32-40 weeks gestation and 8 months postnatal. Factor 1 was not significantly associated with any outcomes, although when adjusted for sex only it was associated with pure oppositional-conduct disorder (OR=0.64, p=0.047). Across all models adjusted for the sex of the infant and maternal mental state, Factor 2 (adult speech and activity) showed strong associations with overall caseness and within all sub-diagnostic groups except pervasive development disorder and pure oppositional conduct disorder. For every one standard deviation increase in the combined adult verbal/activity score, the odds of being a case infant was reduced by 43% (95% CI: 20%, 60%; p=0.001). Adjusting for the sex of the infant alone slightly weakened the associations between the outcomes and Factor 2, with the result that the associations with conduct disorder alone (OR=0.47, p=0.069) and oppositional defiant and/or DBD NOS (OR=0.64, p=0.067) were no longer significant. Factor groups 3 and 4 did not associate significantly with overall caseness or any sub-diagnostic group. (Table 4 to be inserted here). Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 10 Discussion Our holistic analysis of interpersonal behaviours within early social interaction has shown adult activity and adult speech in combination to strongly predict later psychiatric diagnosis in the child at seven years of age. Specifically, lower levels of adult activity and lower levels of adult speech significantly predicted caseness and the diagnostic groups of: any ADHD, inattentive ADHD, any emotional disorder, any anxiety disorder, DBDs, oppositional defiant and/or DBDNOS, and CD at seven years of age. No predictors were found in the interactive behaviours of the child. Several studies have found associations between caregiver behaviour, developmental outcomes and later child psychiatric diagnosis (Jacobvitz & Sroufe, 1987; Campbell et al., 1991; Belsky, Hsieh, & Crnic, 1998; Olson et al., 2002; Beebe et al., 2011). These findings highlight the inverse relationship between maternal responsiveness during the first year of life and future child conduct problems (Shaw et al., 1996; Kochanska, 1997; Wakschlag & Hans, 1999; Olson, Bates, Sandy, & Lanthier, 2000), with maternal postnatal depression also associated with adverse cognitive, behavioural and emotional development in the child (Cogill, Caplan, Alexandra, Robson, & Kumar, 1986; Murray, Kempton, Woolgar, & Hooper, 1993; Halligan et al., 2007; Cooper, Murray, & Halligan, 2010; Murray, Halligan, & Cooper, 2010), and maternal ADHD symptoms being negatively associated with positive parenting (Murray & Johnston, 2006; Chronis-Tuscano et al., 2008; Semple, Mash, Ninowski, & Benzies, 2011). The association between lower levels of adult activity and speech and child psychopathology that we have observed is concordant with previous studies. Low maternal initiation and responsiveness have been related to the development of behavioural problems (Gardner, 1994), and reported also in mothers of children with ADHD (Cunningham & Barkley, 1979; Mash & Johnston, 1982; Harvey et al., 2003; Murray & Johnston, 2006; Chen & Johnston, 2007; Chronis-Tuscano et al., 2008; Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 11 Banks, Ninowski, Mash, & Semple, 2008). Vocalisations of depressed mothers in early interactions have a slower response time and show less length variation with infant age (Bettes, 1988; Reissland, Shepherd, & Herrera, 2003). However, in our analysis the predictive strength of the adult activity and speech scores was not explained by depression or anxiety of the adults. The prospective non-clinical cohort design of the ALSPAC study has enabled us to confirm that the same two categories of parental behaviour at one year predict diagnosis of a wide range of later attention, conduct and emotional psychopathologies in the child. This finding lends some support to the suggestion that parental ADHD symptoms may be a non-specific risk factor for multiple dimensions of child psychopathology (Humphreys, Mehta, & Lee, 2010). Given previous evidence of negativity and irritability found in parenting behaviours in relation to conduct problems and DBDs (Barkley, Anastopoulos, Guevremont, & Fletcher, 1992) it is of note that factors involving adult behaviour categories of well-being, contingent responsiveness, cooperativeness, and playfulness were not found in this study to be significant predictors of later child psychopathy. The lack of predictive association found for variables other than adult activity and speech may reflect the situational context of the reading task in which the adult and infant dyads were participating, with the caregiver asked to share a picture book with their infant and to engage their child in this activity as they would at home. The structure of the reading activity can be understood to accentuate the facilitating role of the adult in ‘framing’ and directing the task activity, and to reduce the social demand of the context in comparison to, for example, an unstructured play situation where ideas for activities have to be generated and negotiated. Additionally, sessions were terminated when the child lost interest in the activity, or showed signs of upset. Adults were not required to refocus the child, meaning parenting approaches in relation to dealing with child distress or potential non-compliance were not filmed. Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 12 The context of the reading task situation may also explain the finding that no infant behaviour category predicted later development of psychopathology. Previous studies have indicated differences in the behaviours of infants who are later diagnosed with a psychopathology, such as negative emotionality, fussiness and hyperactivity (Weiss & Hechtman, 1993; Guerin et al., 1997; Shaw et al., 1996; Auerbach et al., 2005), however, our study found no significant differences in the overall activity of the infants, nor evidence of infant emotionality being a predictor of later disorder. The structured focus of the task may have served to modulate the child’s activity, with the interpersonal behaviour range of the child being more limited by the scaffolding measures adopted in the task by the caregiver, and, with sessions being terminated when the child lost interest in the book or became upset, strong negative emotionality would not have been present. Nevertheless, previous research has also indicated that in relation to ADHD and hyperactivity symptoms in the early years, ‘non-optimal caregiving’ behaviour could not be attributed to observed infant behaviour (Jacobvitz & Sroufe, 1987; Carlson, Jacobvitz, & Sroufe, 1995; Morrell & Murray, 2003). No predictors in the interpersonal behaviours of adult or child were found for PDD, which may have been a consequence of low power due to small sample sizes in this group of disorder (n=6). A second explanation may be the object focussed structure and reduced interpersonal demand of the task context. Limitations A limitation of the present study is the structured context of the activity, which was object centred and may have reduced the social demand of the interaction, possibly ‘masking’ or preventing behaviours that would otherwise take place in a context in which the infant and adult Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 13 could generate ideas for activity and negotiate shared and individual intentions. The visual content of the videos was also limited at times. The camera recording the mother-infant interaction had been placed in an upper corner of the room, resulting in the faces of the participants not always being visible. Additionally, small sample sizes in relation to particular disorders may have led to type 2 errors and there are potentially cases within the control group in the present study, and vice versa (Foreman, Foreman, Prendergast, & Minty, 2001; Sayal, Goodman, & Ford, 2006); both under-diagnosis and over-diagnosis which routinely occur in ADHD (Angold, Erkanli, Egger, & Costello, 2000; Reid, Hakendorf, & Prosser, 2002). Strengths of the Study The primary strength of the present study is that we used data from a prospective longitudinal non-clinically based population cohort study. This has allowed us to apply the same assessment measures to the interactions of case and control dyads in relation to a range of psychiatric disorders, enabling comparison of predictors between and amongst disorders and consideration of predictors of co-occurring disorders. Unlike many other studies which have been retrospective, it does not have to rely on parental reports which can be subject to memory recall problems. Another strength of the present study is that all the children involved underwent psychiatric assessment at age 7 years using the DAWBA (Goodman et al., 2000) with all case children receiving assessment of data by a child psychiatrist. Lastly, the present study also made a partial adjustment for caregiver psychopathology via the maternal anxiety and depression ratings data, which is important to strengthen the conclusions we draw from our findings given that there is much evidence indicating the impact of parental psychopathology on infant cognitive and psychological development. Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 14 Clinical Implications The finding in early parenting behaviour at one year of two risk markers for later attention, behaviour and emotional psychopathologies in the child indicates these behaviours as areas of focus for early screening research, and supports the involvement of parents in interventions (McLaughlin & Harrison, 2006; Johnston & Jassy, 2007; Burke, Pardini, & Loeber, 2008). Interventions focused on promoting parental responsiveness and infant cognitive stimulation have resulted in parenting changes and improvements in the infant’s developmental outcomes in the preschool years (van den Boom, 1995; Landry et al., 2006), and the identification of caregiver activity and speech levels as predictors of a range of later child psychopathology will further inform the formulation of targeted interventions. Future research Our results have shown that at 12 months, two categories of parental behaviours in a structured book reading context can be identified which predict later attention, conduct and emotional disorders in the child. Interactive context is known to influence interpersonal behaviours (Wilson et al., 2011) and future research in a prospective population cohort should examine parent and infant behaviours in other observational contexts to investigate the identification of additional risk markers of later child pathology. Conclusion Holistic analysis of early caregiver-child interaction at one year has shown lower levels of parental activity and speech to predict diagnosis of a range of later psychopathologies in the child. As key risk markers within early interaction, these parental behaviours could inform the development of a focused observational screening tool, accessible to clinicians and health Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY practitioners. 15 The commonality of these risk markers to a range of attention, conduct and emotional disorders, indicates that targeted intervention programmes could also be developed to support these parental interactive behaviours. Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 16 Table Captions Table 1. Mean (SD), for Holistic Adult and Infant interaction scores, overall and by case-control status. Table 2. Factor analysis of the 14 holistic variables, assuming 4 latent factors. Loadings exceeding ± 0.5 shown in bold. Table 3. Number of cases overall and number and percentage within each sub-diagnostic group, overall and by gender. Table 4. Mean (SD) of predictors 'Factor 1' and 'Factor 2', within controls, cases overall and case sub-diagnostic groups. Sex-adjusted OR's estimates for caseness associated with a 1 SD increase in predictors, 95% confidence intervals and p-values. Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 17 References Angold, A., Erkanli, A., Egger, H. L., & Costello, E. J. (2000). Stimulant treatment for children: A community perspective. Journal of the American Academy of Child and Adolescent Psychiatry, 39, 975-984. Auerbach, J. G., Atzaba-Poria, N., Berger, A., & Landau, R. (2004). Emerging developmental pathways to ADHD: Possible path markers in early infancy. Neural Plasticity, 11, 29-43. Auerbach, J. G., Landau, R., Berger, A., Arbelle, S., Faroy, M., & Karplus, M. (2005). Neonatal behavior of infants at familial risk for ADHD. Infant Behavior and Development, 28, 220224. Auerbach, J. G., Berger, A., Atzaba-Poria, N., Arbelle, S., Cypin, N., Friedman, A., & Landau, R. (2008). Temperament at 7, 12, and 25 months in children at familial risk for ADHD. Infant and Child Development, 17, 321-338. Banks, T., Ninowski, J. E., Mash, E. J., & Semple, D. (2008). Parenting behavior and cognitions in a community sample of mothers with and without symptoms of attentiondeficit/hyperactivity disorder. Journal of Child and Family Studies, 17, 28–43. Barkley, R. A., Karlsson, J., & Pollard, S. (1985). Effects of age on the mother child interactions of ADD-H and normal boys. Journal of Abnormal Child Psychology, 13, 631-637. Barkley, R. A., Anastopoulos, A. D., Guevremont, D. C., & Fletcher, K. E. (1992). Adolescents with attention deficit hyperactivity disorder: mother-adolescent interactions, family beliefs and conflicts, and maternal psychopathology. Journal of Abnormal Child Psychology, 20, 263-88. Beebe, B., Steele, M., Jaffe, J., Buck, K., Chen, H., Cohen, P., Kaitz, M., Markese, S., Andrews, H., Margolis, A., & Feldstein, S. (2011). Maternal anxiety symptoms and mother–infant self- and interactive contingency. Infant Mental Health Journal, 32,174-206. Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 18 Belsky, J., Hsieh, K. H., & Crnic, K. (1998). Mothering, fathering, and infant negativity as antecedents of boys’ externalising problems and inhibition at age 3 years: differential susceptibility to rearing experience? Development and Psychopathology, 10, 301-320. Bettes, B. A. (1988). Maternal depression and motherese: temporal and intonational features. Child Development, 59, 1089-96. Burke, J. D., Pardini, D. A., & Loeber, R. (2008). Reciprocal relationships between parenting behavior and disruptive psychopathology from childhood through adolescence. Journal of Abnormal Child Psychology, 36, 679-692. Campbell, S. B., Breaux, A. M., Ewing, L. J., Szumowski, E. K., & Pierce, E. W. (1986). Parent identified problem preschoolers - mother-child interaction during play at intake and 1-year follow-up. Journal of Abnormal Child Psychology, 14, 425-440. Campbell, S. B., Pierce, E. W., March, C. L., & Ewing, L. J. (1991). Noncompliant behavior, overactivity, and family stress as predictors of negative maternal control with preschool children. Development and Psychopathology, 3, 175–190. Carlson, E. A., Jacobvitz, D., & Sroufe, L. A. (1995). A developmental investigation of inattentiveness and hyperactivity. Child Development, 66, 37-54. Chen, M., & Johnston, C. (2007). Maternal inattention and impulsivity and parenting behaviors. Journal of Clinical Child and Adolescent Psychology, 36, 455–468. Chronis-Tuscano, A., Raggi, V. L., Clarke, T. L., Rooney, M. E., Diaz, Y., & Pian, J. (2008). Associations between maternal attention-deficit/hyperactivity disorder symptoms and parenting. Journal of Abnormal Child Psychology, 36, 1237–1250. Cogill, S., Caplan, H., Alexandra, H., Robson, K., & Kumar, R. (1986). Impact of maternal postnatal depression on the cognitive development of young children. British Medical Journal, 292, 1165–1167. Cooper, P., Murray, L., & Halligan, S. (2010). Treatment of Postpartum Depression. Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 19 Encyclopedia on Early Childhood Development. Published online May 18, 2010. Website accessed on the 28th of September 2011. Cunningham, C. E., & Barkley, R. A. (1979). Interactions of normal and hyperactive-children with their mothers in free play and structured tasks. Child Development, 50, 217-224. Dawson, G. (2008). Early behavioral intervention, brain plasticity, and the prevention of autism spectrum disorder. Development and Psychopathology, 20, 775-803. DuPaul, G. J., McGoey, K. E., Eckert, T. L., & VanBrakle, J. (2001). Preschool children with attention-deficit/hyperactivity disorder: Impairments in behavioral, social, and school functioning. Journal of the American Academy of Child and Adolescent Psychiatry, 40, 508-515. Field, T., Healy, B., Goldstein, S., Perry, S., Bendell, D., Schanberg, S., Zimmerman, E.A., & Kuhn, C. (1988). Infants of depressed mothers show "depressed" behavior even with nondepressed adults. Child Development, 59, 1569-79. Firth, D. (1993). Bias reduction of maximum likelihood estimates. Biometrika, 80, 27–38. Foreman, D., Foreman, D., Prendergast, M., & Minty, B. (2001). Is clinic prevalence of ICD-10 hyperkinesis underestimated? Impact of increasing awareness by a questionnaire. European Child and Adolescent Psychiatry, 10, 130-134. Gardner, F. E. M. (1994). The quality of joint activity between mothers and their children with behavior problems. Journal of Child Psychology and Psychiatry, 35, 935-948. Golding, J., Pembrey, M., Jones, R., & the ALSPAC Study Team. (2001). ALSPAC – the Avon Longitudinal Study of Parents and Children: I. Study methodology. Paediatric and Perinatal Epidemiology, 15, 74–87. Goodman, R., Ford, T., Richards, H., Gatward, R., & Meltzer, H. (2000). The Development and Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 20 Well-Being Assessment: Description and initial validation of an integrated assessment of child and adolescent psychopathology. Journal of Child Psychology and Psychiatry, 41, 645-655. Guerin, D. W., Gottfried, A. W., & Thomas, C. W. (1997). Difficult temperament and behaviour problems: A longitudinal study from 1.5 to 12 years. International Journal of Behavioral Development, 21, 71–90. Guralnick, M. J. (2004). Family investments in response to the developmental challenges of young children with disabilities. In Kalil, A., & Deleire, T. (Eds.), Family investments in children’s potential: Resources and parenting behaviors that promote success (pp. 119–137). Mahwah, NJ: Erlbaum. Halligan, S. L., Murray, L., Martins, C., & Cooper, P. J. (2007). Maternal depression and psychiatric outcomes in adolescent offspring: a 13-year longitudinal study. Journal of Affective Disorders, 97, 145-154. Harvey, E., Danforth, J. S., Eberhad, T., McKee, T., Ulaszek, W. R., & Friedman, J. L. (2003). Parenting of children with attention deficit/hyperactivity disorder (ADHD): The role of parental ADHD symptomatology. Journal of Attention Disorders, 7, 31–42. Humphreys, K. L., Mehta, N., & Lee, S. S. (2010). Association of parental ADHD and depression with externalizing and internalizing dimensions of child psychopathology. Journal of Attention Disorders, 2010 Dec 20. [Epub ahead of print]. Jacobvitz, D., & Sroufe, L. A. (1987). The early caregiver-child relationship and attention-deficit disorder with hyperactivity in kindergarten - A prospective-study. Child Development, 58, 1496-1504. Johnston, C., & Jassy, J. S. (2007). Attention-deficit/hyperactivity disorder and Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 21 oppositional/conduct problems: links to parent-child interactions. Journal of the Canadian Academy of Child and Adolescent Psychiatry = Journal de l'Academie canadienne de psychiatrie de l'enfant et de l'adolescent, 16, 74-79. Kochanska, G. (1997). Mutually responsive orientation between mothers and their young children: Implications for early socialization. Child Development, 68, 94–112. Kubicek, L. F. (1980). Organisation in two mother-infant interactions involving a normal infant and his fraternal twin brother who was later diagnosed as autistic. In T. Field, S. Goldberg, D Stein, & A. Sostek (Eds.). High risk infant and children: Adult and peer interactions. New York: Academic Press. Lahey, B. B., Van Hulle, C. A., Keenan, K., Rathouz, P. J., D'Onofrio, B. M., Rodgers, J. L., & Waldman, I. D. (2008). Temperament and parenting during the first year of life predict future child conduct problems. Journal of Abnormal Child Psychology, 36, 1139-1158. Landry, S. H., Smith, K. E., & Swank, P. R. (2006). Responsive parenting: Establishing early foundations for social, communication, and independent problem-solving skills. Developmental Psychology, 42, 627–642. Latimer, K., Thompson, L., Kemp, J., Wilson, P., Gillberg, C., & Minnis, H. (in press). Attention Deficit Hyperactivity Disorder, Conduct Disorder and other Disruptive Behaviour Disorders: A systematic review of antenatal and early years risk factors. Child: Care, Health and Development. Lifford, K. J., Harold, G. T., & Thapar, A. (2008). Parent-child relationships and ADHD symptoms: A longitudinal analysis. Journal of Abnormal Child Psychology, 36, 285-296. Marwick, H., & Murray, L. (2008). The effects of maternal depression on the ‘musicality’ of infant directed speech and conversational engagement. In Malloch, S., & Trevarthen, C. (Eds.). Communicative Musicality: Narratives of Expressive Gesture and Being Human. (p. 281 -300). Oxford: Oxford University Press. Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 22 Marwick, H. (in press). Augmentative Communication. Language Learning Support of Children with Profound and Multiple Learning Difficulties (PMLD). In Handicap, Education and Participation – Encyclopaedia of Special Education. Stuttgart: Kohlhammer. Mash, E. J., & Johnston, C. (1982). A comparison of the mother–child interactions of younger and older hyperactive and normal children. Child Development, 53, 1371–1381. McLaughlin, D. P., & Harrison, C. A. (2006). Parenting practices of mothers of children with ADHD: The role of maternal and child factors. Child and Adolescent Mental Health, 11, 82-88. Morrell, J., & Murray, L. (2003). Parenting and the development of conduct disorder and hyperactive symptoms in childhood: a prospective longitudinal study from 2 months to 8 years. Journal of Child Psychology and Psychiatry, 44, 489-508. Murray, L., Kempton, C., Woolgar, M., & Hooper, R. (1993). Depressed mothers' speech to their infants and its relation to infant gender and cognitive development. Journal of Child Psychology and Psychiatry, 34, 1083-1101. Murray, C., & Johnston, C. (2006). Parenting in mothers with and without attentiondeficit/hyperactivity disorder. Journal of Abnormal Psychology, 115, 52–61. Murray, L., Marwick, H., & Arteche, A. (2010). Sadness in mothers' 'baby-talk' predicts affective disorder in adolescent offspring. Infant Behavior and Development, 33, 361-4. Murray, L., Halligan, S. L., & Cooper, P.J. (2010). Chapter 8. Effects of postnatal depression on mother-infant interactions, and child development. In: Wachs T, Bremner G, eds. Handbook of Infant Development. Volume 2, Second Edition. Malden, MA: WileyBlackwell. Olson, S. L., Bates, J. E., Sandy, J. M., & Lanthier, R. (2000). Early developmental precursors of externalizing behavior in middle childhood and adolescence. Journal of Abnormal Child Psychology, 28, 119–133. Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 23 Olson, S. L., Bates, J. E., Sandy, J. M., & Schilling, E. M. (2002). Early developmental precursors of impulsive and inattentive behavior: from infancy to middle childhood. Journal of Child Psychology and Psychiatry, 43, 435-447. Ploner, M., Dunkler, D., Southworth, H., Heinze, G. (2010). logistf: Firth's bias reduced logistic regression. Reid, R., Hakendorf, P., & Prosser, B. (2002). Use of psychostimulant medication for ADHD in South Australia. Journal of the American Academy of Child and Adolescent Psychiatry, 41, 906-913. Reissland, N., Shepherd, J., & Herrera, E. (2003). The pitch of maternal voice: a comparison of mothers suffering from depressed mood and non-depressed mothers reading books to their infants. Journal of Child Psychology and Psychiatry, 44, 255-61. Rothbart, M. K. (1989). Temperament in childhood: A framework. In Kohnstamm, G. A., Bates, J. E., & Rothbart, M. K., Ed.(s). Temperament in childhood (pp. 59–73). NY:Wiley. Saint-Georges, C., Mahdhaoui, A., Chetouani, M., Cassel, R. S., Laznik, M. C., Apicella, F., Muratori, P., Maestro, S., Muratori, F., & Cohen, D. (2011). Do parents recognize autistic deviant behavior long before diagnosis? Taking into account interaction using computational methods. PLoS One, 6, e22393. Epub 2011 Jul 27. Sayal, K., Goodman, R., & Ford, T. (2006). Barriers to the identification of children with attention deficit/hyperactivity disorder. Journal of Child Psychology and Psychiatry, 47, 744-750. Semple, D. L., Mash, E. J., Ninowski, J. E., & Benzies, K. M. (2011). The relation between maternal symptoms of attention-deficit/hyperactivity disorder and mother-infant interaction. Journal of Child and Family Studies, 20, 460-472. Shaw, D. S., Owens, E. B., Vondra, J. I., & Keenan, K. (1996). Early risk factors and pathways in Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 24 the development of early disruptive behavior problems. Development and Psychopathology, 8, 679-699. Shaw, D. S., Bell, R. Q., & Gilliom, M. (2000). A truly early starter model of antisocial behavior revisited. Clinical Child and Family Psychology Review, 3, 155–172. Thompson, L., Kemp, J., Wilson, P., Pritchett, R., Minnis, H., Toms-Whittle, L., Puckering, C., Law, J., Gillberg, C. (2010). What have birth cohort studies asked about genetic, pre- and peri-natal exposures and child and adolescent onset mental health outcomes? A systematic review. European Child and Adolescent Psychiatry, 19, 1-15. Thorpe, K., Rutter, M., & Greenwood, R. (2003). Twins as a natural experiment to study the causes of mild language delay: II: Family interaction risk factors. Journal of Child Psychology and Psychiatry, 44, 342-355. Trevarthen, C., & Marwick, H. (1982). Cooperative Understanding in Infancy. Project report to the Spencer Foundation, Chicago. University of Edinburgh. Trevarthen, C., & Marwick, H. (1986). Signs of motivation for speech in infants, and the nature of a mother's support for the development of language. In Lindblom, B., & Zetterstrom, R. (eds.). Precursors of Early Speech. p. 279-308. New York: Stockholm Press. Trevarthen, C. (2001). Intrinsic motives for companionship in understanding: Their origin, development, and significance for infant mental health. Infant Mental Health Journal, 22, 95-131. Trevarthen, C., & Aitken, K. J. (2001). Infant intersubjectivity: Research, theory, and clinical applications. Journal of Child Psychology and Psychiatry, 42, 3-48. van den Boom, D. C. (1995). Do first-year intervention effects endure? Follow-up during toddlerhood of a sample of Dutch irritable infants. Child Development, 66, 1798–1816. Wakschlag, L. S., & Hans, S. L. (1999). Relation of maternal responsiveness during infancy to the Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 25 development of behavior problems in high-risk youths. Developmental Psychology,35, 569579. Webb, S. J., & Jones, J. H. (2009). Early identification of autism: early characteristics, onset of symptoms, and diagnostic stability. Infant Young Child, 22, 100-118. Weiss, G., & Hechtman, L. T. (1993). Hyperactive boys grown up: ADHD in children adolescents, and adults. New York: Guildford Press. Wilson, P., Puckering, C., McConnachie, A., Marwick, H., Reissland, N., & Gillberg, C. (2011). Inexpensive video cameras used by parents to record social communication in epidemiological investigations in early childhood—A feasibility study. Infant Behaviour and Development, 34, 63 – 71. Zahn-Waxler, C., Iannotti, R.J., Cummings, M. E., & Denham, S. (1990). Antecedents of problems behaviors in children of depressed mothers. Development and Psychopathology, 2, 271–291. Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 26 Appendix A Holistic Measure (Coded Manually) All categories rated for adult and infant separately on a 5 point scale of extent of occurrence. 1. Overall well-being Definition: a judgment on the overall positive emotional state of the infant and adult throughout the segment (is each happy and relaxed?). Rated on a 5 point scale. 2. Overall contingent responsiveness Definition: a judgment of the overall contingent responsiveness of infant and adult to each other throughout the segment (are they responsive to each other’s expressiveness and communication?). Rated on a 5 point scale. 3. Overall co-operativeness Definition: a judgment on the overall co-operativeness of infant and adult in relation to each other throughout the segment (do they comply with each other’s wishes and coordinate their actions?). Rated on a 5 point scale. 4. Overall involvement Definition: a judgment of the overall involvement of infant and adult in the task or focus of activity throughout the segment (is each engaged in the activity?). 5. Overall Activity Levels Rated on a 5 point scale. Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 27 Definition: a judgment on the overall activity levels of infant and adult throughout the segment (is there energy and movement?). Rated on a 5 point scale. 6. Overall playfulness Definition: a judgment on the overall playfulness of infant and adult throughout the segment (is there fun, games, smiling and laughter?). Rated on a 5 point scale. 7. Overall fussiness Definition: a judgment on the overall fussiness of infant and adult throughout the segment (is there restlessness, negativity and lack of compliance with each other’s wishes?). Rated on a 5 point scale. 8. Overall Speech Definition: a judgment on the overall speech or vocalisation levels of infant and adult throughout the segment (is there vocal expressiveness?). Rated on a 5 point scale. Appendix B Table B.1. Number and percentage of case and control videos by score for holistic adult and infant interaction variables. Control Case Scores 1 2 3 4 5 1 2 3 4 5 Wellbeing adult 0 0 2(2%) 19(16%) 98(82%) 0 0 2(3%) 15(25%) 42(70%) Wellbeing infant 0 1(1%) 10(8%) 31(26%) 77(64%) 0 0 5(8%) 19(32%) 35(58%) Contingency adult 0 0 8(7%) 38(32%) 73(61%) 0 0 9(15%) 20(33%) 30(50%) Contingency infant 0 8(7%) 33(28%) 46(38%) 32(27%) 0 7(12%) 13(22%) 28(47%) 11(18%) Cooperativeness adult 0 2(2%) 2(2%) 33(28%) 82(68%) 0 5(8%) 15(25%) 39(65%) 5(8%) Cooperativeness infant 0 1(1%) 11(9%) 35(29%) 72(60%) 0 0 6(10%) 21(35%) 32(53%) Involvement adult 0 0 0 6(5%) 113(94%) 0 0 1(2%) 4(7%) 54(90%) Involvement infant 1(1%) 8(7%) 36(30%) 54(45%) 20(17%) 0 7(12%) 21(35%) 21(35%) 10(17%) Activity adult 0 3(2%) 20(17%) 88(73%) 8(7%) 1(2%) 2(3%) 19(32%) 33(55%) 4(7%) Activity infant 2(2%) 2(2%) 23(19%) 82(68%) 10(8%) 0 0 12(20%) 42(70%) 5(8%) Playfulness adult 75(62%) 36(30%) 7(6%) 1(1%) 0 39(65%) 17(28%) 3(5%) 0 0 Playfulness adult 83(69%) 30(25%) 5(4%) 1(1%) 0 42(70%) 14(23%) 3(5%) 0 0 Fussiness adult 117(98%) 2(2%) 0 0 0 58(97%) 1(2%) 0 0 0 Fussiness infant 96(80%) 16(13%) 7(6%) 0 0 44(73%) 13(22%) 2(3%) 0 0 Speech adult 0 8(7%) 24(20%) 83(69%) 4(3%) 1(2%) 8(13%) 20(33%) 27(45%) 3(5%) Speech infant 13(11%) 54(45%) 39(32%) 12(10%) 1(1%) 6(10%) 28(47%) 21(35%) 4(7%) 0 Table B.2a. Proportion agreement levels, inter-rater reliabilities and rank correlations of the 16 holistic variables. % agreement Inter-rater Inter-rater weighted Kappa rank correlation Involvement Infant Score 0.60 0.73 Wellbeing Infant Score 0.80 0.66 Contingency Infant Score 0.40 0.59 Fussiness Infant Score 0.80 0.40 Speech Infant Score 0.50 0.49 Cooperativeness Adult Score 0.67 0.49 Speech Adult Score 0.80 0.59 Playfulness Adult Score 0.67 0.44 Cooperativeness Infant Score 0.57 0.32 Playfulness Infant Score 0.83 0.24 Activity Adult Score 0.83 0.18 Activity Infant Score 0.70 0.19 Contingency Adult Score 0.57 0.12 Wellbeing Adult Score 0.73 0.04 Involvement Adult Score 0.93 -0.04 Fussiness Adult score* 0.97 0.00 *n/a for fussiness adult score as all values=1 for one of the raters. 0.75 0.73 0.58 0.55 0.55 0.51 0.43 0.42 0.38 0.37 0.31 0.21 0.07 0.04 -0.04 n/a Table B.2b. Inter-rater reliabilities and rank correlations of the 4 holistic factor analysis latent variables. Factor 1 Factor 2 Factor 3 Factor 4 Inter-rater weighted Kappa Inter-rater rank correlation 0.53 0.66 0.61 0.47 0.64 0.62 0.46 0.40 Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 30 Figure B.1. Scree plot of eigenvalues from 14 holistic variables (adult involvement and fussiness removed). The shaded area shows a 95% confidence band for eigenvalues from 100 simulated random (uncorrelated) data sets, with the number (dimension) of non-trivial factors indicated by the number of eigenvalues exceeding the random eigenvalues Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 31 Table 1. Table 1. Mean (SD), for Holistic Adult and Infant interaction scores, overall and by case-control status. Total Group Control Case Wellbeing Adult Score 4.76 (0.48) 4.81 (0.44) 4.68 (0.54) Wellbeing Infant Score 4.53 (0.67) 4.55 (0.69) 4.51 (0.65) Contingency Adult Score 4.48 (0.67) 4.55 (0.62) 4.36 (0.74) Contingency Infant Score 3.81 (0.90) 3.86 (0.90) 3.73 (0.91) Cooperativeness Adult Score 4.62 (0.62) 4.64 (0.61) 4.58 (0.65) Cooperativeness Infant Score 4.48 (0.69) 4.50 (0.70) 4.44 (0.68) Involvement Adult Score 4.93 (0.27) 4.95 (0.22) 4.90 (0.36) Involvement Infant Score 3.66 (0.88) 3.71 (0.86) 3.58 (0.91) Activity Adult Score 3.78 (0.63) 3.85 (0.56) 3.63 (0.74) Activity Infant Score 3.83 (0.63) 3.81 (0.68) 3.88 (0.53) Playfulness Adult Score 1.43 (0.63) 1.45 (0.65) 1.39 (0.59) Playfulness Infant Score 1.35 (0.60) 1.36 (0.61) 1.34 (0.58) Fussiness Adult Score 1.02 (0.13) 1.02 (0.13) 1.02 (0.13) Fussiness Infant Score 1.26 (0.55) 1.25 (0.56) 1.29 (0.53) Speech Adult Score 3.60 (0.73) 3.70 (0.65) 3.39 (0.85) Speech Infant Score 2.43 (0.82) 2.45 (0.85) 2.39 (0.77) Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 32 Table 2. Table 2. Factor analysis of the 14 holistic variables, assuming 4 latent factors. Loadings exceeding ± 0.5 are shown in bold. Item Factor 1 Factor 2 Factor 3 Factor 4 Cooperativeness Infant Cooperativeness Adult Contingency Infant 0.91 0.58 0.54 0.04 -0.03 0.05 0.04 0.12 0.17 0.01 0.09 0.05 Speech Adult Activity Adult 0.01 -0.02 0.90 0.88 0.08 0.03 0.07 0.10 Wellbeing Infant Fussiness Infant Wellbeing Adult 0.53 -0.46 0.44 0.01 -0.01 0.14 0.73 -0.62 0.52 0.10 0.01 0.05 Playfulness Infant Playfulness Adult 0.13 0.05 0.05 0.23 0.11 0.14 0.98 0.75 Involvement Infant Contingency Adult Speech Infant Activity Infant 0.44 0.21 0.01 -0.11 0.08 0.46 0.12 0.27 0.41 0.16 0.35 0.32 0.07 0.15 0.21 0.10 Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 33 Table 3. Table 3. Number of available cases overall and number and percentage within each sub-diagnostic group, overall and by gender. Total Gender Female Male Nobs 178 56 122 Ncases 59 18 41 16 (27%) 2 (11%) 14 (34%) Inattentive ADHD 5 (8%) 2 (11%) 3 (7%) Pervasive development disorder 6 (10%) 1 (5%) 5 (12%) Any emotional disorder 27(45%) 12 (63%) 15 (37%) Any anxiety disorder 25 (42%) 12 (63%) 13 (32%) 5 (8%) 2 (11%) 3 (7%) Disruptive behaviour disorders (DBD) 35 (60%) 8 (45%) 27 (66%) Any oppositional-conduct disorder 26 (44%) 6(33%) 20 (49%) 5 (8%) 1(5%) 4 (10%) Oppositional defiant and/or DBD NOS 21 (37%) 5 (28%) 16 (39%) Pure oppositional conduct disorder 19 (33%) 6 (33%) 13 (32%) N (%) of cases Any ADHD Any depressive disorder Conduct disorder alone Running head: EARLY PREDICTORS OF CHILDHOOD PSYCHOPATHOLOGY 34 Table 4. Table 4. Mean (SD) of predictors 'Factor 1' and 'Factor 2', within controls, cases overall and case sub-diagnostic groups. OR estimates for caseness associated with a 1 SD increase in predictors, 95% confidence intervals and p-values, adjusted for the sex of the infant and pre- and post-natal maternal depression and anxiety. Factor 1 N Mean (SD) Factor 2 OR (95% CI) Mean per SD; p-value (SD) OR (95% CI) per SD; p-value Control 120 13.0 (1.8) - 7.5 (1.1) - Case 59 12.7 (1.8) 0.84 (0.61, 1.17); p=0.310 7.0 (1.5) Any ADHD disorder 16 12.8 (1.8) 0.88 (0.52, 1.57); p=0.657 0.42 (0.23, 0.70); 6.6 (1.9) p=0.001 12.0 (1.9) 0.68 (0.34, 1.43); p=0.281 0.19 (0.04, 0.56); 5.4 (2.2) p=0.001 0.56 (0.24, 1.43); 7.2 (1.0) p=0.212 Inattentive ADHD 5 0.57 (0.40, 0.80); p=0.001 Pervasive development disorder 6 13.3 (1.8) 1.23 (0.54, 3.58); p=0.659 Any emotional disorder 27 13.3 (1.7) 1.15 (0.70, 1.98); p=0.588 6.9 (1.8) 0.51 (0.31, 0.80); p=0.003 Any anxiety disorder 25 13.3 (1.7) 1.13 (0.67, 1.97); p=0.654 6.8 (1.8) 0.47 (0.28, 0.75); p=0.001 12.4 (1.9) 0.75 (0.52, 1.09); p=0.132 6.9 (1.6) 0.53 (0.34, 0.79); p=0.001 Any oppositional26 conduct disorder 12.4 (1.8) 0.76 (0.50, 1.17); p=0.208 7.0 (1.3) 0.50 (0.31, 0.80); p=0.004 Conduct disorder 5 alone 12.2 (1.6) 0.70 (0.32, 1.56); p=0.361 6.6 (1.3) 0.37 (0.12, 0.98); p=0.045 Oppositional defiant and/or DBD Nos 21 12.5 (1.9) 0.80 (0.50, 1.30); p=0.359 7.0 (1.4) 0.53 (0.31, 0.89); p=0.016 Pure oppositional 19 conduct disorder 12.1 (1.9) 0.66 (0.42, 1.05); p=0.076 7.2 (1.3) 0.63 (0.37, 1.09); p=0.094 Disruptive behaviour disorders 35