Institutional Logics and Business Models: International Comparative
advertisement

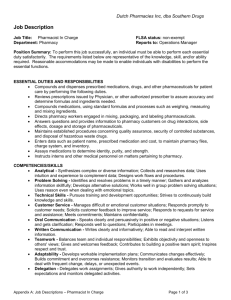
AOM submission # 14103 Institutional Logics and Models of Retail Pharmacy: A Comparison of Sweden, Italy, UK and USA Trish Reay (University of Alberta) Trish.Reay@ualberta.ca Giuseppe Delmestri (University of Bergamo) giuseppe.delmestri@unibg.it Beth Goodrick (Florida Atlantic University) goodrick@fau.edu Davide Nicolini (Warwick University) Davide.Nicolini@wbs.ac.uk Kajsa Lindberg (University of Gothenburg) kajsa.lindberg@gri.gu.se Petra Adolfsson (University of Gothenburg) petra.adolfsson@gri.gu.se Somewhat modified version of the paper presented at the International Management Division of the Academy of Management Conference August 2009, Chicago Abstract: Using a multiple case study approach, we compare retail pharmacy in four different countries-Sweden, Italy, UK, and USA. We draw on the concept of institutional logics to understand both the isomorphism associated with globalization and also the variety of organizational models observed in different countries. We identified characteristics associated with each of six sectors (markets, corporations, professions, states, families, and religions) and compared the typical model of retail pharmacy in each country with the ideal type for each logic. In contrast to most accounts of institutional change in the realm of globalization studies which have focused on the development of similar organizational forms across nation-states over time, we see that some local material practices and symbolic constructions are resilient. We conclude that different configurations of potentially conflicting logics help explain the models of retail pharmacy in the four different countries. Key words: institutional change; institutional logics; globalization Globalization may be taking us to a world where businesses look much the same in all geographic settings. On the other hand, in some settings, we continue to see striking differences in organizations when comparing across countries. We were struck by a situation of both similarities and differences in our international comparison of the business of retail pharmacy in four countries – Sweden, Italy, UK and USA (see Figure 1 for a reconstruction of the main historical events shaping pharmacy in the four countries). 1 AOM submission # 14103 Pharmacists (health professionals who dispense medications) hold similar qualifications throughout the western world, and their work practices of dispensing medications based on physician prescriptions is also very consistent. Pharmaceutical products themselves are developed, produced and distributed by very large multinational corporations such as Pfizer, and Merck. The product sold throughout the world is exactly the same. For example, a 10 mg. tablet of Valium looks the same and is of identical composition wherever it is sold. However, the pharmacy in which pharmacists work, and in which Valium or other pharmaceuticals are sold takes many different forms. In Sweden, pharmacies are part of a government owned monopoly, and pharmacists work as public sector employees. In Italy, pharmacies are independently owned by pharmacists and often ownership is passed on to family members. In the UK, pharmacies can be owned by pharmacists, a partnership of pharmacists, or a corporation. There is no limit to the number of stores that one individual, partnership or corporation may own, however, only a pharmacist may dispense prescribed pharmaceuticals. In the USA, there are no restrictions on ownership1. Similar to any other business, anyone with sufficient financial resources can own a pharmacy, but only a pharmacist may dispense prescribed pharmaceuticals. Institutional theory provides a framework for understanding both similarity and differences. It arose from a desire to understand why organizations were so similar to each other – the question of isomorphism (Meyer and Rowan, 1977; Scott, 2008). However, over the past decade institutionalists have become increasingly interested in understanding change. They want to understand how established institutions are broken down and replaced with new ones, or how systems move away from established norms 1 The one exception is the USA state of North Dakota where only a pharmacist may own a pharmacy. 2 AOM submission # 14103 and standards. Within this focus on institutional change, the concept of institutional logics (values and beliefs that guide behavior within a field) has played prominently. Theorists suggest that it is the transition of an organizational field from one guiding logic to another that underpins such change (Thornton and Ocasio, 1999; Thornton, 2004). We see that institutional theory and the concept of institutional logics provide potentially interesting and informative ways of understanding both the isomorphism associated with globalization and also the variety of organizational models observed in different countries. In this paper, we contribute to the institutional theory literature by drawing on relatively recent studies that point to the importance of not just one guiding logic, but multiple institutional logics and their collective impact on field level actors (Goodrick & Reay, 2007; Reay and Hinings, 2005; forthcoming; Thornton and Ocasio, 2008). We suggest that attention to the co-existence of multiple logics provides insights into processes of institutional change and the existence of both similarities and differences in organizational models when comparing across countries. We wanted to understand the similarities and differences among typical models of retail pharmacy in four countries. Retail pharmacy provides a very interesting setting to study these relationships because a number of important societal logics collectively shape the way in which pharmacy services are provided in different countries. For example, a logic of professionalism guides practices since pharmacists are highly educated professionals whose work is grounded in an exclusively held body of abstract knowledge. At the same time, the market logic also guides practices since financial sustainability of retail pharmacies depends upon selling pharmaceutical products. In addition, logics of state, corporatism, family and religion may also impact. 3 AOM submission # 14103 In the remainder of the paper we describe the current literature on institutionalist views of globalization, institutional change more generally, and the role of institutional logics. Next we briefly describe our four case studies of retail pharmacy with some attention to key historical events. We then explain our research methods and present our findings concerning the configuration of logics we observed in each country. Finally, we set out our discussion and conclusions. Background Literature: Comparative studies of business practices in different countries have a long history in management research. However, with the revival of institutionalism (neoinstitutional theory) in the 1970s, new approaches to globalization studies began to emerge. In particular, studies eventually labeled as “world society theory” (e.g. Meyer et al., 1975) brought two new approaches to understanding differences and similarities across countries. First, institutionalists brought attention to the “power of culture and norms in motivating social change,” and second they drew on “the notion of institutional isomorphism” to challenge “realist expectations that intrinsic needs and unique histories result in distinctive trajectories and features” (Drori, 2008: 452). Within this institutional tradition, researchers began to give particular attention to the characteristics of the place in which business practices occurred. Studies focused on the importance of different institutional principles as related to different structures that manifested those principles (Orrù, Biggart & Hamilton, 1991). And, globalization began to be considered not only as a process of adaptation to global conditions and pressures, but also as a process of institution building at the global level. In this way, globalization 4 AOM submission # 14103 came to be conceptualized as comprised of two complementary processes: (1) the diffusion of practices throughout the world, and (2) the development of global institutions with values and beliefs that could be shared by organizations around the world. (Drori, 2008) These concepts of globalization that rely upon not only diffusion of practices but also the transfer and sharing of values and beliefs are consistent with concepts of institutional change more generally and the role of institutional logics in guiding organizational behavior (Scott, 2008). Institutional logics are the organizing principles that shape the behavioral possibility of actors (Friedland & Alford, 1991). They exist at the societal level and are associated with each of the most important societal level orders -- market, state, democracy, family, and religion. Each societal sector is characterized by a central logic which is associated with “a set of material practices and symbolic constructions,” that is “available to organizations and individuals to elaborate” (Friedland & Alford 1991: 248). Institutional logics thus shape behavior by specifying which goals or values should be pursued within a given domain, and what actions, interactions, or interpretations are appropriate for the pursuit (Scott et al. 2000; Thornton 2004; Thornton & Ocasio 2008). Although earlier studies assumed that one dominant logic organized the behavior of all actors in an organizational field, there is now recognition that most fields are characterized by multiple logics. “Multiple frameworks are available within developed societies, which are differentiated around numerous specialized arenas – political, economic, religious, kinship, and so on – and each of which is governed by a different logic” (Scott, 2008: 186). As organizations or other actors negotiate their actions across 5 AOM submission # 14103 these arenas, they may be influenced by different logics. In addition, organizations may be able to draw on the different logics as resources in designing (or re-designing) their operations. The relationship between symbolic connstructions and material practices that constitute institutional logics is conceptually important in understanding institutional stability and change. We see that symbolic constructions and material practices are best viewed as two sides of a coin rather than two poles of a traditional reductionist opposition between materialism and idealism (Delmestri, 2008). Researchers have shown that changing institutional logics at the field level leads to altered practices of both organizational and individual actors (Hoffman, 1999; Thornton, 2004). At the same time, research also shows that changing practices of local actors may lead to modifications in institutional logics (Reay & Hinings, forthcoming). Understanding this relationship between symbolic systems and material practices is further complicated by relatively recent theorizing that many organizational fields are guided by multiple institutional logics rather than a single dominant logic. As Scott pointed out, “Multiple frameworks are available within developed societies, which are differentiated around numerous specialized arenas – political, economic, religious, kinship, and so on – and each of which is governed by a different logic” (Scott, 2008: 186). As organizations or other actors negotiate their actions across these arenas, they may be influenced by different coexisting and possibly competing logics. In these settings, material practices (and changes in these practices) may be best understood in relationship to an intertwined grouping of institutional logics that may also be changing. 6 AOM submission # 14103 In this paper, we take the position that institutional change and processes of globalization can best be understood by focusing on the dynamics between or among institutional logics and also by giving attention to how these logics are materialized in observable organizational behavior. We attempt to better understand how processes of institutional change can lead to both similarities and differences in different national settings through our empirical comparative study of retail pharmacy in four different countries – Sweden, Italy, UK and USA. Case Studies We used a multiple case study approach to investigate similarities and differences in the way that pharmacy services are organized in four different countries. Here we provide a short description of each case. Sweden: In Sweden, pharmacies were privately owned from the 17th century until 1970. Then, in 1971 the pharmacy system was nationalized and the state took over ownership of all pharmacies. Pharmacists became public employees. Since that time, the stateowned company, Apoteket AB, has held the exclusive right to engage in drug retailing. The state also controls the price of prescribed pharmaceuticals, since they are considered an integral component of the public health system. Residents receive a tax-based system of pharmaceutical benefit. In 2002, a new agency was appointed by the government to determine which pharmaceuticals are reimbursable and to set prices that patients pay. Pharmacies are not established to make a profit. They are in place to provide a health service. This description of pharmacy practices accurately represents the current situation; however, Economic Union (EU) anti-competition concerns are soon to be 7 AOM submission # 14103 addressed through a new (but not yet established) way of organizing that will move away from completely state-owned pharmacies. Italy: In the past, the most prevalent form was “one pharmacist, one pharmacy.” Going back to the early 19th century, laws precluded pharmacists from owning more than one pharmacy. Since then some constraints have been altered. Pharmacies ownership remains limited to pharmacists, but may be transferred relatively easily to a family member or (with more restrictions) another pharmacist. Currently, one pharmacist may own only one pharmacy, and up to four pharmacists may create a partnership that owns up to four pharmacies. In addition, because the government considers the pharmacy to be a public service, pharmacists have the opportunity to personally obtain a charter by winning open publicly regulated competitions. Currently, the municipal and cooperative pharmacies account for approximately 10% of pharmacies, while privately owned pharmacies are the rule. Regardless of ownership, the government continues to limit the number and location of pharmacies. The price of pharmaceuticals has been determined by state authorities since 1240, and traditionally medicine has been distributed for free to the poor. In 1978, with the institution of a national health care system, pharmaceuticals became fully reimbursable as a right of citizenship. The Italian government has taken, and continues to take a strong role in managing the overall pharmacy system, but relies on individual pharmacists as owners and business operators of individual pharmacies. UK: Since 1880, any private investor has been allowed to own a pharmacy provided that the dispensing activity is carried out by a licensed pharmacist. Thus a pharmacy may be 8 AOM submission # 14103 owned by any individual, partnership or corporation. While the government does not regulate or limit the number of pharmacies, it does control the number of contracts with pharmacies which dispense reimbursable drugs. This means that pharmacies with a contract receive full reimbursement from the National Health Service (NHS) for all prescribed pharmaceuticals dispensed. Pharmacies without a contract would have to charge the full price to consumers. In recent years, NHS contracts have been used to prevent extreme forms of competition and to preserve some of the independent pharmacies. Currently in the UK, the price of reimbursable pharmaceuticals was resolved through a Government-Industry agreement. Until the early 1900s, the price of pharmaceuticals was left to market forces, but in the 1950s, a series of mechanisms were introduced and resulted in almost complete government price control. These mechanisms have been relaxed over time, but now, UK consumers pay a very low, set fee for any ‘reimbursable’ prescription. USA: Ownership of pharmacies is not restricted. Anyone may own a pharmacy, but only a pharmacist is allowed to dispense pharmaceuticals. Prior to the 1920s there was no legal restriction on ownership. As chain drug stores began to proliferate, some states restricted ownership to pharmacists. A 1928 Supreme Court decision ruled that state laws were unconstitutional; anyone could open a pharmacy if they had sufficient means to do so. The owner was required to hire a pharmacist if they did not hold the credentials. In 1973, the Supreme Court decision was overturned, with the result that states could restrict ownership. However, since then, only one state (North Dakota) has chosen to restrict pharmacy ownership to pharmacists. Most pharmacies are a small component of a much 9 AOM submission # 14103 larger store where many other products (e.g. groceries, household goods, cosmetics) are also sold. Following a free market principle, pharmaceuticals have been treated as a normal good, with the price determined through mechanisms of supply and demand. Private insurance plans (usually through employers) pay the cost of pharmaceuticals with a moderate portion paid directly by the consumer. Recently, the federal government pays partial costs for those citizens 65 and older. Government insurance also provides limited coverage for the poor. Since insurance plans are discretionary for employers, not all citizens are covered. Insurance companies negotiate price with suppliers but overall costs to consumers are higher than in most other countries. In the USA, the government role has primarily been to provide regulations with regard to safety standards and the maintenance of a relatively free-market system. Research Methods: We followed a modified content analysis (Krippendorf, 2004) by using analytic categories developed from concepts outlined by Friedland and Alford (1991) and Thornton and Ocasio (2008). For each of our four case studies, we analyzed archival records, professional publications, government statistics and other publications. We also visited typical pharmacies in each country. Based on all data sources, we identified characteristics associated with each of six sectors (markets, corporations, professions, states, families and religions) – each with its own distinct logic (Thornton, 2004). Using the concept of ‘ideal type’ (Freidson, 2001; Thornton, 2004) we developed a description of how the field of retail pharmacy would be organized if that sector (with its distinct logic) organized the field. For example, if the market sector exclusively organized the 10 AOM submission # 14103 field of retail pharmacy, the observable material practices would be: unrestricted ownership, signs of outlets emphasizing brand distinctiveness, pricing of products based on principles of demand and supply, product content uncontrolled, no restriction on who dispenses medications, and absence of external subsidies for consumers. The above listed characteristics describe the ideal type for the market logic. (The ideal type for each of the other five logics is described in Table 1 by the list of characteristics recorded in the first column.) [Table 1 about here.] Then, for each sector (logic) and based on our description of the ideal type, we evaluate the ‘closeness to ideal type’ for each characteristic in each case (Sweden, Italy, UK and USA). This means that we compared the observed typical model of retail pharmacy in each country with the ideal type for each logic. This evaluation required that all members of our research team from different countries used their individual and collective knowledge of each case to develop an agreed upon ranking. Each ranking is based on a five point scale where 5 = very close to ideal type, and 1 = not at all close to ideal type. Table 1 shows our evaluations of closeness to ideal type for each characteristic in each geographic setting. For ease of discussion, we have summarized these evaluations to develop an overall rating (high, moderate or low) of the relative strengths of each logic in each country. These ratings are indicated in Table 2. [Table 2 about here] In addition to these evaluations, we also draw on the history of pharmacy in each country to understand changes as they have occurred over time. To get a better understanding of the field, we further analyzed each critical event presented in Figure 1. 11 AOM submission # 14103 (In this version of the paper, we report on only one selected event for each case study. We focus on the most recent event with significant implications that can be observed.) Following the literature that conceptualizes institutional logics as realized in material practices (Friedland & Alford, 1991; Thornton, 2004; Thornton & Ocasio, 2008) and with particular recognition of the inherent duality of logics and practices (Delmestri, 2009; Mohr & Duquenne, 1997), we developed a coding scheme to record: (1) the nature of the problem associated with the critical event, (2) a description of how the problem was raised to the field level, (3) the way in which the problem was resolved, and (4) the material practices evident in the field after the resolution. (See Table 3 for a summary.) We then used this information to understand how conflict among multiple logics within each field arose, was elevated to a level where resolution became critical, and how the resulting practices reflect the new arrangements under which logics co-exist. Based on our knowledge of retail pharmacy in each country, we focused on three societal level logics that we believed to be most relevant across the four cases – the market, professional and state logics. In addition to understanding this process within each field, we also attempt to draw further conclusions from comparisons of patterns identified across cases (Stake, 1995). Findings: Configurations of Logics Based on our ratings of the strength of each logic, we developed a snap-shot view of the set or configurations of logics associated with the typical model of retail pharmacy in each country. In each setting we observed that more than one logic was rated at moderate or strong, a finding that is consistent with other studies that highlight situations 12 AOM submission # 14103 where more than one dominant logic guides behavior in a field (Goodrick & Reay, 2007; Reay & Hinings, 2005; forthcoming). In this section we describe the configuration of logics guiding typical retail pharmacy practices in each country. Sweden We rated the configuration of logics associated with the typical model of retail pharmacy in Sweden as: State = high; Professional = moderate; and Corporate = moderate. There are only small indicators of a market approach, and there is no evidence that the church or family logics are relevant. In Sweden, the state influence is strong since pharmaceutical services are viewed as an integral component of the publicly funded health care system. All pharmacies are operated by the state-owned corporation, Apoteket AB. This company currently holds the exclusive right to sell pharmaceutical products in Sweden, although this arrangement will likely be modified based on recent rulings by the EU. We also evaluated the state logic as highly influential because the consumer price of pharmaceuticals is determined based on socially acceptable standards, and kept low as part of overall government objectives to maintain the health of the population. Low-income citizens receive medications at no cost. Similar to all countries we studied, the government takes responsibility for ensuring the quality of pharmaceutical products. In addition to the strong influence of the state logic, we also rated the influence of the professional and corporate logics as moderate. The professional association for pharmacists controls educational and entry-to-practice standards. The dispensing of pharmaceutical products is restricted to licensed pharmacists, although pharmacy technicians may dispense a limited number of products. Even products that are freely 13 AOM submission # 14103 available in many other countries (Over-the-counter pharmaceuticals – OTCs – such as Tylenol or cold remedies) have been available only in pharmacies. Even though Apoteket is state-owned, it does operate on a corporate model with bureaucratic structures and reporting relationships. Pharmacists must work within this corporate structure, and receive a relatively low salary (Lindberg & Adolfsson, 2007). A visit to a typical Apoteket pharmacy provides the following view. Pharmacy outlets have outside signage showing a stylized green caduceus (a winged staff entwined by two snakes) followed by the name of the company (Apoteket), and the name of the city of neighborhood where the pharmacy is located. Inside the store, many products (cosmetics, herbal remedies and personal products) are displayed in easily accessible shelving, and sales personnel walk about in this open area of the shop. Pharmacists and pharmacy technicians are easily available to provide information about products, and also dispense controlled medications from behind the counter. Displays inside the pharmacy are often related to health maintenance products and provide a strong sense of professionalism. Italy Our evaluation of the configuration of logics associated with the typical model of retail pharmacy in Italy is: Professional = high; State = high; and Family = moderate. There are few indicators of a market or corporate approach, and at this point in history, there is no longer evidence that the religious logic is relevant. We rated the influence of professionalism as high because ownership of pharmacies is restricted to pharmacists. The professional association sets educational 14 AOM submission # 14103 standards and determines appropriate qualifications for entry to practice. As in other countries, dispensing of pharmaceutical products is also restricted to pharmacists, however, in Italy, even OTC pharmaceutical products must be sold by pharmacists. The influence of the state logic is also high. Pharmaceuticals are considered to be an important component of publicly provided health services. As such, the cost of medication is reimbursable from the government for all citizens. The government controls the number of pharmacies in any community by granting only a limited number of pharmacists the right to operate a pharmacy. In Italy, the family logic remains moderately influential in the typical model of retail pharmacy. The majority of pharmacies are passed on from father to son (or daughter). Regulations on ownership favor the transfer to a family member – even if the family member does not currently hold the appropriate qualifications as a pharmacist. Special provisions allow time for the family member to become educated as part of ownership transfer process. The owner of the pharmacy typical hires other family members (including non-pharmacists) to work in the store – making the pharmacy a typical family business, strongly guided by family principles. A customer visiting an Italian pharmacy will see consistent signage on the outside of the building with a green cross and the word, “Farmacia.” In addition, the title and name of the owner-pharmacist is displayed, often signaling the name of a traditional family that has owned the outlet for decades or even centuries. Inside the pharmacy, displays tend to be focused on pharmaceutical or other health-based products. Stores are relatively small, with displays of cosmetic or herbal products in the open area. The pharmacist must be on-site for all sales of pharmaceutical products, and if he or she is 15 AOM submission # 14103 absent for any period of time, customers must return later to pick up their prescription or OTC purchase. Very recently, new regulations allow that OTC products may be purchased in supermarkets, but only in a section of the store specifically designated for OTCs, and only with the assistance of a pharmacist to put the medication into the consumer’s shopping cart. UK Our evaluation of the configuration of logics in a typical UK pharmacy is as follows: State = high; Corporate = high; Professional = moderate; Market = moderate. The family and religious logics do not hold observable influence. We rated the influence of the state logic as high because pharmaceuticals are considered an important part of the National Health System (NHS). All citizens receive prescribed medications for a small flat fee (approximately ₤7). Although the government does not own pharmacies, the number of pharmacies holding a contract with the NHS is limited. Pharmacies could operate without an NHS contract, but they would then be forced to recover the full cost of medications from consumers. This effectively limits the establishment of a pharmacy to those with an NHS contract. As in other countries, the government also plays a strong role in setting standards for the quality of pharmaceutical products. We also rated the influence of the corporate logic as high. Ownership of a pharmacy (or pharmacies) may be by a person, partnership or corporation. In effect, this has translated in 2007 into about 60% of pharmacies being multiples, i.e. owned by corporate chains. In particular, Boots owns more than 50% of all pharmacies in the UK. 16 AOM submission # 14103 This large corporate ownership of pharmacies means that bureaucratic systems and structures prevail. Most pharmacists work as employees of a corporation such as Boots, and corporate management of stores is the norm. The configuration of logics we identified for UK pharmacies also includes moderate influence from the professional and market logics. The professional association of pharmacists controls educational standards and manages eligibility criteria. Only pharmacists can dispense prescribed medications, but the list of OTC products is relatively large and these products may be sold in any store by anyone. The influence of the market logic is also evident because unrestricted ownership means that anyone can open a pharmacy, and in some parts of the country ownership is relatively diverse. Pharmacy owners do operate based on profitability criteria, although the market is definitely skewed by NHS coverage for the cost of most medications (Anderson, 2005; Silcock et al., 2004). A visit to a typical UK pharmacy would show a relatively large store with corporate signage on the front of the premises indicating the name of the corporation (or individual owner). Inside the pharmacy, a large number of cosmetic, personal hygiene, and OTC products are displayed in multiple rows of shelving. The pharmacist counter is usually set prominently near the front of the store, and often features a queue of people waiting to have their prescription filled. Displays within the store are focused on both healthy living advice, and also advertising for personal products such as shampoo or cosmetics. USA 17 AOM submission # 14103 We rated the typical model of retail pharmacy in the USA as: Market = high; Corporations = high; Professions = moderate and State = moderate. In contrast to the other countries studied, we observed that the market logic holds a strong influence in organizing the typical model of retail pharmacy in the USA. Pharmacy ownership is unrestricted, which means that anyone can operate the business even though only a pharmacist can dispense medications. This was determined in 1928 when the US Supreme Court ruled that states could not restrict ownership of retail pharmacies in the same way that they could not restrict ownership of other business (U.S. Supreme Court, 1928). Also consistent with the ideal type of the market logic, prices of pharmaceutical products are determined by supply and demand without government interference. There are few subsidies available for consumers, although recent changes to Medicare programs provide government support for senior citizens. Even though the market logic strongly influences the model of retail pharmacy, some aspects of retail pharmacy are not consistent with the market logic. The quality of pharmaceutical products is controlled by government – not the market. The bargaining power of insurance companies influences the price paid for pharmaceuticals. And although there are a large number of OTC medications that can be sold by anyone, most pharmaceuticals can only be sold to consumers by a licensed pharmacist. We also found that the configuration of logics associated with retail pharmacy in the USA included strong influence from the corporate logic. Almost all pharmacies are owned by corporations, and unlike the European model, names of pharmacists are not prominently displayed. This situation has changed dramatically since the 1950s when 52% of pharmacies were owned by independent pharmacies. Currently, less than 3% of 18 AOM submission # 14103 pharmacists report being self-employed (Mott et al., 2000). The professional and state logics also contribute to the configuration of logics since dispensing of medications (other than OTCs) is restricted to pharmacists who have been educated in accordance with standards determined by the professional association. And the state logic is also important because the quality of medications is highly regulated by government authorities, and increasingly the government is involved in programs to provide pharmaceuticals to senior citizens (CMS, 2009). Currently, neither the family logic nor the religious logic influence the model, but in the first half of the 20th century, family ownership of pharmacies was common (Kremers et al., 1963). Churches have not taken a role in pharmacy practice in the history of the USA. The picture of a typical pharmacy in the USA is very strongly connected to the market logic. Most pharmacies are very large stores where many other products (in addition to pharmaceuticals) are sold. The two largest chains have 4,000 stores each and dispense 41% of total prescriptions sold (U.S. Department of Health and Human Services, 2000). Pharmaceutical sales typically occur at the back of the store, where a pharmacist and technicians work behind a locked counter to fill prescriptions and dispense medications to customers. Inside and outside store displays indicate the corporate brand (e.g. Walgreen’s) and often indicate bargain prices available on merchandise other than pharmaceuticals. For example, front door signage commonly announces sale prices on soft drinks, snack foods or toiletries. Retail pharmacies in the USA provide an image of a place where consumers go to purchase a wide variety of products. They may or may not purchase pharmaceuticals in their store visit. 19 AOM submission # 14103 To summarize by comparing across cases, we observed different configurations of logics in each country we studied. The model of retail pharmacy in the USA is particular influenced by the market logic, but also by logics of corporatism, professionalism and the state. The model in the UK is closest to that of the USA with strong influence from the corporate logic but also from the state logic, and only moderate influence from the market and professional logic. In Sweden the influence of the state is very high since pharmacies are operated by a state owned corporation that holds a monopoly for pharmaceutical services. In addition, the professional and corporate logics influence the model. And finally, the Italian case is somewhat different. In this configuration of logics, the professional and state logic are high in influence together with moderate influence from the family logic. Discussion and Conclusions: We view the pharmacy as a place to observe how institutional logics become materialized in a locally sustainable model of retail pharmacy. Since the pharmacy is the location where patients (consumers) take possession of medications, it is a physical space where the intersection of multiple institutional logics becomes more visible. In each country we examined, there was significant influence from a number of potentially competing logics and the tension among those logics was resolved in different ways. The model of retail pharmacy in the USA is the most influenced by the market logic. This finding is not surprising given that the USA is the only one of our cases where market principles organize the provision of health care more generally. The strength of the market logic is observable not only in the pricing mechanism for pharmaceutical 20 AOM submission # 14103 products (demand and supply), but also in the wide variety of products sold in a typical US pharmacy. Owners of pharmacies are businessmen and as such they sell products on which they can make a profit. Some products are pharmaceuticals, but many are not. However, even though the market logic is strong in the USA it does not explain other components of the model. Quality assurance of pharmaceutical products is not left to market forces – it is highly controlled by government agencies. And the logic of professionalism (not the market logic) explains the requirement that only pharmacists dispense prescribed medications. Thus we see that a configuration of logics (that might otherwise be considered competing logics) collectively influence the observed model. We have used the USA case as an example, but in the other three cases, we similarly find that the influence of a number of logics is evident. We draw on this concept of a configuration of logics to better understand processes of institutional change that result in both similarities and differences in retail pharmacy across countries. Most accounts of institutional change in the realm of globalization studies focused on the development of similar organizational forms across nation-states over time including the globalization of health (Inoue & Drori, 2006). In contrast, our study suggests that some local material practices together with their symbolic justifications may be more resilient than others. For example, across our four cases, we see the standardizing influence of professional pharmacists – even when they are paid by the state (Sweden) compared to those in the USA who receive relatively large salaries based on highly profitable pharmacy sales. But at the same time, we see continued adherence to market-based pricing (USA) and equally strong adherence to nonmarket, flat fee consumer prices (UK). This suggests that some components of a state 21 AOM submission # 14103 logic may be strongly evident, while other components are not. Overall, we see that the dynamics among institutional logics and material practices involve both continuity and change. From an institutional perspective, globalization consists of two processes of change – (1) global institutionalization of world society through global organizations and (2) the diffusion of established models from one national setting to another (Drori, 2008). These processes are considered to be complementary, but how they co-exist has not been fully addressed. The theoretical construct of a configuration of logics provides a framework for understanding how both processes can occur simultaneously – perhaps existing as complementary to each other, but also potentially in competition with each other. For example, we see that the strength of the professionalism logic is moderate or high in each of the countries we studied. Its universal strength may be explained by the existence of global organizations such as international pharmacy associations, or global pharmaceutical manufacturers. In addition, societal trends have been toward standardization to protect patient safety with the diffusion of professional models of health care as one component (Inoue & Drori, 2006). However, global standards may come into opposition with local preferences or long-established traditions such as family ownership of pharmacies in Italy. In this country, we can explain the co-existence of potentially conflicting logics of family and professionalism through a configuration of logics that balances and accommodates principles of family ownership with the global necessity of professional standards. Based on our historical data sources, we see that changes in national models of retail pharmacy shift over time in association with alterations in the configuration of 22 AOM submission # 14103 logics. Logics that were a strong component of the configuration at one point in time, became less significant or in some cases almost irrelevant at a later date. For example, in the early history of Italian pharmacies, the church played a very strong role with monks compounding medications and distributing them to those in need – a practice prohibited only in the late 19th century by a young Italian state in the struggles to establish itself in front of delegitimizing attacks by the Vatican authorities. Today, the church plays no role in pharmacy and discussion of a religious logic seems inappropriate. Similarly, in the USA during the somewhat lawless settling of western areas, pharmaceutical products were concocted by anyone and sold to those who would buy. The practices were fully consistent with a free market logic. Over time, government standards were introduced, ownership of pharmacies was restricted and then unrestricted, and most recently, government subsidies for some population segments have been introduced. Although pharmacy practices in the USA are more closely aligned with the market logic than in other countries studied here, they are much less aligned now than they were in the past. Both of these examples show the concept of a configuration of logics may help to explain gradual shifts (continuous change) because within the grouping of logics, changes in one logic may be compensated for or buffered by alterations in other logics. Our attention to the role of historical events also points to the importance of what Schneiberg (2007) labeled as flotsam and jetsam. We observed that previous events held ongoing significance to the constellation of logics, even when those events were temporally distant and not logically related. For example, in Italy the historical importance of family dynasties in many areas of business means that sustaining family ownership of pharmacies is viewed as a very appropriate government strategy. Also, in 23 AOM submission # 14103 the USA, previous legal and regulative battles that were fought over the importance of free-market principles have left indelible patterns leading decision-makers to adopt stances in support of free-market principles for pharmacies. We believe that more attention to the importance of previous events (often not in the same industry) may help to uncover important insights about the resilience of certain models in some countries. In this paper, we have drawn on the concept of a configuration of logics (Goodrick & Reay, 2007) to understand how institutional changes may result in worldwide similarities but also differences. Our content analysis of archival data, historical information and personal observations has allowed us to consider how the arrangement of potentially conflicting logics may influence models of retail pharmacy in four different countries – Sweden, Italy, UK and USA. This work contributes to previous institutionalist approaches to understanding globalization, and also to institutional theory and the role of institutional logics. We hope that further investigations in different industries will build on our work. References Anderson, S. 2005. Making Medicines: A Brief History of Pharmacy and Pharmaceuticals. Pharmaceutical Press. Centers for Medicare and Medicaid Services (CMS), Prescription Drug Coverage General Information. http://www.cms.hhs.gov/prescriptiondrugcovgenin/ Retrieved January 13, 2009. Delmestri G. (2008): Institutional Streams, Logics and Fields. Research in the Sociology of Organizations, 26, forthcoming. 24 AOM submission # 14103 Drori, G.S. 2008. ‘Institutionalism and Globalization Studies’. In Greenwood, R., Oliver, C., Sahlin, S. & Suddaby, R. (Eds.), Sage Handbook of Organizational Institutionalism: 449- 472. Freidson, E. 2001. Professionalism: The third logic. Chicago: University of Chicago Press. Friedland R. & Alford, R, R.. 1991. Bringing society back in: Symbols, practices, and institutional contradictions. In W. W. Powell & P. J. DiMaggio (Eds.), The new institutionalism in organizational analysis: 232-263. Chicago: University of Chicago Press Goodrick, E. & Reay, T. 2007. Multiple Logics in the Field of Pharmacy. Presentation at Academy of Management Meeting, Philadelphia, PA, August. Hoffman, A.J. 1999. Institutional evolution and change: Environmentalism and the U.S. chemical industry. Academy of Management Journal, 42//4: 351-371. Inoue, K. & Drori, G.S. 2006. The global institutionalization of health as a social concern. International Sociology, 21(2): 199-219. Kostova, T., Roth, K. and Dacin, M.T. 2008. ‘Institutional theory in the study of multinational corporations: A critique and new directions’, Academy of Management Journal 33(4): 994-1006. Kremers, E, Urdang, G., and Sonnedecker, G. 1963. Kremers and Urdang’s History of Pharmacy. 3rd edition. J.B. Lippincott Company, Philadelphia. Krippendorf, K. 2004. Content Analysis. Thousand Oaks: Sage. Lindberg, K. & Adolfsson, P. 2007. The evolution of Swedish pharmacies and recent reforms. Working Paper GRI – rapport 2007: 5. Gothenburg Research Institute. Gothenburg University. Meyer, J.W., Boli-Bennett, J. & Chase-Dunn, C. 1975. Convergence and divergence in development. Annual Review of Sociology, 1: 223-246. Meyer, J.W. & Rowan, B. 1977. Institutionalized organizations? Formal structure as myth and ceremony. American Journal of Sociology, 83: 440-463. Orrù, Biggart & Hamilton, 1991. Organizational Isomorphism in East Asia. In W. W. Powell & P. J. DiMaggio (Eds.), The new institutionalism in organizational analysis. 25 AOM submission # 14103 Reay, T. & Hinings, C.R. 2005. The recomposition of an organizational field: Health care in Alberta, Organization Studies, 26(3): 349-382. Reay, T. & Hinings, C.R. forthcoming. ‘Managing the rivalry of competing institutional logics’, Organization Studies. Schneiberg, M. 2007. What’s on the path? Path dependence, organizational diversity and the problem of institutional change in the US economy, 1900-1950. SocioEconomic Review, 5, 47-80. Scott, W.R. 2008. Institutions and Organizations, 3rd edition. Thousand Oaks: Sage. Scott, W.R., Ruef, M., Mendel, P.J. & Caronna, C.A. 2000. Institutional change and healthcare organizations. Chicago: University of Chicago. Silcock, J., Raynor, D.K. & Petty, D. 2004. The organisation and development of primary care pharmacy in the United Kingdom. Health Policy, 67, 207-214. Thornton, P. 2004. Markets from Culture. Stanford University Press. Thornton, P.H. and Ocasio, W. 2008. ‘Institutional logics’, In R. Greenwood, C. Oliver, K. Sahlin, and R. Suddaby (Eds), Sage Handbook of Organizational Institutionalism: 99-129. Thousand Oakes, CA: Sage Publications U.S. Supreme Court. 1928. Louis K. Liggett Co v. Baldridge, 278 U.S. 105. 26 AOM submission # 14103 Table 1: Closeness to ideal type by logic and by typical pharmacy type in country (1= not at all close to ideal type; 5= very close to ideal type) Institutional logic (characteristics of ideal type) Markets Ownership unrestricted Prices set by demand/ supply Inside & outside displays emphasize brand distinctiveness Product content unregulated No restrictions on who dispenses drugs No subsidies for consumers Corporations Corporate ownership Prices set to maximize corporate profit Inside & outside displays signal corporate distinctiveness Product content determined by corporation Corporation determines who dispenses drugs Corporations may subsidize some consumers (e.g. seniors) Professions Pharmacist ownership Prices set to give pharmacists fair salary Inside & outside displays signal professional affiliation Product content assured by pharmacist Only pharmacists dispense drugs Sweden Italy UK USA 1 2 1 1 5 1 5 5 2 1 5 5 1 1 1 1 1 1 2 2 1 1 1 4 3 1 1 1 4 2 5 5 3 1 5 5 1 1 1 1 1 1 1 1 1 1 1 1 1 1 5 1 2 1 1 1 3 5 1 1 1 1 1 1 4 5 4 4 27 AOM submission # 14103 Pharmacist chooses to subsidize some consumers (or not) States State ownership Prices set based on public social welfare Inside & outside displays signal affiliation with state Product content assured by state regulations State dispenses drugs directly to patients State subsidizes consumers unable to pay Families Family ownership Prices set by family owners Inside & outside displays signal family presence Product content assured by family owners Families determine who dispenses drugs Family owners choose to subsidize consumers Religions Church ownership Prices determined by church officials Inside & outside displays signal religious affiliation Product content assured by church officials Church dispense drugs Church chooses to subsidize some consumers (e.g. poor) 1 1 1 1 4 5 1 5 1 5 1 1 1 1 1 1 5 5 5 5 1 1 1 1 5 5 5 2 1 1 5 1 1 1 1 1 1 2 1 1 1 1 1 1 1 2 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 28 AOM submission # 14103 Table 2: Overall rating of logic strength (closeness to ideal type) in each country (present times) Logic Market Corporate Professional State Family Religion Sweden Low Moderate Moderate High Low Low Italy Low Low High High Moderate Low UK Moderate High Moderate High Low Low USA High High Moderate Moderate Low Low Country 29 AOM submission # 14103 Table 3: Selected problems, resolutions and practices The problem How problem gained importance at field level How problem was resolved Description of practices at resolution Sweden 1970 How should the government ensure that pharmacies were located appropriately in urban and rural areas to meet citizens’ need for access to pharmaceuticals? Government and health officials became concerned with increasing numbers of independently owned pharmacies that tended to be clustered in urban areas. Government took action to meet health needs of citizens. Negotiations between the government and the association of pharmacy owners resulted in the decision to nationalize all pharmacies through establishment of Apoteket AB. Italy 1968 Who can own a pharmacy, and do they have the right to sell their pharmacy? And what role should pharmacists take in the health system? Political parties negotiated a compromise agreement that led to legislation establishing: (1) pharmacists’ responsibilities as quasi public health officers, (2) pharmacy ownership by right of a personal license, tradable only once in a lifetime and inheritable by family members who could have time to gain certification as a pharmacist. UK 2003 How should NHS contracts with community pharmacies be controlled? Discussion of pharmacy ownership was framed around survival of rural pharmacies and the future identity of the pharmacist as a business owner or public officer. Different arguments made by different key actors: pharmacy owners association, pharmacy employees association, and main political parties (Christian Democrats, Socialists, Communist Party & MSI. Question was whether to make pharmacists public officers or maintain non-tradable personal license arrangement. Office of Fair Trading recommended an end to controls limiting numbers of NHS contracts for new community pharmacies. All pharmacies owned by government corporation, Apoteket. Any profits are held by Apoteket. Location, hours of operation, etc. controlled by govt. Pharmacists and others are government employees. Prescription drugs dispensed only by pharmacists. OTC drugs sold only in pharmacies. Pharmacies owned by a pharmacist or cooperatives of pharmacists. Any profits are held by owner. The number and location of pharmacies are controlled by government. Prescription drugs dispensed only by pharmacists. OTC drugs sold only by pharmacists. Government decision: modify entry control regulations rather than abolish them. Health authorities monitor number of pharmacies with an NHS contract, and Pharmacy owned by any individual or corporation. 55% pharmacies belong to chains. Any profits held by owner. Pharmacies are integrated with health 30 AOM submission # 14103 decide whether new applications for a contract will be granted. USA 1928 Should ownership of pharmacies be restricted to pharmacists? New York corporation with three stores challenged Pennsylvania State Law restricting ownership of new pharmacies to registered pharmacies or corporations in which all members were pharmacists. State court supported restrictive ownership. 1928 Supreme Court ruled that there was insufficient evidence that nonpharmacist ownership of a pharmacy would threaten public health safety. The risk did not warrant restriction of private business. Therefore, no restrictions could be placed on pharmacy ownership. system through NHS reimbursements & health authority control over contracts. Prescription drugs dispensed only by pharmacist. OTC drugs sold in controlled retail settings. Pharmacies can be owned by any individual or corporation. 61% of pharmacies belong to chains. Pharmacies operate as businesses (as opposed to as part of a health care system) and are reimbursed primarily through private insurance and copays. Prescription drugs dispensed only by pharmacist. OTC drugs sold in any retail establishment as well as in vending machines. 31 AOM submission # 14103 Figure 1: Critical problems and resolutions over time in the four countries 32 AOM submission # 14103 33