BS3050 Diet

BS3050 Physiology of Sport and Exercise
Nutritional Requirements for Sport and Exercise
Aims: to explain the fundamental nutritional requirements for energy supply and the rationale underlying the use of dietary supplements to enhance exercise performance
Learning outcomes:
An understanding of the dietary requirements for carbohydrate, protein and fats in the normal individual and in athletes
An understanding of the effectiveness and proposed mode of action of selected commercially available dietary supplements on athletic performance, including amino acid supplements, creatine, caffeine, bicarbonate, medium-chain triglycerides,
-Hydroxy
-methyl butyrate,
L
-carnitine
Meeting energy requirements
The energy requirements of an individual vary but in general the BMR (basal or resting metabolic rate) accounts for 65 – 75 % of the total energy expenditure (about 20% of this –
1760 kJ is from the 120 g glucose consumed by daily the brain!); thermogenesis accounts for about 10%, while physical activity accounts for 15 –30 % of total energy expenditure.
Sedentary females have a daily energy expenditure of 8,400 - 10,500 kJ whilst males require
10,500 – 12, 500 kJ. Regular exercise increases this by about 30% whilst elite athletes will require double the intake.
Energy can come from a number of different dietary sources with fat yielding 39 kJ/g, more than twice as much as protein (17 kJ/g) and carbohydrate (16 kJ/g) but as I explained last week the energy from carbohydrate is more immediately available particularly when compared to fat.
Strategies to optimise performance and speed recovery
Meeting the energy demands of exercise and maintaining body mass and body fat at optimal levels are the key goals of an athlete in training. Individuals must have strategies for refuelling and re-hydrating during and between bouts of exercise. They must be able to do this without experiencing detrimental side-effects such as gastro-intestinal discomfort. It is not the intention to discuss the requirements for vitamins and ions such as iron, calcium and zinc, which are also important components of the diet, but to concentrate on the energy providing components.
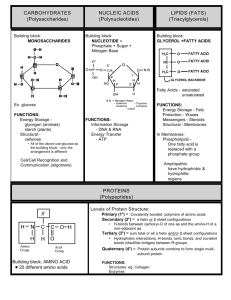
Carbohydrate
Before or between bouts of heavy training it is important to increase muscle glycogen deposition which can mean the intake of between 7 and 10 g /kg body weight of carbohydrate per day
To enhance recovery eat a high carbohydrate meal or snack within 15 –30 min of an event to help replete the glycogen stores and to keep topping up the carbohydrate at 30 min intervals for about 5 hr after exercise. This appears to be better than waiting for several hours
In long term events is advisable to consume carbohydrate during the event. This is usually in the form of a sports drink containing sugars which will supply the carbohydrate and fluid needs simultaneously. Restoration of fluid and electrolyte balance is essential.
Monosaccharides such as glucose, fructose and galactose are readily absorbed and the two latter are readily converted to glucose by the liver and released into the bloodstream before
they can be converted to muscle glycogen. Disaccharides such as sucrose and maltose are hydrolysed to their monosaccharide components whilst the plant starches amylose and amylopectin , need to be hydrolysed to maltose by intestinal amylase before they can be absorbed and utilized.
Carbohydrate loading : This is a method of building up glycogen levels prior to an endurance competition It involves a low carbohydrate diet combined with steady exercise to lower the muscle glycogen over a few days a week or so before the competition. The athlete switches to a high carbohydrate diet (4-700 g/day) 3 days before the competition. The affected muscles overcompensate for the lack of glycogen and build up a higher than normal level of glycogen – up to about 4%. This is only useful for events that involve depletion of glycogen i.e. intense aerobic activity lasting an hour or more. However endurance training also builds up the capacity for glycogen replenishment anyway, which diminishes the carbohydrate loading effect in highly trained athletes. One problem is that additional water
(2.7-g water/g glycogen) is stored along with this glycogen and the athlete can feel that the muscles are heavy – negating any positive benefits from glycogen loading.
Protein
Although the protein requirement of athletes are greater than those of sedentary individuals because the amino acids are required for the repair and recovery of damaged muscle and the generation of new muscle when required. It is about 1.2 –1.8 g/kg for a trained athlete i.e. much less than for carbohydrate. It is important that the protein diet supplies the eight essential aminoacids (i.e. those which cannot be synthesised in the body – His, Iso, Leu, Lys,
Met, Phe, Thr, Try, Val) Most individuals will have no difficulty in meeting this dietary requirement, the main problem for carnivores is that the protein is the diet is accompanied by a considerable level of fat (e.g. red meat, the hard cheeses etc.); and for vegans it is important that the protein is derived from a variety of sources to supply the essential amino acids
.
Fats
It is recommended that the fat content of an athlete's diet should be about 25%
It is very difficult to avoid fats in most diets most athletes will consume more than they require. Having said that essential fatty acids (linoleic and linolenic acids) of vegetable origin are essential part of our diets.
Commercial dietary supplements as aids to training and performance
There is a huge commercial industry dedicated to claims that various dietary supplements provide ergogenic benefits (i.e. act to improve physical work capacity or athletic performance). Some of these are effective and have a scientific basis but with others the benefits are less clear and indeed may be ineffective. I will not discuss pharmacological ergogenic aids such as the anabolic steroids, amphetamines, diuretics,
-blockers and peptide hormones which will be discussed later in the course.
The definition of a dietary supplement covers vitamins, minerals, amino acids, carbohydrate, protein and any other substance that is normally found in the human diet. These can be taken as a concentrate of any of the individual constituents (including metabolites) of the diet. The definition also includes herbal extracts. In some cases there is some doubt whether particular agents are dietary supplements (legal as far as the IOC are concerned) or pharmacological agents eg dehydroepiandrosterone (an androgenic steroid hormone precursor) sold in the
USA as a dietary supplement but banned by the IOC
Amino Acid Supplements
There is no convincing evidence that oral amino acid supplements have any ergogenic effects on training or performance. There is some evidence that some amino acids (Arg, Lys ) can stimulate growth hormone (GH) release when taken intravenously or orally but these effects are minor compared to the natural release of GH which occurs normally during exercise. The level of circulating GH can increase 10 –fold during intensive exercise but there is no significant further increase GH by amino acids.
GH acts to increase amino acid uptake and protein synthesis (anabolic effect) and to stimulate lipolysis, increasing fatty acid release and reducing carbohydrate utilization (Metabolic effect)
Chromiak and Antonio (2002) Nutrition 18: 657-661. The IOC prohibits the use of GH as a pharmacological agent.
Creatine
Creatine is of course a natural component of meat and fish because of its role in the storage of energy as creatine phosphate. Creatine supplementation (creatine is not banned by the IOC) involves the ingestion of about 20 g /day for several days and it does indeed increase the muscle creatine levels particularly in untrained individuals. These increased levels can be sustained by taking a lower intake of creatine of about 3-g/day subsequently. There are a number of studies to indicate that creatine supplementation does indeed increase power output in the explosive sports such as sprinting and weightlifting. Presumably the elevated creatine phosphate level contributes to faster ATP turnover, delays depletion of phosphocreatine and reduces the dependence on anaerobic glycolysis as well as decreasing the recovery time after intense effort. Highly trained athletes, however, do not appear to benefit, presumably because their creatine phosphate levels are optimal anyway. Creatine supplementation does not improve performance in endurance events that require a high level of aerobic metabolism.
Caffeine
One of the most widely ingested drugs in the world due to its location in the leaves, seeds and fruits of plants. So it can be either a dietary supplement (a plant extract) or a drug, dependent on the levels found in the blood. The IOC has set an upper limit of 12
g/ml, accepting that it is a widely used drug. A cup of coffee can contain from 60 –180 mg caffeine dependent on the method of preparation while tea can contain from 20 –50 mg per cup depending on how long it has been brewed. Soft drinks like Coke and Pepsi have 46 and 38 mg respectively.
Caffeine is eliminated rapidly from the body
It is reported that coffee drinking 1 hr before exercise improves the endurance in aerobic exercise as well as performance in high-intensity effort. The physiological basis for this is not very well understood. Caffeine exerts a variety of pharmacological effects:
Caffeine increases cyclicAMP levels in adipose cells by inhibiting the action of adenosine receptors which normally inhibit lipolysis. It also inhibits phosphodiesterase which breaks down cAMP. The effect of the elevated cAMP is to promote lipolysis leading to an increase in plasma fatty acids and an increased use of fatty acid by muscle mitochondria sparing glycogen metabolism. There is good evidence that ingestion of caffeine leads to an increased dependence on lipolysis in prolonged exercise whilst increasing the total power output over a sustained period.
There is also evidence that caffeine exerts a direct effect on skeletal power at sub- maximal operation possibly because of the increased release of Ca 2+ from the sarcoplasmic reticulum.
Caffeine is a potent diuretic causing fluid loss, as well as exerting other undesirable physiological effects on the CNS as well as increasing heart rate and blood pressure.
Medium Chain Triglycerides (MCT)
These are sources of fatty acids (C
8
- C
10
) which are more immediately available than the normal fats which are esters of glycerol and long chain fatty acids (C
16
- C
18
). This is partly because of the delay in gastric emptying and slow absorption and distribution of these latter fats. MCTs on the other hand, are rapidly absorbed and digested into medium chain fatty acids (MCFA). These can move quickly across plasma membrane and enter mitochondria without the intervention of the carnitine- acyl transferase system and undergo
-oxidation.
The proposed mechanism is that these are oxidised in preference to glycogen in the short term thus sparing the need to break down glycogen stores as rapidly as in the absence of MCFA’s.
There is some evidence of a small increase in energy output in a 40 km cycling trial with reduced carbohydrate metabolism.
L
-
Carnitine
Carnitine facilitates the uptake of fattyacyl CoA derivatives by mitochondria thus accelerating the process of
-oxidation of fatty acids. It also lowers lactate levels by reduces inhibition of pyruvate dehydrogenase. Carnitine may be useful for the clinical treatment of patients with progressive muscular weakness, there is no evidence that it is beneficial in endurance athletes or those undertaking anaerobic exercise even in normally sedentary individuals. (Note that the mixed isomer
D,L
-
Carnitine is toxic)
Bicarbonate Loading
The rationale here is that anaerobic glycolysis leads to a significant lowering of intracellular pH (acidosis) leading to a decrease in the efficiency of muscular contraction. This acidosis can be counteracted to some extent by increasing the buffering capacity of the blood reaching
Alkalosis can be induced by ingesting sodium bicarbonate solution which raises the pH of the blood by about 0.1 pH unit. There is evidence that this can significantly enhance muscle power over a short period of time, presumably as the result of the change in pH and the greater capacity to ‘mop-up’ H + ions produced in anaerobic glycolysis. Adverse effects of bicarbonate loading can include abdominal discomfort and diarrhoea, which could negate any positive effects of this treatment.
-Hydroxy
-methyl butyrate
A bioactive metabolite – normally a breakdown product of the essential amino acid, leucine.
It has a very short half-life in the body of 2-3 hr so it is taken is small doses several times a day. It may decrease protein catabolism and possibly increase fatty acid
-oxidation. Appears to increase muscle strength. Not many studies on either its effectiveness or potential adverse effects so far. It was only introduced in 1996 and is one of the most expensive dietary supplements.
References :
Exercise Physiology 5 th ed. (2001) McArdle, Katch and Katch Chapter 23 Special aids to training and performance
British Medical Bulletin Vol 48 (3) Sports Medicine p 477 – 95, 569-91