University of - Brain & Behavior Research Foundation
advertisement

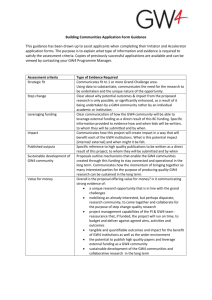
UNIVERSITY OF PENNSYLVANIA "TruTranscripts, The Transcription Experts" (212-686-0088) 2-1 University of Pennsylvania Healthy Minds Across America April 10, 2010/Tape 2 NARSAD RESEARCH (Background Conversation) DR. RUBEN C. GUR: When we try to understand the abnormalities in brain, one major effect of having a brain disorder is that your cognitive processes suffer. And, over more than a century of trying to link what cognitive disorders are impaired, depending on which brain region is impaired, we developed a set of tests that measure different cognitive functions, and that can be linked to a specific brain system. And, this is a typical assessment that is done in the field, to look at ... (Background Conversation) DR. RUBEN C. GUR: That look at different domains of behavior. So, for example, we measure abstraction in mental flexibility. It turns out that people who have frontal lobe damage have a difficult time abstracting a principle out of events, and once they come up with a certain pattern of behavior, they persist in it. They can't change their position. And, this is related to frontal lobe damage. Attention requires cooperation between two parts of the brain, one part that tries to shut out everything and tune into the most important stimulus. You are right now flooded by stimuli, even though it's a fairly quiet room. There's light, there are slides, you're reminded that you're maybe a little hungry, maybe a little thirsty, maybe a little tired. So a lot of things bombard your brain, and you have to tune all UNIVERSITY OF PENNSYLVANIA "TruTranscripts, The Transcription Experts" (212-686-0088) 2-2 of them out and just listen to the strange accent talking to you. This is attention. And there is one part of the brain that decides what is important. So that part ... for example, if an animal is hungry, and we put an electrode there, when we show the animal food, it will light up. But if the animal is not hungry, the same region will not light up for food. That very same neuron will light up if the animal is thirsty and you're showing it water. And then, that information goes to the front of the brain, and the front of the brain decides what to do. So when we measure attention, we look at the parietal frontal system. Memory is mostly in the temporal lobe, in the area right behind your ears. And if it's verbal memory, like remembering a list of items that you need to get in the supermarket, or remembering a story, or remembering any verbal information, that's more done in the left side of the temporal lobe. Remembering faces, remembering events, spatial scenes, is done more on the right side. Language is mostly in the left hemisphere, and there are parts of the brain that are responsible for understanding language. Other parts are responsible for speaking. So, if a patient gets damage in the front part of the left hemisphere, they will understand what you tell them, but they have a hard time answering. They can't articulate the answer. Conversely, if the damage is in the back, they speak fine, but they don't understand. So, by looking at both comprehension and expression of language, we can map where the damage could be in there. Spatial processing, the ability to navigate, the ability to throw a stone and make it hit, those kinds of things, the visual angles, UNIVERSITY OF PENNSYLVANIA "TruTranscripts, The Transcription Experts" (212-686-0088) 2-3 rotating objects in your mind in three dimensions, that's all done in the right hemisphere. Sensory and motor functions are somewhere in the middle of the brain. And these are also important, because if they are impaired, we know there is a problem there. Now, for years, we have been studying this. But really, anyone who knows people with severe mental illness know that, yeah, they have difficulties in attention, they have difficulties in memory, they have difficulties in those areas. But really, a lot of the difficulties are related to emotion. They just don't emote the way most people do. Sometimes they don't understand when I try to express something to them. They understand the words, but they don't get the feeling behind it. And, sometimes they become very threatened by something very innocuous. I just said something very simple, and they get all startled. So, why is that happening? And in order to understand that, we have to understand how the brain deals with emotion. So, many years ago, Charles Darwin recognized that, and wrote a whole book, a very important contribution on emotion. And what Charles Darwin said is, if you want to study emotion, look at the face. And as you can see in this illustration, all these bodies look identical. But if you try to look at the face, you pretty much can tell where that body is lying on the path of the motorcycle. So, this person is very happy. He sees the motorcycle already passed. This person sees the motorcycle approaching. And this person thinks this is possible, that the motorcycle will end right on him. So, the face tells you what the person is feeling. And what Darwin has also pointed out is that, across species, the same muscles literally are used on the face in order to UNIVERSITY OF PENNSYLVANIA "TruTranscripts, The Transcription Experts" (212-686-0088) 2-4 express specific emotion. So, an angry human being and an angry dog literally move the same facial muscles. And so, when you run into a dog that looks like that, you know how that dog is feeling. And so, emotions are not only to communicate within the species, but also to communicate across species. And it's a very important function. Now, how do we study emotion? We put a lot of effort about 10 years ago, because the field was behind. It wasn't really only our fault, but the whole field was not really recognizing the importance of understanding emotion. We didn't have stimuli. We had to get emotional expressions that we can use in order to probe the ability to comprehend emotion. So we turned to the thriving community of actors and actresses in Philadelphia area, and with the help of the artistic director of the Arden Theater(?), we brought in 150 actors and actresses who are professionals in expressing emotion. And they really know how to do it. And so, we collected about 5,000 pictures. And because actors become really emotional, and they move, we had to get help from the geeks over in the computer science department. And they set us up with the ability to obtain the face in the three dimensions, so the actor was free to move about. And after that, we could straighten up the face and create stimuli that expressed different emotions. This is hiding, but it's interesting. The eyes are hiding, and what we are finding, for example, is that patients mostly determine emotion from the mouth. They don't look at the eyes. Now, in this case, it's clear that this person is happy. You don't needed to see the eyes. And that this woman is sad, and this angry, and this is fearful, and this person is disgusted. These are emotions that are universal. UNIVERSITY OF PENNSYLVANIA "TruTranscripts, The Transcription Experts" (212-686-0088) 2-5 Anywhere around the world, people understand these specific emotions. Happy, sad, anger, fear and disgust. So, after we have that, we can go and find out how people perform. And, one thing that becomes very clear is that, in terms of emotion processing, men and women are like two different species. Women are way better, and take a lot less effort, in understanding and expressing emotions. This is a study, a functional MRI, where we gave healthy people just a job. They see an emotion, they have to tell us whether it's happy or sad or angry or fearful. And, we looked at how much activity, and which regions become activated in the brain. And this shows you slices of brain, going from the bottom all the way to the top. This here is the visual area, so part of the brain that needs to analyze the face is lighting up. But this, here, is called the limbic system, and that's the part that becomes engaged with emotion. That's the part that really lights up if you are angry, or if you are fearful, or if you are really happy. For men, just to understand the emotion, there is a literal limbic storm in their brain. The whole emotion area needs to work on it. Whereas, for women, they do light up the visual areas, but then they just light up a region called amygdala, which is a specialist in understanding emotion. The amygdala is the part of the brain, it's right in the middle of the brain, and that lights up every time anything you see has an emotional relevance. What happens with patients with schizophrenia, if you do the same study? It's a desert. The limbic area just doesn't light up. It just doesn't respond to the emotional content of the face, even though they have to decipher the emotion. UNIVERSITY OF PENNSYLVANIA "TruTranscripts, The Transcription Experts" (212-686-0088) 2-6 Now, here's, in the more recent study, we replicated that effect. But we try to see what happens to a brain of someone with schizophrenia when they just see a face. Happy face, or an angry face, or a fearful face. What happens to the brain when they see it? Now, if you just look at their activity during ... this is basically, they were lying in a scanner, and they would see, this is a baseline stimulus. Then they will see a face. Then they'll see another face. And the job here, in this one, push the button every time you see a happy face. Then this will be repeated. Push a button every time you see a sad face. Then every time an angry face, every time a fearful face. So, just working on this task ... MAN: Ruben, (Inaudible). DR. RUBEN C. GUR: Yes. MAN: What's the difference between the colors? The yellow on the top, and sort of more darker on the bottom? DR. RUBEN C. GUR: Okay. The colors indicate how much activation happened in that particular region. And these are only statistically significant areas. We don't look at areas where it wasn't statistically significant. And this is, the lowest level of statistical significant is 2.3. The highest that we got was 6.2. And you see that healthy subjects activate visual areas, and they activate the limbic system, amygdala, at a range between 4.2 and 6.2. It's very strong activation. Patients with schizophrenia, their brains are no different. They activate the same regions. But they activate it in the range of 2.3 to 4.5. Much less. UNIVERSITY OF PENNSYLVANIA "TruTranscripts, The Transcription Experts" (212-686-0088) 2-7 And this line here shows what happens if we take controls and we subtract patients from them, statistically. So, we can see, what are regions that are significantly different between controls and patients? And it turns out that controls activate more of the amygdala that you already heard about. The inferior frontal region that is involved in making a decision, in evaluating. So, the inferior frontal is very prominent. And then, the thalamus, which is the traffic cop of the brain. And the traffic cop says, what do I do? Where do I send that information? Okay? So, this is over the whole task. Now, we can probe the same study to ask a more specific question. What brain regions become active every time you see a face? And how does that predict whether or not you will identify the emotion? And this is where we see a big difference between patients and controls. This is happy, sad, anger and fear, and this is how much the amygdala is activated for each emotion. And in control, the amygdala is especially responsive. It's a very old organ. We share it with crocodiles. It just is a danger sensor, a threat sensor. So, if amygdala sees a happy face, it relaxes. Actually, the activation is negative. It's down. Sad face, no danger. Angry or fearful face, that's when the amygdala activates. If somebody's looking at you angry or scared of something, then amygdala becomes active. And, the more the amygdala activates in healthy people, the more likely they are to correctly identify the face as angry or fearful. Yes? MAN: How about if it's a misperception? Like, if I understand, you're talking about, like, an angry face or a happy face would be a cue (Overlap/Inaudible). DR. RUBEN C. GUR: Right. UNIVERSITY OF PENNSYLVANIA "TruTranscripts, The Transcription Experts" (212-686-0088) 2-8 MAN: So, how about if the person who's amygdala we're talking about misperceives? DR. RUBEN C. GUR: Exactly. And that's exactly what we are looking for. What happens if someone sees an angry face and they say, happy, or neutral? Well, in healthy people, the more the amygdala activates, the more likely the person is to perceive the face correctly. In patients with schizophrenia, we have a paradoxical finding, which you see here in the blue line. Actually, if the amygdala activates, for fear or angry faces, they say, this person is happy. So, the amygdala malfunctions. It sends the wrong signal, and it does more of that if it activates. So, one implication is that we need to teach, either pharmacologically or through training, teach them to relax. Teach them not to be so anxious, or give them a medication that will reduce the level of anxiety. Because, the amygdala is already highly tuned, and paradoxically, if it should go up, it shuts down. WOMAN: I have a question. Does the same thing happen in other mental illnesses? DR. RUBEN C. GUR: So far, we have only seen this in schizophrenia. And what we also found ... it's one question to see it in a patient. What does it mean? How does it relate to the clinical symptoms of these patients? And, here, we found a correlation that is very rare, very big point. Usually a correlation goes from -1 to +1, and -1 means, every time one thing goes up, the other thing goes down. +1 means every time one thing goes up, the other thing goes also up. This is a correlation of .937, which is almost unheard of in relating behavior to anything. UNIVERSITY OF PENNSYLVANIA "TruTranscripts, The Transcription Experts" (212-686-0088) 2-9 These are the clinical ratings of flat affect(?) in the patients. These are patients who just don't respond emotionally. And it turns out that the more there is increase in amygdala in response to a fearful face, the flatter the affect. So, these patients learn not to trust their amygdala, not to assume that, because they think something is threatening, it really is threatening. And what is the safest way is to shut down emotionally. That's the way they can deal with it. We also examined what happens ... so, you meet a lot of people. And sometimes, when you meet them first time, they are in a happy mood. Sometimes they are in a bad mood. How does that influence your ability to recognize them next time? And what we are finding ... and this is a paper that just came out last week, in the American Journal of Psychiatry ... what we find is that, if the first time you see a face, that face is happy, the next time you see it, the amygdala is less likely to activate than if the last time you saw it, the face was angry. So, even though, right now, you're seeing the face ... in the recognition phase, all of these faces were neutral. This woman, if when I saw her first, she had this fearful face, when I see her next time, even though her face is neutral, my amygdala will be sounding an alarm. Yes. MAN: So, in a sense, if I understand you, it sounds like anger, seeing anger, seeing an angry face, will imprint itself more on you than seeing a happy face. DR. RUBEN C. GUR: That is correct. Yes. Yes. And it turns out that, in patients, this whole system is attenuated. And, the more it is attenuated, the more severe symptoms they have. So, here's another example of relating severity of symptoms to the deficits in being able to recognize faces, especially emotion on the face. UNIVERSITY OF PENNSYLVANIA "TruTranscripts, The Transcription Experts" (212-686-0088) 2-10 The other thing we can do with functional imaging is look at the correlation between what happens when you make one part of the brain active, and the rest of the brain. And this way, we identified a system that, if you look at what is correlated, it turns out that there is a whole system here that becomes active for recognizing emotion. And, in patients, this system is overactive. So, every time there is an evocation of the emotional system, in healthy people, it stays in the emotional part of the brain. In patients, it spreads to the cognitive part of the brain, and they begin to ruminate. They begin to do more with it than they should. Now, we have, now, a computerized battery that basically is comprised of all the tests that we have used over the years inside the scanner. So, the difference between these tests and those that I've showed you when I started, is that these are all tests that have been administered to people in the scanner, so we know what part of the brain becomes active. We can look at it more precisely. It's also more efficient because it's computerized, so all the responses are immediately recorded, and there is no error in putting in the data. You don't need to interpret. You do the test. The whole thing takes about one hour, instead of the old way that took almost half a day, and sometimes more. And at the end, you get a lot more information, because you find out now only how accurately they perform, but also how fast they perform. The computer is excellent at faithfully recording how many milliseconds it took you to think about each question. As you know, performance is a bull that has two horns. One of them is called accuracy. The other is called speed. Practically anybody could do anything, given enough time. But if you have a UNIVERSITY OF PENNSYLVANIA "TruTranscripts, The Transcription Experts" (212-686-0088) 2-11 deadline, you can do the most perfect product, you miss the deadline by an hour, and it's worthless. So you always have to juggle between how well you want the job done and how quickly it needs to be done. So we can look at that the way patients do it. And here is an example of a big, again, sex difference that we are studying in patients. In this test, you see a face, and you have to say, is this happy, sad, anger or fear? In this test, you see two lines. This is a test of line orientation. And you click a button that will move the red line and try to make it have the same angle of the blue line. So, how many times do you click until they are really parallel? And these are huge sex differences. This study was run by NBC on its Web site, so thousands of people took the test. And this is their performance, relative to age. And you can see that for emotional discrimination, accuracy goes up a little bit between early years and later years, and then it goes down. As you know, with aging, things go down. But women are more accurate than men. If you look at speed, women are faster than men, even though speed, again, goes down with aging. If you look at line orientation, you get exactly the opposite result. Men are better than women, also across the age range. If you look now at teenagers, who are at high risk to developing schizophrenia, you see that their main deficits are in abstraction and flexibility, in memory, especially face memory, and in the ability to detect emotions on the face. Now, psychiatrists do make a diagnosis after an interview of someone, and they may say, "This patient has flat affect." And this, how good the diagnosis is, entirely depends on the experience and UNIVERSITY OF PENNSYLVANIA "TruTranscripts, The Transcription Experts" (212-686-0088) 2-12 training of the psychiatrist. So we are working to make this something more objective. And again, our friends in the computer science department have devised a method where you can take a face of a person, when it's neutral, take the same face when it's showing an emotion, and use it like the same method used to analyze brains. You stretch or squeeze the emotional face to fit into the neutral face, but you record at every picture element how much you had to stretch or to squeeze, in order to get there. And so, now, it turns out, the computers ... if anybody told you computers don't understand emotions, they didn't used to. Now they do. Computer can identify happiness, sadness, anger and fear very well. And now, we can go ahead and see what happens for a patient, and we can do it as a movie. We can take a patient describing a happy experience or a sad experience, and the computer will go frame by frame and tell us, "This one is happy. This one is anger. This one is fear." So, they can do segment by segment, what the person was expressing. And, if we now compare a healthy person, here. Green is happy. Sad is brown. Anger is red. Fear, yellow. And neutral is blue. Here we ask a healthy person to express happiness, and most of the lines, during this 400 seconds that we took, most of the lines are green, is up(?). So, the person pretty much expressed happy. Here, it's brown, for sad. Here it's red, for anger. It took a bit longer for that person to finally show up, anger. And here it's yellow, for fear. UNIVERSITY OF PENNSYLVANIA "TruTranscripts, The Transcription Experts" (212-686-0088) 2-13 If you look at the patient with schizophrenia, happy, they sort of almost overdid it. But, sad, anger and fear, all sorts of emotions came up. Really unrelated. You couldn't really tell. And if you summarize it across ... and this is a study that Dr. Kohler was senior author on, you can see that, most of the time, for healthy people, when you ask them to express a particular emotion, most of the time they express the appropriate emotion. And very little different emotions. In patients, most of the time it's neutral. And they spend almost as much time expressing the target emotion as expressing other emotions. Now, faces is not the only way we express emotions. We also express them in our voice. And if my talk gets too long, you will hear Raquel's angry voice saying, "It's 2:30!" So, we use that kind of a sentence. "It's 11:00." And you can say, "It's 11:00," neutral, or you can say, "It's 11:00!" You're happy that it's 11:00. Or you can say, "It's 11:00," or you can say, "It's 11:00!," the way Raquel will say in a moment. And most people will be able to tell whether you are happy about the fact that it's 11:00, sad, angry, or fearful about it. And, you can quantify how much specific vocal cues. You just basically analyze the vocal output, and you can quantify how much vocal cue needs to be present for people to identify. And it turns out ... this is a study a post-doctoral fellow, David Lightman(?), did in our lab ... that, the more cue there is in the voice, the better the recognition of the voice. What you can see is the patients with schizophrenia in the grey bar, this is attenuated. So even though you may say to a patient, "It's 11:00!," they are not going to pick it up as angry. You have to say it even more pronounced for them to be picking up. UNIVERSITY OF PENNSYLVANIA "TruTranscripts, The Transcription Experts" (212-686-0088) 2-14 The same for any other emotion. For happy, too. You may think that you express that you are happy. They may not hear it. They may not decipher the cues in your voice to make that determination. Now, what happens in the brain? It turns out, if you look at controls, there are two systems in the brain of controls that activate, basically. One is the superior temporal gyrus. It's right here, above the ears. It's the top part of the temporal lobe. And that part, it's right behind your ears, so it's convenient. It takes all the stimuli and integrates your auditory stimuli into meaningful perceptions. And then, there is the frontal part of the brain, the inferior frontal gyrus. And the inferior frontal gyrus interprets it. So, what we see is that, if you compare all emotions compared to neutral, again, healthy subjects, and people with schizophrenia, activate the same regions. It's not different brains. It's the same brains. The only thing that is conspicuous in its absence is that part. It's the singular gyrus. And that's the part that relays the information from the temporal lobe to the frontal lobe in order for it to make decisions. So, they need to be trained in activating that particular region, and there are programs that can be used to train people how to activate, how to connect between what you hear, what you see, and how to evaluate it. And, what happens in healthy people is, the greater the saliency in the cue of the emotion, the more there is a signal of the emotion, the more you activate this superior temporal gyrus area. When the saliency goes down, then the frontal lobe has to get in. You're not clear. Is the person angry, or fearful? Then, you begin to ask your frontal lobe, the one that decides, that puts things in context. UNIVERSITY OF PENNSYLVANIA "TruTranscripts, The Transcription Experts" (212-686-0088) 2-15 Say, well, that person couldn't be angry, because I just said something nice, so maybe it's something else. So, this part becomes more active, as the signal goes down. So, the clearer the signal, the less you need the frontal lobe. In patients, you see an attenuation in this difference. And if you look at the difference between patients and controls, they fail to activate sufficiently the frontal lobe, in order to interpret the emotion that they heard. Yes. MAN: These responses, like from the frontal lobe, the amygdala, are they voluntary or involuntary, or kind of a combination? DR. RUBEN C. GUR: They are involuntary. You couldn't change them. In fact, you can do a lot of this work in patients with epilepsy and need brain surgery. As you know, the brain doesn't have pain receptors. So, the only thing you need to worry about for pain is the skin above your skull. So, brain surgery can be done with the patient fully awake. And then, in order to find out how to avoid language areas, the surgeon will start sending electrical signal, in order to map, for example, the sensory motor area. So, they'll send one signal. If it's going to the left, the patient will lift the right arm. If it's going another spot next to it, they'll start moving their finger. So you can literally make them, like a puppet, do what you want by sending the electrical signal to the right. You ask the patient, "Why did you raise your right arm?" "Gee, I felt like it all of a sudden." Right? So, they never say, "Well, you must have done something." People don't respond that way. So, it feels like it's voluntary. But it's not. Yes? UNIVERSITY OF PENNSYLVANIA "TruTranscripts, The Transcription Experts" (212-686-0088) 2-16 WOMAN: Doctor, because the cues don't work effectively in a sick person, does that lead to anxiety? Is that why you have (Overlap/Inaudible) ... DR. RUBEN C. GUR: Exactly. Exactly. Because if you can't understand the emotion of the people talking to you, your safest bet is, you know, stay away. WOMAN: What if there's an overreaction? The opposite of stay away? What happens in the brain when there's an overreaction? DR. RUBEN C. GUR: Well ... WOMAN: Because (Overlap/Inaudible) ... DR. RUBEN C. GUR: They may attack. They may attack. WOMAN: Aggressive behavior. WOMAN: But I'm saying, what's going on in the brain then? DR. RUBEN C. GUR: So, the amygdala is an interesting structure, in terms of its activity as a function of stimulation. The disease that affects the amygdala the most is temporal lobe epilepsy. And those patients, if you study their brain between seizures, the amygdala looks almost like it's dead, like it's not there. There's very little activity in the amygdala. You study the same patient during a seizure, and the level of activity in the amygdala is off the charts. In fact, it's so high that it gets damaged. Because, when brain tissue begins to work, it breaks down sugar, and the products of breaking down sugar are toxic. And that's why we have blood flow going all the time through the brain, to clean the garbage. Not only to bring in the oxygen that's needed, but UNIVERSITY OF PENNSYLVANIA "TruTranscripts, The Transcription Experts" (212-686-0088) 2-17 also take out those toxic chemicals that result from brain activity. So, and a (Inaudible)-tologist will tell you, "I can't tolerate even one seizure a year," because every time there is a seizure, there is more damage. So, schizophrenia is not temporal lobe epilepsy, but the brain doesn't know from disease. That's not how the brain works. It's still a disorder that affects the amygdala. And the amygdala is a region that will go from no activity to a lot of activity, very quickly. People with damage in the amygdala have a syndrome called the Kluver-Bucy Syndrome, and these people are characterized, typically, as being super cool. Nothing seems to bother them. But then something totally unexpected, like hearing the tick of the swing of the baby, can set them off and they'll start breaking furniture. So it goes from zero to 60 very quickly. WOMAN: And what is that called? DR. RUBEN C. GUR: It's a syndrome called after the people who described it first. You see it in humans and in animals. It's called, I don't know how important, Kluver-Bucy Syndrome, after the people who discovered it. And it's symptom of amygdala damage. Animals, too. Mice. Yes? WOMAN: Doctor, have they done any correlation, correlate ... I don't have the right word ... between sleep apnea and not getting enough oxygen and (Inaudible)? DR. RUBEN C. GUR: Sleep in mental health is a very neglected area. There is more and more work in this area, but we don't have enough knowledge on it. WOMAN: So, just to clarify, temporal lobe epilepsy and schizophrenia. There are journal articles where they seem to overlap, UNIVERSITY OF PENNSYLVANIA "TruTranscripts, The Transcription Experts" (212-686-0088) 2-18 and then they spread back out, and then they overlap. So, it is just opposite, (Overlap/Inaudible) ... DR. RUBEN C. GUR: It's not clear. There's a British psychiatrist by the name of Trimble(?), who made a career out of comparing schizophrenia and epilepsy. Also, Pierre Flor-Henry, a Canadian. It affects the same organ system, but it's unclear that the mechanisms are even similar. So, it's not surprising that you have some common features. And it wouldn't be surprising if it turns out that some treatments in one disorder help in the other. But, the causes are different, the pathology is different, the genetics are different. So we need to understand schizophrenia independently. It's 2:30. Or, almost 3. My goodness. All right. So, basically, I want to thank everybody who is helping in this research, and for your patience in listening to me. Thank you very much. (Applause). WOMAN: (Inaudible) question? WOMAN: When people have that (Inaudible) weaken the amygdala, is there a test that'll show that? DR. RUBEN C. GUR: Well, we can do functional imaging study, and that's what we are looking at now. These are called biomarkers, and Raquel referred to them as evoked endophenotypes. We can take a patient, give them this same paradigm, the same task that we use in the healthy people, and see how their brain responds differently. And that will tell us that this patient does have that problem. Increasingly, we are coming to what is called individualized medicine, where we know the genetic makeup, we know the specific UNIVERSITY OF PENNSYLVANIA "TruTranscripts, The Transcription Experts" (212-686-0088) 2-19 abnormalities, and we can begin to tailor treatment to individuals. It's not there yet. I would say five years, it will be there. WOMAN: So, generational, if you know it goes back to the generations on one side of the family, we can say, well, this person was put in a home with Alzheimer's. But it wasn't really Alzheimer's. It was sort of bipolar, sort of schizophrenia. We're not sure. But we didn't label it that. And the next generation comes along. Clearly, it's bipolar, schizophrenia, but that's not in our family. And the next generation comes along, which is my kids, and I say, this is clearly something wrong, and we're going to treat it before it gets worse. But, does each time the gene expresses itself get worse and earlier? I mean, how does that work that ... DR. RUBEN C. GUR: There is no evidence that subsequent generation have worse cases. None whatsoever. WOMAN: Just, we're more aware of it. DR. RUBEN C. GUR: I think that's the main thing that happens here. But, it's the same as with heart disease. It used to be, when they say heart disease goes in families. It turns out, it's not heart disease that goes in families. It can be high cholesterol, high blood pressure, high sugar levels, Type A personality, those people who think they carry the whole world on their shoulders all the time. So, smoking has a genetic component. So, you can have all those genes, but you lead a healthy lifestyle, and you take your Lipitor, and you exercise, and you don't smoke, you can outlive someone who has none of these genes. On the other hand, if you have these genes, and you have a hoagie every day and you are sedentary and you smoke, and all that stuff, you'll get that disease. UNIVERSITY OF PENNSYLVANIA "TruTranscripts, The Transcription Experts" (212-686-0088) 2-20 WOMAN: I think you're right on, Doctor. I'm Mary (Inaudible). I unfortunately lived(?) manic depressive, but was not manic depressive. And I'm now a mental health advocate in (Inaudible) County Health Department with the MAP(?) program. And the MAP program is to get rid of the stigma of mental health, because it all relates to our life's ups and downs, and how we deal with them. And, my specialty is with adolescents, because most adolescents are being diagnosed manic depressive, where, what it is, in my opinion, because I deal with this, is that they're brought up to believe the world is hunky-dory. Then when they're in adolescence and facing the real world, it's not hunky-dory. So they're having a problem adjusting to real life. Then, the psych world has taken it, diagnosed them manic depressive, unipolar, bipolar, whatever you want to call them, thrown them on drugs. The drugs pose a lot of side effects. You know, there's good and bad of everything. So I'm glad to hear, and excuse my ignorance to not knowing, you know, I'm glad to be here to hear everything you and your wife had said. DR. RUBEN C. GUR: Thank you. DR. RAQUEL E. GUR: I think maybe brief questions, so that we can be on time? And if Doctor ... (AUDIO DROP-OUT) DR. RUBEN C. GUR: Most of the environmental effects are intra-uterine. WOMAN: (Inaudible). DR. RUBEN C. GUR: Yes. Usually, there is evidence associating malnutrition during the second trimester. Other evidence shows link with the flu during second trimester. Most of the UNIVERSITY OF PENNSYLVANIA "TruTranscripts, The Transcription Experts" (212-686-0088) 2-21 environmental effects that occur after birth can produce a lot of psychological damage, but they do not generate something like schizophrenia. WOMAN: (Inaudible). DR. RUBEN C. GUR: Or bipolar illness. They could generate other, milder forms of mental illness. DR. RAQUEL E. GUR: The whole line of research that is just beginning in serious mental illness is called epigenetics. So, these are changes that can take place intrauterine, perhaps even after that. Because of conditions that modulate the effects of the genes. So this is now a new line of research that is done in humans, beginning, and also in animal studies. And it's coming from cancer research. So some of the methods that have applied to cancer research are now being applied to serious mental illness, primarily to schizophrenia, and then bipolar. The children (Overlap/Inaudible) ... DR. RUBEN C. GUR: And these are genetic changes. They occur in the gene, but you did not get them from your parents. DR. RAQUEL E. GUR: Mm-hm. So, there's a change in the genetic expression from environmental conditions. WOMAN: So, all (Inaudible). DR. RUBEN C. GUR: Right. Right. But, I think it's also ... not to minimize the environment, even for healthy brains, the ways that we do that to make the environment helpful for us. So, if it applies to, you know, healthy brains, it should apply to vulnerable brains. So, let us climb out(?), not being overstimulated, getting too excited about things, or reducing stress, and increasing resilience. So, these things that are important. The work on the brain result (Inaudible), you know, making the genetic change. UNIVERSITY OF PENNSYLVANIA "TruTranscripts, The Transcription Experts" (212-686-0088) 2-22 DR. RUBEN C. GUR: Also, the environment is important for shaping what ends up happening. You can probably have the identical genetic makeup, and if you grew up in an affluent environment, you will become the dean of a medical school. If you grew up in the ghetto, you may become, you know, the head of a mob. So, that's a big difference. But, and that's because of the environment. That's ... DR. RAQUEL E. GUR: There's opportunities (Inaudible). WOMAN: Not just (Inaudible), can the way you were raised make it worse? DR. RAQUEL E. GUR: Oh, it can make, maybe, the people who have the vulnerability more likely to express it. Yes. Mmhm. That's one of the focuses. Let me take the last question (Inaudible). WOMAN: (Inaudible). I mean, if you're going to have a bipolar break, it's often between ages 15 and 18, first, when it happens. And believe me, it doesn't matter if your parents came from University of Pennsylvania or Columbia and have the best environment. If you have the genes for bipolar, you will have the break (Inaudible) experience, when I worked in patient psych. Brilliant Penn students, brilliant, with brilliant parents, (Inaudible) visits. If they're going to have a schizophrenic break when they're 20, they will have their schizophrenic break, or bipolar. It's sad, but it's true. And ... (END OF TAPE)