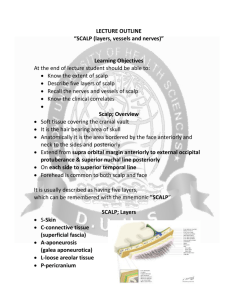
Scalp Reconstruction
advertisement

1 SCALP RECONSTRUCTION Scalp anatomy THE HAIR-BEARING AREA extending from the top of the neck muscles at the back, to the forehead and eyebrows at the front and down over the temples to the ears and zygomatic arches. Alternatively: The soft tissue covering of the cranium. Unit composed of skin, dense subcutaneous tissue and epicranius muscle. Boundaries Posteriorly: Anteriorly: Laterally: Posterior nuchal line Superior orbital ridges Temporal lines and upper borders of the zygomatic arches LAYERS S Skin C Connective tissue (dense) = Subcutaneous connective tissue. A Aponeurosis = Epicranial aponeurosis and muscle.= galaea L Loose areolar tissue= subaponuerotic fascia P Pericranium The first 3 layers are firmly bound together and contain the vessels and nerves. 2 1. SKIN skin of the scalp is the thickest in the body, measuring between 3 and 8 mm, which makes it a useful donor site for split-thickness grafting. It is denser here than anywhere else in the body. It contains a great number of hairs, sweat and sebaceous glands. It is attached by dense fibrous septa to underlying aponeurosis and muscle. 2. SUBCUTANEOUS DENSE CONNECTIVE TISSUE A firm, dense, fibro-fatty layer. Contains fibrous septae which bind the skin to the underlying galea aponeurotica. The hair follicles of the skin often extend into this layer.(thus skin flaps should include some fat to protect these structures) vessels, lymphatics, and nerves course through the subcutaneous layer just superficial to the galea. The abundant fibrous tissue in this layer surrounds the blood vessels and prevents them from contracting when cut. This is why the scalp bleeds profusely when injured. Infections in this layer are contained by the fibrous tissue and tend therefore to be localised but very painful. 3. GALEA APONEUROTICA = EPICRANIAL APONEUROSIS = EPICRANIUS Musculaoaponuerotic layer =The Galea: Strictly speaking the galea refers to the aponeurotic component of this layer but the musculoaponeurotic layer contains the frontalis and occipitalis contiguous with the paired frontalis muscles anteriorly, the paired occipitalis muscles posteriorly, and the temporoparietal fascia laterally. the strength layer of the scalp 3 Its fibres are orientated sagittally so that longitudinal wounds tend to remain closed while coronally orientated wounds gape. The occipito-frontalis muscle: (a) Frontal Belly (frontalis) Paired quadrilateral muscles. Origin: Anterior border of the aponeurosis (below the coronal suture). Insertion: Interdigitates with the fibres of orbicularis oculi, corrugator supercilii and procerus, Attaches to overlying skin in the region of the eyebrow. Note: The frontal belly has no bony attachment. Action: Elevates the eyebrow and produces transverse wrinkles of the forehead. Nerve: Temporal and zygomatic branches of the facial nerve. (b) Occipital Belly (occipitalis) Paired quadrilateral muscles. Origin: Superior nuchal line (ie, has a bony attachment). Insertion: Posterior edge of epicranial aponeurosis. Action: Draws the scalp backwards. Nerve: Posterior auricular branch of facial nerve. As this muscle is supplied by the facial nerve, the scalp may be regarded as an upward prolongation of the face that extends back to the occiput. 4 4. LOOSE AREOLAR TISSUE = SUB-EPICRANIAL SPACE = SUBGALEAL FASCIA This is a very thin, tenuous and delicate layer. Tolhurst found that this layer consists of a superficial + deep layer of loose areolar tissue + an intervening collagenous sheet. This is the plane of cleavage that is used when separating the superficial 3 layers from the pericranium (scalping) when raising a flap. Also known as the subgaleal fascia, the innominate fascia, and the subaponeurotic plane. The loose areolar tissue of this plane allows for scalp mobility. The layer is traversed by: (i) vessels and nerves that run from just above the orbit to the scalp, (ii) emissary veins that run from the intracranial venous sinuses to the scalp, (iii) small blood vessels that supply the pericranium. Because of the tenuous nature of this loose areolar tissue, it is a potential space in which blood or pus may readily collect. The ‘space’ is limited by the superior nuchal line posteriorly and the zygomatic arch laterally, but anteriorly, because frontalis is not attached to bone, the ‘space’ has no limit and any collection may spread into the face. This subgaleal fascia can be harvested for thin, pliable coverage of defects of the head and neck or can be used for free tissue transfer. greatest amount of scalp mobility occurs in the parietal regions where the temporoparietal fascia overlies the temporalis fascia In general, the design of scalp flaps takes advantage of this feature so that tissue advancement is gained from the parietal regions. 5. PERICRANIUM The periosteum of the scalp. A thin yet strong membrane. It is loosely attached and strips easily from the skull, except at the suture lines where it dips between the bones as the sutural membrane which is continuous with the internal periosteum (outer layer of the dura). BLOOD SUPPLY OF THE SCALP The scalp is supplied by vessels that enter at its periphery and which run in the subcutaneous connective tissue. Because of the multiple, free anastomoses that exists, one set of vessels can nourish the entire scalp. This superb blood supply allows the design and construction of a wide variety of flaps that in other parts of the body would not survive. 5 The main blood supply to the scalp comes from the external carotid artery via four branches. The internal carotid artery by way of the ophthalmic artery provide a further two branches to the front of the scalp. EXTERNAL CAROTID BRANCHES 1. Superficial Temporal Artery 2. Posterior Auricular Artery 3. Occipital Artery Cephalic to the nuchal line 4. Internal Maxillary Artery (mentioned only in McC) – deep temporal artery INTERNAL CAROTID BRANCHES 1. Supra-trochlear Artery (medial; smaller) In line with medial canthus 2. Supra-orbital Artery (lateral; larger) In line with medial limbus Note that there is thus an anastomotic system between the internal and external carotid arteries in the scalp. The Superficial Temporal Artery (STA) The large terminal branch of the external carotid artery that emerges from the upper end of the parotid gland. It runs behind the TMJ and crosses superficial to the posterior root of the zygomatic arch just in front of the ear. Branches: 1. Transverse facial Face. 2. Middle Temporal Arises close to the zygomatic arch, pierces the temporal fascia to supply the temporal muscle and then anastomoses with the deep temporal branches of the maxillary artery. Its companion vein grooves the skull. 6 Terminal branches: 1. Frontal The smaller anterior branch which runs a sinuous course to the forehead and which is prominent in the elderly. 2. Parietal The larger posterior branch which runs to the parietal eminence. Posterior Auricular Artery Arises from the external carotid in the parotid gland. Runs posteriorly behind the ear, in front of the mastoid process to the scalp. It is accompanied by the lesser occipital nerve. Occipital Artery Arises from the external carotid artery opposite the facial artery near the lower border of the digastric muscle. It ascends close to the inner aspect of the mastoid process (can be palpated). It emerges from the apex of the posterior triangle and runs up to supply the scalp. It is accompanied by the greater occipital nerve. Three main types of variations in the relations of the occipital artery and the hypoglossal nerve found in 42 dissected specimens are described, according to the level at which the nerve crosses the external carotid artery and the point of origin of the occipital artery. o Type I, the hypoglossal nerve crosses the external carotid artery inferior to the origin of the occipital artery – most commonly described where hypoglossal nerve passes in between occipital artery and its branch to SCM o Type II, the nerve crosses the external carotid artery at the level of origin of the occipital artery o Type III, it crosses superior to that level. 7 THE VENOUS DRAINAGE OF THE SCALP The veins run back with the arteries. The supra-orbital and supra-trochlear veins drain by the angular vein into the (anterior) facial vein. They also connect to the ophthalmic vein. The superficial temporal vein drains into the retromandibular vein (with the maxillary vein) and thus into the external jugular vein. The posterior auricular vein drains into the external jugular vein (with the retromandibular vein). The occipital vein drains into the suboccipital venous plexus which empties both into the vertebral and external jugular veins. Diploic veins from the frontal, parietal and occipital bones enter nearby veins. 8 Emissary veins: These are important connections between the veins of the scalp and the intracranial sinuses. They may allow infection to spread from the scalp or face intra-cranially. The following are recognised emissary veins: 1. 2. 3. 4. 5. 6. 7. 8. 9. vein of the foramen caecum (frontal sinus to superior sagittal sinus) ophthalmic veins (supra-orbital veins to cavernous sinus) parietal emissary vein mastoid emissary vein (posterior auricular vein to transverse sinus). nb and constant. veins of the hypoglossal canal (deep veins of the neck to the transverse sinus) veins of the condyloid canal (deep veins of the neck to the transverse sinus) veins of the foramen lacerum (pterygoid plexus to the cavernous sinus) veins of the foramen ovale (pterygoid plexus to the cavernous sinus) middle meningeal emissary vein LYMPHATIC DRAINAGE OF THE SCALP A coronal watershed runs from ear to ear. The scalp anterior to this line drains to the parotid lymph nodes. That part posterior to the line drains to mastoid, preauricular and occipital lymph nodes which drain into the deep upper cervical nodes. 9 THE NERVE SUPPLY OF THE SCALP (A) TRIGEMINAL (V) (I) Ophthalmic Division (V1) gives off a frontal branch which divides into: (1) Supra-orbital nerve This emerges from the supra-orbital notch usually as 2 branches: a. superficial division pierces the frontalis muscle on the forehead and supplies the skin of the forehead and anterior hairline region. b. Deep division runs just superficial to the periosteum up until the level of the coronal suture, where it pierces the galeal aponeurosis approximately 0.5 to 1.5 cm medial to the superior temporal line to innervate the frontoparietal scalp. 1. the upper eyelid 2. the forehead 3. the front of the scalp as far as the vertex. (2) Supra-trochlear nerve (smaller) Emerges medial to supra-orbital notch to supply: the upper eyelid lesser amount of the anterior scalp near the midline. (II) Maxillary Division (V2) gives off the zygomatic nerve which has as a branch The zygomatico-temporal nerve. It pierces the temporal fascia close to the zygomatic bone. Supplies the skin of the anterior temple. (III) Mandibular Division (V3) The auriculo-temporal nerve runs with the STA in front of the ear. 10 Supplies: skin of the side of the scalp but not as far as the midline, skin of the external ear and EAM, the parotid gland. (B) OCCIPITAL NERVES (I) Lesser Occipital C2 anterior primary ramus from the cervical plexus. Supplies the skin behind the ear. (II) Greater Occipital C2 dorsal primary ramus. Supplies the skin of the scalp up to the vertex. emerge from the semispinalis muscle approximately 3 cm below the occipital protuberance and 1.5 cm lateral to the midline (III) Third Occipital C3 dorsal primary ramus. 11 Supplies posterior midline and adjacent scalp. THE TEMPOROPARIETAL REGION In this region, excluding skin, subcutaneous tissue and temporal muscle, there are 4, sometimes 5 different layers. Temporoparietal Fascia (=superficial temporal fascia): The most superficial layer beneath the subcutaneous fat. The lateral extension of the galea. Continuous with the SMAS. Subgaleal fascia in the temporoparietal region: Well developed and richly supplied by the STA. Easy to dissect as a discrete layer. Can be used as an inferiorly based flap for ear, eyelid and cheek reconstruction. Superficial temporal fat pad: Found along the inferior extent of the subgaleal fascia as it is reflected. Lies atop the deep temporalis fascia. Of variable size, usually thin. Not covered by temporalis fascia at any point. Temporalis fascia: A tough, thick, white, fascial sheet overlying the temporalis muscle. Above the superior temporal line, it fuses with the pericranium. The temporal muscle arises from the deep surface of the temporal fascia and the whole of the temporal fossa. Inferiorly, the temporal fascia splits in 2; The superficial leaflet attaches to the lateral border of the zygomatic arch, and, The deep leaflet attaches to the medial border of the zygomatic arch. There is a small quantity of fat between the two leaflets. Deep temporal fat pad: Between the temporal fascia and the muscle fibres there is a thin layer of bright yellow fat that is thought to allow easy gliding of the muscle under the zygomatic arch. The temporalis muscle: Origin: (1) Temporal fossa between the inferior temporal line and the infratemporal crest, and, (2) Temporal fascia. This fan shaped muscle converges from above downwards to its tendon which is inserted into the mandible. Insertion: (1) Coronoid process borders and inner aspect, and, 12 (2) Groove down the anterior border of the ramus of the mandible as far as the attachment of buccinator in the retromolar fossa. Innervation: From the anterior division of the mandibular nerve (V3) via 2 deep temporal branches Action: Mainly elevates the jaw, ie closes the mouth. The posterior fibres can retract the jaw (after it has been moved forward by the lateral pterygoids). This is the only muscle or part of a muscle that can retract the jaw. Blood supply: Temporal branches of the maxillary, reinforced by the middle temporal. Relations: Posterior to the temporalis tendon: Nerve and vessels to masseter. Anterior to the temporalis tendon: Buccal nerve and vessels. 13 TRAUMATIC DEFECTS 1. Lacerations Scalp lacerations may be involved with skull fractures cervical spine / brain injuries and life threatening problems an these should be excluded prior to the rx A Skin Defects Options 1. Direct closure 2. Dress only 3. SSG if periosteum intact and TE/excise subsequent stages skin grafts should be unmeshed to give the best possible appearance TE has revolutionised scalp reconstruction. Placed subgaleal In the acute setting, if perichondrium present, this can be grafted on to and later reconstructed with TE. 4. Burr outer table and graft (trephanation) Dress for 5-7 days then graft 5. Periosteal flaps 6. Random fasciocutaneous flaps If perichondrium is absent other options must be considered: The classic solution is a large rotation or transposition flap with SSG of donor area which is later reconstructed with an expanded flap. Local flaps can be used or the options mentioned above for total avulsion. Some special local flaps 1. Rotation flaps (better for small defects) 2. Transposition flaps + SSG (for larger defects) 3. Gillies tripod flap 4. Pinwheel flaps 5. Bipedicle flaps 6. Double opposing rotation flaps 7. Orticochea 3 and 4 flap method (large flaps pedicled at the periphery and raised like the peels of a banana. Used to surface frontal and occipital defects of medium to large size.) 8. Can do periosteal flaps and graft on to the flap. The stretch of local flaps is improved by criss cross incisions (scoring) in the galea. Basic surgical considerations 1. avoid diathermy to the skin edge – may destroy hair follicle 2. consider direction of hair growth when reconstructing 3. Excessive tension at wound closure can cause alopecia from either hair follicle loss or anagen phase arrest. 4. exploit skin viscoelastic properties of stress relaxation and creep with either hooks and manual force or by rapid intraoperative tissue expansion using expanders 5. galeal scoring 14 a. By carefully scoring the galea perpendicular to the direction of desired tissue gain, additional advancement can be achieved. b. According to Raposio et al., each galeotomy corresponds to a 40 percent reduction in scalp closing tension and approximately 1.67 mm of tissue gain. c. Ideally, the galea is incised at 1-cm intervals and tested after each score to see whether adequate tissue length has been gained. d. Care should be taken to prevent inadvertent injury to the scalp arteries that lie just superficial to the galea. e. Avoid electrocautery when performing galeal scoring to prevent potential thermal injury to these vessels. 6. Disregarding topical adhesives, staples are the least ischemic of skin closure techniques 7. resist the temptation for excision of dog ears – these usually settle with time Small defects (3-5cm) Smaller defects usually closed directly Important to close the galea as a separate layer Defects no larger than 3cm can be closed directly by undermining Periosteal flap In the event of exposed bone a flap of periosteum centered over a major feeding vessel radiating 1-2 cm from a feeding vessel can be rotated in and then grafted with SSG For defects up to 7cm Certain points when designing these flaps: o Random vessels that vascularize these flaps are weakest between the major territories hence the flap should be centered over a major vasc territory and should not cross the midline o Pedicle dissection is limited to a point 1-2 cm from the where feeding vessels may enter the o When dissecting over temporalis the aponeurosis should be included to augment the vascularity of the flap o They are thin flaps and thus are very susceptible to pressure, hematoma seroma etc 15 In non graftable bed can also remove the outer table to expose well vascularized diploe which is dressed for 5-7 days and then grafted Small defects of the scalp and forehead can be resurfaced with advancement flaps on the subcutaneous pedicles Pinwheel flap pinwheel incisions are approximately twice as long as the diameter of the wound. 4 incisions at 0o, 90o, 180o and 270o. advantage of minimal undermining of a uniquely designed flap with very little need for excision of excess normal tissue and distribution of tension over four suture lines 16 Rhomboid flaps Various designs: o Reconstruction of the vertex of the scalp with three adjacent rhomboid flaps to replicate the natural whorl pattern of hair in this region o Bilobed design - limited to defects no larger than 5 x 4.5 cm in the parietal region. 17 Larger defects Fasciocutaneous flaps Mainstay of reconstruction of defects of the scalp Local flaps of hair bearing scalp give dependable wound coverage Orticochea – incorporated multiple relaxing incisions in the galea to obtain additional flap length. May use scoring in perpendicular and parallel axis to gain both width and length (usually parallel) galeotomies has been confirmed to be useful for lengthening scalp flaps and for reducing tension on wound margins when closing scalp defects. Extreme care when scoring the galea to avoid injury to the BV that lie above the galea The flaps should be based on major vessels Indications for scalp flaps: 1. Defects of the hair-bearing area of the scalp not extending to dura. 2. Defects up to 200–300 cm2 in surface area. 3. Deep defects of the hair-bearing area of the scalp where quick cover is mandatory in patients who are not candidates for free flap transfer because of poor medical condition. Advantages of scalp flaps: 1. Use of local tissue. 2. Quick, easy, and safe dissection. 3. Flap reliability. Disadvantages of scalp flaps: 18 1. Flaps are not thick enough to fill deep defects. 2. Flaps are mostly hair-bearing and cannot be used for forehead reconstruction. 3. Flaps must be very carefully designed, otherwise the surgeon may not be able to cover large defects adequately because of the rigidity of the scalp tissues. 19 Temporoparietal Occipital flap (Juri Juri) 20 21 Distant flaps and free tissue transfer Pedicled flaps Three main pedicle flaps are 1) pec major 2) lat doesi 3) trapezius Lateral-inferior defects can be closed with the pec major or lat dorsi. Any defects higher than this can not be reached by theses two flaps Post inf occipital defect can be covered with a trapezius flap usually the post variant based on the perforators rather than the cervical artery Free flaps 1) omental falp(mobile and pliable) and ssg 2) facial flap – serratus 3) fasciocutaneous- radial forearm, scapular and parascapular 4) muscle – lat dorsi most common, serratus, gracillis rectus Tissue expansion Up to 50 % of the scalp can be resurfaced with expanders without changing the hair growth pattern or creating new donor defects If more skin is need to cover the wound the expanders can be left in place after the first advancement for reinflation and additional expansion at a later date (sequential expansion) Principles for expansion of the skull 1. slow 2. serial inflation 3. multiple expanders 4. choose the best expanders to fit specific areas 5. peripheral capsulotomy only main disadvantage of tissue expansion is the length of treatment, sometimes as long as 2 to 3 months and involving two or more operations. Pressure from the expander(s) on the cranial vault can also cause molding of the bones and even erosion of the skull, with potentially disastrous consequences. These bony changes are more pronounced in children, in whom nevertheless the skull will return to normal by 18 months. Expanders are placed in multiple locations adjacent to the leading edge of the defect shape of tissue expander bases affects the amount of tissue gain. Van Rappard et al. determined that expanders with a round base, a crescentic base, and a rectangular base give tissue gains of 25, 32, and 38 percent, respectively. A single large expander is preferred over multiple smaller expanders, as this will give the greatest gain in tissue per volume of expansion and minimize the infectious risk The incisions should be place perpendicular to the axis of expansion 22 Expansion begins at 10 – 14 d and repeated bi/weekly Estimating the amount of expansion necessary can be difficult The available area is calculated by measuring the distance over the expander and subtracting the distance of the base About 20 % of the measured expander skin is lost during advancement thus it is important to over expand by 20-30% Once maximal capsule has been met the expander is removed and the scalp flap s advanced The capsule is important for the blood supply of the expanded tissue and thus should be left insitu Careful scorning of the capsule can be done if needed for a further increase in length of the expanded flap Previously expanded scalp tissue can be re-expanded after 4-6 mnths The gain in length from the secondary expansion is less than the primary expansion 1. Total Scalp Avulsion Dramatic. Usually long hair caught in a machine. Usually includes forehead, eyebrows and part of the ears. Previously used to be treated by SSG. Now treated by replantation. A recent report from Japan (BJPS, 1996) describes a 3 team approach (one to clean the recipient area; one to clean the scalp and one to harvest vein grafts) Vein grafts were used in every case. Principles of Scalp Replantation 1. Adequate debridement, including clipping of hair. 2. Stable patient with traumatic blood loss replaced. 3. Up to 18 hrs of cold ischaemia can be tolerated. 4. Vascular anastomoses must all be outside the zone of injury. Thus need vein grafts 5. STA and vein are the largest. 6. Scalp can survive on one pedicle 7. . associated with significant blood loss and must be replaced 8. blood loss should be minimized by performing multiple venous anatomises 9. arterial anast first if warm ischemia time greater than 10 h 10. contraindications are inability to find art and vein and warm ischemia time greater than 10 H 23 Reconstruction of the bone When defects include full thickness calvarium need to adresss the need for calvarial recon Two schools of thought 1) reconst like lat dorsi provide a layer thick enough for protection 2) calvarial replacement is necessary to avoid complications of headache , dizziness and seizures options 1) alloplastic – methyl methacrylate, metal sheets, acrylic a. these have higher infection rates b. have adv of being prefabricated c. bone substitutes are also uses eg demineralised bone implants, hydroxyapatite, calcium phosphate and calcium sulphate 1) autogonous bony reconstruction- free bone grafts or vascularized bony reconstructions a. these are incorporated by creeping substitution but bone reabsorption can be can be unpredictable and significant and is related to the status of the recipient bed,, the type of donor bone(memb less reab than endochondral) b. split calvarial bone grafts - useful as can be moulded in kids and minimal donor site morbidity c. two technique for harvest d. in-vivo technique the outer table is split from the inner table e. ex-vivo technique a craniectomy is performed and the calvarial bone is split , the inner tableused for bone graft and the outer table used for the donor site a. split rib cranioplasty- ribs will regenerate if the periosteum left intact and donor morbidity minimal if no more than three or four ribs taken and pneumothorax avoided Ribs are difficult to mould and can reabsorb over time Radiotherapy wounds of the scalp Post rad wounds often develop from minor trauma and susceptible to infection which can then lead to necrosis Not suitable for local options as SSG, local flaps and direct closure as poor quality of tissue Only limited options and that is free muscle (better than free fascial as muscle better against infect as per mathes and chang) Underlying bone often involved and colonized by bacteria. If bone not grossly necrotic the cover by vasc tissue leads to replacement of the bone If necrotic then needs to be removed covered by free vasc tissue and then 3-6mnths later the bone graft inserted into the defect 24 REFERENCES McC SRPS 7 (15), 1995.