Document

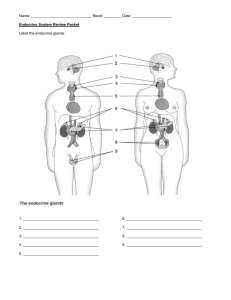
9.1 – The Glands and Hormones of the Endocrine System
(Taken from Biology 12, MHR)
The nervous system rapidly affects specific tissues, to which it is directly connected by neurons.
The endocrine system relies on chemical messengers called hormones, which circulate in the blood and have broad, long-lasting effects.
endocrine system: in vertebrates, system that works in parallel with the nervous system to maintain homeostasis by releasing chemical hormones from various glands; composed of the hormone-producing glands and tissues of the body
hormones: chemical messenger sent to many parts of the body to produce a specific effect on a target cell or organ
endocrine hormones: chemicals produced in glands and secreted directly into the blood.
The circulatory system carries the hormones to the various organs of the body.
Most hormones are distributed by the bloodstream to target cells. Target cells have receptors for the hormone, and the hormone combines with the receptor as a key fits a lock.
See Figure 9.3, pg 391
Chemical Control Systems
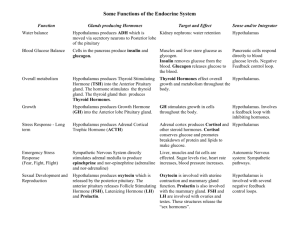
Along with the nervous system, the endocrine system provides integration and control of the organs and tissues. The nervous system enables the body to adjust quickly to changes in the environment. The endocrine system is designed to maintain control over a longer duration.
Hormones serve the body not as chemical products but as regulators, speeding up or slowing down certain bodily processes.
Chemical Signals: Steroid and Water-Soluble (Protein) Hormones
-
-
-
-
There are two types of hormones:
1) Steroid Hormones
made from cholesterol (a lipid compound) includes male and female sex hormones and cortisol composed of complex rings of carbon, hydrogen, and oxygen molecules not soluble in water but are soluble in fat
Steroid hormones can easily diffuse through the lipid bilayer of cell membranes and then into the target cells, where they combine with receptor molecules located in the cytoplasm.
-
-
The hormone-receptor complex then moves into the nucleus and attaches to a segment of chromatin that has a complementary shape.
The hormone activates a gene that sends a message to the ribosomes in the cytoplasm to begin producing a specific protein. (Figure 9.4A, pg 393)
-
-
-
-
-
-
2) Water-Soluble (Protein) Hormones
includes insulin and human growth hormone (hGH), epinephrine, and thyroxine (T
4
) contain chains of amino acids of varying length soluble in water
Water-soluble hormones cannot diffuse across the cell membrane.
Protein hormones exhibit a different action. They combine with receptors on the cell membrane.
Specific hormones combine at specific receptor sites.
Some of the protein hormones form a hormone-receptor complex that stimulates the conversion of adenosine triphosphate (ATP) into cyclic adenosine
-
Regulating the Regulators
monophosphate (cyclic AMP). cyclic AMP functions as a messenger, activating enzymes in the cytoplasm to carry out their normal functions. (Figure 9.4B, pg 393)
-
-
-
-
-
When the hypothalamus receives signals from various sensors in the body, it secretes releasing hormones which often travel to the pituitary gland.
The releasing hormones stimulate the pituitary gland to secrete hormones that act on other endocrine glands.
Tropic hormones are hormones that target endocrine glands and stimulate them to release other hormones.
Many hormones are regulated by negative feedback mechanisms.
See Figure 9.5, pg 394
Working Together to Maintain Homeostasis
-
-
-
-
Homeostasis depends on the close relationship between the nervous system and the endocrine system.
Some nervous system structures (e.g., hypothalamus) secrete hormones.
Several chemicals function as both neurotransmitters and hormones (e.g., epinephrine).
The endocrine and nervous systems are regulated by feedback loops.
The regulation of several physiological processes involves the nervous and endocrine systems acting together.
HOMEWORK: pg 395 #1 – 12
9.2 – Hormonal Regulation of Growth, Development, and Metabolism
(Taken from Biology 12, MHR, 2011)
The Pituitary Gland: The Master Gland
-
-
-
-
also referred to as the “master gland” because it controls other endocrine glands
Small sac-like structure that is connected by a stalk to the hypothalamus which is the area of the brain associated with homeostasis.
Interaction between nervous system and endocrine system is evident in the hypothalamus-pituitary complex.
The pituitary gland produces and stores hormones and the hypothalamus stimulates the release of hormones by the pituitary gland by way of nerves.
The pituitary gland is composed of separate lobes: the posterior lobe and the anterior lobe.
Posterior Lobe
-
-
-
-
Anterior Lobe
-
is considered part of the nervous system stores and releases hormones which have been produced by the hypothalamus (Ex: antidiuretic hormone, oxytocin)
Hormones travel by specialized nerve cells from the hypothalamus to the pituitary.
The pituitary gland stores the hormones releasing them into the blood when needed.
-
-
produces its own hormones produces and releases six major hormones: thyroid-stimulating hormone (TSH), adrenocorticotropic hormone (ACTH), prolactin (PRL), human growth hormone (hGH), follicle-stimulating hormone (FSH), and luteinizing hormone (LH) hypothalamus regulates the release of hormones from the anterior pituitary these hormones activate specific cells in the pituitary, causing the release of pituitary hormones, which are then carried to target tissues through the blood.
Some hypothalamus hormones inhibit the secretion of hormones from the anterior pituitary
Ex:
Dopamine inhibits the secretion of prolactin (PRL), a pituitary hormone that stimulates milk production in women who have given birth.
Somatostatin inhibits the secretion of somatotropin, the pituitary hormone associated with growth of long bones.
See Figure 9.7, pg 397
Human Growth Hormone
-
-
The anterior pituitary produces and secretes human growth hormone (hGH) to regulate growth, development, and metabolism.
Human growth hormone (hGH) stimulates the liver to secrete hormones called
growth factors.
-
-
-
Growth factors along with hGH influence many physiological processes including:
protein synthesis
cell division and growth, especially the growth of cartilage, bone, and muscle
metabolic breakdown and release of fats stored in adipose (fat) tissue. hGH causes the elongation of bones by stimulating the growth of muscles, connective tissue and the growth plates at the end of long bones.
Too much hGH during childhood can result in gigantism and too little hGH during childhood can result in dwarfism.
-
-
-
See Figure 9.9, pg 398
Overproduction of hGH in adults can lead to a condition called acromegaly.
Excess hGH can no longer cause an increase in height so the bones and soft tissues of the body widen.
See Figure 9.10, pg 399 -
The Thyroid Gland: A Metabolic Thermostat
Located at the base of the neck, immediately below the larynx (voice box) and in front of the trachea or windpipe.
One important thyroid hormone is thyroxine (T
4
) which increases the rate at which the body metabolizes fats, proteins, and carbohydrates for energy.
Hyperthyroidism is a condition caused by the thyroid producing extremely high levels of thyroxine.
Individuals who secrete higher levels of thyroxine oxidize sugars and other nutrients at a faster rate. These individuals tend not to gain weight.
Hypothyroidism is a condition caused by the thyroid producing extremely low levels of thyroxine.
Individuals who have lower levels of thyroxine do not oxidize nutrients as quickly and therefore tend not to break down sugars as quickly. Excess sugar is eventually converted into fat. These individuals tend to experience weight gain, muscle weakness, cold intolerance, and dry skin and hair.
Thyroxine secretion is controlled by negative feedback.
See Figure 9.12, pg 401
If there is a decrease in metabolic rate, receptors in the hypothalamus are activated.
Nerve cells in the hypothalamus secrete thyroid-releasing hormone (TRH), which stimulates the pituitary to release thyroid-stimulating hormone (TSH).
TSH is carried by the blood to the thyroid gland, which, in turn releases thyroxine.
Thyroxine raises metabolism by stimulating increased sugar utilization by body cells.
Higher levels of thyroxine inhibits the release of TRH from the hypothalamus, thus turning off the production of TSH from the pituitary.
The Thyroid Gland and Calcitonin
The thyroid gland also produces calcitonin which lowers calcium levels in the blood.
When the concentration of calcium in the blood rises too high, calcitonin stimulates the uptake of calcium into bones, which lowers its concentration in the blood.
See Figure 9.13, pg 403
Thyroid Disorders
The thyroid gland requires iodine to make the thyroid hormones.
When inadequate amounts of iodine are obtained from the diet, the thyroid enlarges, producing a goiter. A goiter appears as a swelling in the neck area.
Without iodine, thyroid production and secretion of thyroxine drops. This causes more and more TSH to be produced.
As a result of the high TSH levels, cells of the thyroid continue to develop, and the thyroid enlarges.
Goiters are very uncommon in Canada since the salt we cook with is iodized (iodine added).
Other sources of iodine include seafood, fish (cod, haddock, and perch), kelp and dairy products.
Parathyroid Glands
The parathyroid glands are four small glands attached to the thyroid.
They maintain homeostasis by responding directly to chemical changes in their immediate surroundings.
Example: low calcium levels in the blood
Stimulates the release of parathyroid hormone (PTH)
A rise in PTH levels causes the calcium levels in the blood to increase and phosphate levels to decrease.
The hormone does this by acting on 3 different organs: the kidneys, the intestines, and the bones.
PTH causes the kidneys and intestines to retain calcium while promoting calcium release from bone.
Once PTH levels have elevated calcium levels, the release of PTH is inhibited.
Calcium levels signal both the release and inhibition of PTH.
See Figure 9.13, pg 402
HOMEWORK: pg 403 #1 - 11
9.3 – Hormonal Regulation of the Stress Response and Blood Sugar
-
-
-
When an inhibitor of stress is identified, both the endocrine system and nervous system make adjustments that enable the body to cope with the problem.
Nervous system adjusts rapidly to stress by increasing heart rate and diverting blood to the needed muscles.
Endocrine system’s response is somewhat slower however, the hormones provide a more sustained response to the stimulus.
Adrenal Glands
-
-
-
-
The Adrenal Medulla: Regulating the Short-Term Stress Response
located above each kidney made up of inner gland, the adrenal medulla, which is surrounded by an outer casing called the adrenal cortex adrenal medulla regulated by the nervous system adrenal cortex regulated by hormones
-
-
-
-
-
-
In response to a stressor, neurons in the sympathetic nervous system carry a signal from the hypothalamus directly to the adrenal medulla.
Epinephrine (adrenaline) and norepinephrine (noradrenaline) are released from the adrenal medulla into the blood – this causes blood sugar levels to rise promotes the conversion of glycogen to glucose for energy
These hormones regulate a short-term stress response that is commonly called the fight-or-flight response. these hormones also increase heart rate, breathing rate, and cell metabolism
See Figure 9.16, pg 405
The Adrenal Cortex: Regulating the Long-Term Stress Response
-
-
adrenal cortex produces 3 different types of hormones: glucocorticoids, mineralocorticoids, and gonadocorticoids
glucocorticoids increase blood sugar
mineralocorticoids increase blood pressure
gonadocorticoids supplement hormones produced by the gonads (testes and ovaries)
Cortisol
-
-
-
-
-
-
cortisol is a steroid hormone synthesized from cholesterol most important glucocorticoid is cortisol which promotes the conversion of amino acids into glucose to help body recover from stress brings about an increase in blood sugar in response to stress promotes the breakdown of fats into fatty acids which also releases glucose decreases glucose uptake by the muscles (not by the brain) long-term stress response hypothalamus sends message to anterior pituitary which secretes ACTH (adrenocorticotropic hormone)
-
-
-
-
-
-
-
-
ACTH is carried in the blood to adrenal cortex.
Adrenal cortex secretes glucocorticoids (cortisol) and mineralocorticoids
(aldosterone).
Increased levels of cortisol in the blood cause negative feedback on the hypothalamus and anterior pituitary, which stops ACTH production, and stops the release of cortisol.
See Figure 9.18, pg 407
Cortisol is a natural anti-inflammatory in the body and suppresses the action of the
immune system.
This is probably why sustained high levels of cortisol make people more susceptible to infections.
Aldosterone
-
-
The main mineralocorticoid is the hormone aldosterone.
Aldosterone stimulates the kidneys to increase the absorption of sodium into the blood.
This increase in solute concentration causes water to diffuse from the kidneys into the blood. This raises blood pressure.
The nervous system activates the rennin-angiotensin-aldosterone pathway in response to reduced blood flow to the kidneys.
By increasing Na + reabsorption, the kidneys help maintain increased fluid volume.
This helps sustain adequate blood pressure during stress.
The Hormones of the Pancreas
-
-
-
-
-
-
-
-
-
The pancreas contains two types of cells: one type produces digestive enzymes; the other type produce hormones.
Hormone-producing cells are located in structures called the islets of Langerhans.
The islets contain beta and alpha cells that are responsible for the production of two hormones: insulin and glucagon.
Insulin is produced in the beta cells of the islets of Langerhans and is released when the blood sugar level increases.
Insulin causes a decrease in the blood sugar level in three ways:
liver stores glucose as glycogen
muscle cells store glycogen and build protein
adipose (fat) tissue uses glucose to form fat
Glucagon is produced in the alpha cells of the islets of Langerhans and is released when blood sugar levels are low, such as after periods of fasting.
Glucagon causes an increase in the blood sugar level in a few ways:
liver breaks down glycogen to glucose
adipose tissue breaks down fat to glucose
Both insulin and glucagon are regulated by negative feedback systems.
See Figure 9.20, pg 409
Diabetes
-
-
-
Diabetes is a chronic disease affecting more than 2 million Canadians.
Diabetes results when the body does not produce enough insulin or does not respond properly to insulin.
Without adequate levels of insulin, blood sugar levels tend to rise very sharply after
-
-
-
meals. This is known as hyperglycemia or high blood sugar.
With hyperglycemia, the kidneys are unable to reabsorb all the blood glucose that is filtered through them, so glucose appears in the urine.
Since excretion of glucose draws water from the body by osmosis, people with diabetes excrete usually large volumes of urine and are often thirsty.
Other symptoms include:
low energy levels
acetone (an intermediary product of fat metabolism) can change blood pH
in severe cases, doctors can smell acetone on the breath of people with diabetes
If left untreated, diabetes can cause blindness, kidney failure, nerve damage, and non-traumatic limb amputation.
1) Type 1 Diabetes
autoimmune disease
immune system produces antibodies that attack and destroy the beta cells of the pancreas
occurs when the pancreas is unable to produce insulin because of early degeneration of the beta cells in the islets of Langerhans
juvenile-onset diabetes / insulin-dependent diabetes
diagnosed in childhood and people must take insulin to live
10% of people with diabetes have type 1 diabetes
2) Type 2 Diabetes
insulin receptors on the body’s cells stop responding to insulin
associated with decreased insulin production or ineffective use of the insulin that the body does produce
known as insulin resistance
adult-onset diabetes
diagnosed in adulthood and can be controlled with diet, exercise, and oral drugs known as sulfonamides
90% of people with diabetes have type 2 diabetes
Type 2 diabetes is linked closely to unhealthy diet and weight gain
Gestational Diabetes
temporary condition that occurs in 2% to 4% of pregnancies
it increases the risk of diabetes in both mother and child
Toward a Cure for Diabetes
Banting and Best
-
-
-
-
-
In 1921, Frederick Banting (a doctor) and Charles Best (a graduate student in biochemistry at the University of Toronto) were assigned a makeshift laboratory by professor John J.R. MacLeod.
At that time, diabetes was thought to be caused by a deficiency of a hormone located in specialized cells of the pancreas.
Banting and Best wanted to isolate the hormone.
They tied the pancreatic duct of dogs and waited seven weeks for the pancreas to shrivel. The hormone was then extracted from the pancreas.
-
-
When the hormone was injected into dogs that had had their pancreas removed, symptoms of diabetes ceased.
Banting and Best wanted to call the hormone isletin, but MacLeod insisted that it be called insulin.
In 1923, Banting and MacLeod were awarded the Nobel Prize for physiology and medicine. Banting was furious that his partner, Best was not included and that
MacLeod got the glory instead.
-
-
-
Today, synthetic insulin is produced by genetically engineered bacteria and other organisms.
Edmonton Protocol has pioneered the first successful islet cell transplant to restore functioning beta cells to the pancreas.
Digital blood monitors are now used to test blood glucose and insulin pumps are often used for insulin injections.
HOMEWORK: pg 413 #1-11
9.4 – Hormonal Regulation of the Reproductive System
(Taken from Biology 12, MHR, 2011)
Sex hormones work to stimulate the development of male and female reproductive systems and regulate the function of the mature reproductive system.
In males, the main sex hormone is testosterone. In females, the main sex hormones are estrogen and progesterone.
In the male reproductive system, a negative feedback hormone system maintains a relatively constant level of sperm production and testosterone.
In females, hormone systems interact to regulate the monthly menstrual cycle.
The Male Reproductive System
male sex hormone testosterone
stimulates the production of mature sperm cells
influences the development of secondary male sexual characteristics at puberty
(maturation of testes and penis, growth of facial and body hair, lowering of the voice, strengthening of muscles)
associated with sex drive
increases secretion of body oils
-
-
Anabolic steroids mimic the action of testosterone in promoting muscle development.
Over use of anabolic steroids can have a number of side effects including shrinking testicles, low sperm count, and the development of breasts.
-
-
-
-
-
-
-
-
-
-
At puberty, the hypothalamus secretes the gonadotropin-releasing hormone
(GnRH) which activates the pituitary gland to secrete and release the male follicle-
stimulating hormone (FSH) and the male luteinizing hormone (LH).
The FSH stimulates the production of sperm cells in the seminiferous tubules of the testes.
At the same time, FSH causes cells in the seminiferous tubules to release a hormone called inhibin.
Inhibin acts on the anterior pituitary gland to inhibit the production of FSH. The result is a negative feedback system.
LH promotes the production of testosterone by the interstitial cells.
Testosterone increases sperm production.
Once high levels of testosterone are detected by the hypothalamus, a negative feedback system is activated.
Testosterone inhibits LH production by the pituitary by deactivating the hypothalamus.
Hypothalamus releases less GnRH, leading to a decrease in LH production which in turn leads to less testosterone production.
See Figure 9.23, pg 414 and Figure 9.25, pg 417
Aging and the Male Reproductive System
Most men experience a gradual decline in their testosterone levels at around
age 40. This condition is called andropause.
Other hormonal changes can occur with age for example, the enlarging of the
prostate gland.
The risk of prostate cancer also increases with age.
The Female Reproductive System
Menstrual Cycle
-
-
-
The menstrual cycle ensures that an ovum is released at the same time as the uterus is most receptive to a fertilized egg.
The human female menstrual cycle takes an average of 28 days.
The menstrual cycle begins with menstruation and ends with the start of the next
-
-
-
-
menstrual period.
The menstrual cycle actually consists of two separate interconnected cycles.
One cycle takes place in the ovaries and is known as the ovarian cycle.
The other cycle takes place in the uterus and is known as the uterine cycle.
Both cycles are controlled by the female sex hormones estrogen and
progesterone, which are produced in the ovaries.
See Figure 9.26, pg 418 and Figure 9.27, pg 420
The menstrual cycle can be divided into four distinct phases:
1) Flow Phase
shedding of the endometrium, or menstruation
lasts for approximately 5 days
2) Follicular Phase
characterized by the development of follicles within the ovary
as follicle cells develop, the hormone estrogen is secreted
estrogen activates the development of female secondary sex characteristics
(development of breasts, body hair, increased thickening of endometrium)
normally takes place between days 6 and 13 of menstrual cycle
3) Ovulatory Phase (Ovulation)
the egg bursts from the ovary and follicular cells differentiate into the corpus luteum
normally takes place on day 14 of menstrual cycle
4) Luteal Phase
characterized by the formation of the corpus luteum following ovulation
corpus luteum secretes both estrogen and progesterone
progesterone stimulates the endometrium and prepares the uterus to receive a fertilized egg
it also inhibits further ovulation and prevents uterine contractions
occurs between days 15 and 28 of menstrual cycle
-
-
If fertilization does not occur, the concentrations of estrogen and progesterone will decrease, causing weak uterine contractions which in turn, cause the shedding of the endometrium.
This marks the beginning of the next flow phase, and the female menstrual cycle starts all over again.
The Ovarian Cycle
-
-
-
In a single ovarian cycle, one follicle matures, releases an ovum, and then develops into a yellowish, gland-like structure as a corpus luteum. The corpus luteum then degenerates.
See Figure 9.27, pg 420 and Figure 9.28, pg 421
The ovarian cycle can be divided into two stages: follicular stage and luteal stage.
Follicular Stage
-
-
-
The onset of puberty in females is signaled by the release of gonadotropin-
releasing hormone (GnRH) from the hypothalamus which activates the pituitary gland, the storage site of female follicle-stimulating hormone (FSH) and female
luteinizing hormone (LH).
During the follicular stage of the menstrual cycle, blood carries FSH to the ovary, where follicle development is stimulated.
The follicles within the ovary secrete estrogen, which initiates the development of the endometrium.
-
-
-
Luteal Stage
-
The increase in estrogen levels results in a negative feedback message being sent to the anterior pituitary gland to turn off secretions of FSH.
At the same time, the rise in estrogen exerts a positive message on the LH-producing cells of pituitary gland. LH secretion rises and ovulation occurs.
Ovulation marks the end of the follicular stage and the beginning of the luteal stage.
-
-
-
-
Under the influence of LH, the remaining follicular cells form the corpus luteum, which produces progesterone and some estrogen.
As progesterone and estrogen build up in the body, a second negative feedback mechanism is activated.
Progesterone and estrogen work together to inhibit the release of both FSH and LH.
Without FSH and LH, the corpus luteum begins to deteriorate, slowing estrogen and progesterone production which in turn signals the beginning of menstruation.
The Uterine Cycle
-
-
-
The uterine cycle is closely related to the ovarian cycle.
See Figure 9.29, pg 422
The uterine cycle begins on the first day of menstruation. At this time, the corpus luteum has degenerated and the levels of the sex hormones in the blood are low.
-
-
At the end of menstruation (around day 5), the endometrium is very thin.
As a new follicle begins to mature and release estrogen, the level of estrogen in the blood increases.
Around day 6, the estrogen level has increased enough to cause the endometrium to begin thickening.
-
-
-
Aging and the Menstrual Cycle
-
-
-
-
After ovulation, the release of progesterone by the corpus luteum causes more thickening of the endometrium.
If fertilization does not occur, the corpus luteum degenerates.
The levels of the sex hormones drop, the endometrium breaks down and menstruation begins again.
-
The number of functional follicles in females decreases with age.
This leads to a decrease in the amount of estrogen and progesterone in the blood.
As the hormone levels drop, a women’s menstrual cycle becomes irregular.
Menopause marks the end of a female’s reproductive life and signals the end of the menstrual cycle.
The decrease in the sex hormones have a number of effects on the body including:
“hot flashes”, mood changes, increase in cholesterol levels, decrease in bone mass, increased risk of uterine cancer, breast cancer, and heart disease.
Hormone Replacement Therapy
-
-
Hormone replacement therapy (HRT) is the administration of low levels of estrogen and/or progesterone to alleviate symptoms of menopause.
Although HRT can be very helpful in alleviate symptoms of menopause, it has been linked to: increased risk of coronary heart disease and strokes, increased risk of cancer, and increased risk of dementia.
HOMEWORK: pg 425 #1 - 12
Table 9.2, pg 424
Summary of Key Reproductive Hormones and Their Functions
Hormone Production
Site
Target
Organ(s)
Function in Male
Reproductive
System
Function in
Female
Reproductive
System
Gonadotropinreleasing hormone
(GnRH)
Folliclestimulating hormone (FSH)
Luteinizing hormone (LH)
Estrogen
Progesterone
Testosterone
Inhibin
Hypothalamus
Anterior pituitary Ovaries and testes
Anterior pituitary Ovaries and testes
Ovary (follicle) Entire body
Ovary (corpus luteum)
Testes
(interstitial cells)
Testes
(seminiferous tubules)
Anterior pituitary gland
Uterus
Entire body
Anterior pituitary and hypothalamus
Stimulates the release of FSH and
LH from the anterior pituitary
Stimulates the development of the sex organs and gamete production
Stimulates the production of testosterone
Minor
Minor
Stimulates the development of the male reproductive tract and secondary sex characteristics
Inhibits FSH production
Stimulates the release of FSH and LH from the anterior pituitary
Stimulates the development of the sex organs and gamete production
Triggers ovulation, and
(with FSH) stimulates estrogen production
Stimulates the development of the female reproductive tract and secondary sex characteristics
Causes uterine thickening
Minor
Inhibits FSH production
The Principal Endocrine Glands and Some of Their Hormones
(Table 9.1, pg 392, Biology 12, MHR)
Endocrine
Gland
Hormone Secreted Effects of Hormones on Target
Tissue/Organs
Hypothalamus Hypothalamus releasing and inhibiting hormones
Thyroid-stimulating hormone
(TSH)
Regulates anterior pituitary hormones
Anterior pituitary Human growth hormone (hGH) Stimulates cell division, bone and muscle growth, and metabolic functions
Stimulates the thyroid gland
Adrenocorticotropic hormone
(ACTH)
Follicle-stimulating hormone
(FSH)
Luteinizing hormone (LH)
Stimulates the adrenal cortex to secrete glucocorticoids
Stimulates production of ova and sperm from the ovaries and testes
Stimulates sex hormone production from the ovaries and testes
Posterior pituitary
Thyroid
Prolactin (PRL)
Antidiuretic hormone (ADH)
Oxytocin (OCT)
Thyroxine (T
Calcitonin
4
)
Stimulates milk production from the mammary glands
Promotes the retention of water by the kidneys
Stimulates uterine muscle contractions and release of milk by the mammary glands
Affects all tissues; increases metabolic rate and regulates growth and development
Targets bones and kidneys to lower blood calcium by inhibiting release of calcium from bone and reabsorption of calcium by kidneys
Parathyroid
Adrenal cortex
Parathyroid hormone (PTH)
Glucocorticoids (e.g., cortisol)
Mineralocorticoids (e.g., aldosterone)
Gonadocorticoids
Promotes reabsorption of sodium and water by the kidneys
Promotes secondary sexual characteristics
Adrenal medulla Epinephrine and norepinephrine Flight-or-flight response
Pancreas Insulin
Raises blood calcium levels by stimulating the bone cells to release calcium, the intestine to absorb calcium from food, and the kidneys to reabsorb calcium
Stimulates tissues to raise blood glucose and break down protein
Ovaries
Testes
Glucagon
Estrogen
Progesterone
Testosterone
Lowers blood glucose levels and promotes the formation of glycogen in the liver
Raises blood glucose levels by converting glycogen in liver to glucose
Stimulates uterine lining growth and promotes development of the female secondary sexual characteristics
Promotes growth of the uterine lining and prevents uterine muscle contractions
Promotes sperm formation and development of the male secondary sexual characteristics