our registration form
advertisement

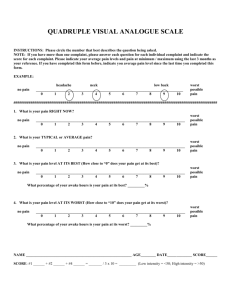
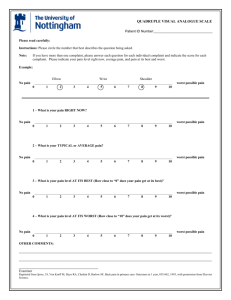
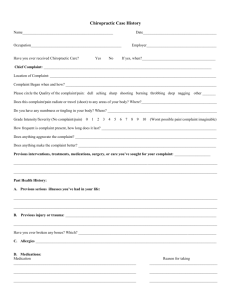
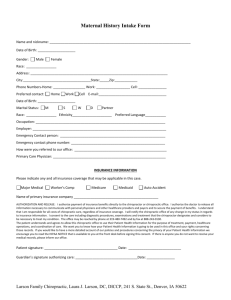
West Family Chiropractic Confidential New Patient Intake Form (Please Print) Today’ Date_______/______/_______ (Office use only) Chart Number_______________________ Patient Information Mr./ Mrs./ Ms. Name Miss. / Dr./….. Mailing Address Birth Date / / Age / Cell Phone ( ) Nick Name City Marital status State Social security # S /M /D / W Fax ( ) Race Zip Home phone Work phone ( ( E-mail Address ) ) Preferred method of contact Occupation. Employer Employer Address Primary Care Physician (PCP) PCP Address PCP Phone ( ) Who referred you to our office? Family Spouse Information Spouses Name Number of Children Insurance Information Are You Insured ? Yes No [ If Yes please present your insurance card(s) to the front desk ] Subscriber (The person who the insurance is through) Subscribers Birth Date / / / Personal, Automobile or Work Related Injury Information *** If this a Personal, Automobile or Work Related injury please fill out additional forms at the front desk ****** Please continue on the next page ****** Page 1 of 4 West Family Chiropractic Confidential New Patient Intake Form (Please Print) Name:_____________________________________________ (Office use only) Chart Number________________ Health history What is your main complaint? How long have you had this complaint? What do you think caused your current problem? Have you ever had this complaint before? Yes No Have you seen other practitioners for this complaint? Have you had chiropractic care before? Yes No (If yes please list) Yes No (If yes please list) (If yes please list) Please mark the areas on the picture below that correspond to the areas of the body where you feel the described sensations. Use appropriate symbols. Mark areas of radiation. Include all affected areas. Do not simply circle the area of involvement please Numbness ----- Pins & needles oooooo Burning xxxxx Aching Stabbing ///// ****** Please continue on the next page ****** Page 2 of 4 West Family Chiropractic Confidential New Patient Intake Form (Please Print) Name:_____________________________________________ (Office use only) Chart Number________________ Pain Assessment: Quadruple Visual Analogue Scale Instructions: Please CIRCLE the number that best describes the question being asked Note: If you have MORE than one complaint, please answer each question for each individual complaint and indicate the score for each complaint. For example: If you have neck & low back complaints circle the pain level for EACH of those complaints What is your pain right now? No Pain |________________________________________________________| 0 1 2 3 4 5 6 7 8 9 10 Worst possible pain What is your Typical or Average pain? No Pain |________________________________________________________| 0 1 2 3 4 5 6 7 8 9 10 Worst possible pain What is your pain level at its best (How close to “0” does your pain get at its best)? No Pain |________________________________________________________| 0 1 2 3 4 5 6 7 8 9 10 Worst possible pain What is your pain at its worst (How close to “10” does your pain get at its worst? No Pain |________________________________________________________| 0 1 2 3 4 5 6 7 8 9 10 Worst possible pain ****** Please continue on the next page ****** Page 3 of 4 West Family Chiropractic Confidential New Patient Intake Form (Please Print) Name:_____________________________________________ (Office use only) Chart Number________________ Health history Cont… Please list any other current health conditions Please list any history of surgeries Please list current medications Any allergies to medications? Please list current vitamins and supplements Please list any other physicians / Practitioners that you currently see Have you been diagnosed with Hypertension? If yes, please describe Have you been diagnosed with Diabetes? If yes, are you type 1 or 2? Any other comments about your diabetes? Do you currently smoke tobacco of any kind? Y / N Are you interested in quitting? Y / N If NO, have you had a past history of smoking? Y / N If yes, everyday or sometimes? I certify that the above information is correct to the best of my knowledge. Signature: __________________________________________ Date_____ /______/______ Page 4 of 4