2011 ANNUAL REPORT ON THE DRUG SITUATION BOSNIA AND HERZEGOVINA Prepared within the EMCDDA — IPA3 Project September 2011 Contributing authors: Milana Skipina, Department for the suppression of the abuse of narcotic drugs, Ministry of Security of Bosnia and Herzegovina, chair of national advisory group and coordinator for the group of authors Sabina Sahman- Salihbegovic, Ministry of Civil Affairs of Bosnia and Herzegovina Jasmin Pljevljak, Department for the suppression of the abuse of narcotic drugs, Ministry of Security of Bosnia and Herzegovina Nermana Mehic–Basara, Federal Ministry of Health of the Federation of Bosnia and Herzegovina Jelena Niskanovic, Institute for Public Health of the Republic of Srpska Nera Zivlak-Radulovic, Ministry of Health of the Republic of Srpska Nermin Sarajlic, Institute for Forensic Medicine and Forensic Toxicology, Medical Faculty of University of Sarajevo, the Federation of Bosnia and Herzegovina Aida Pilav, Ministry of Health of the Federation of Bosnia and Herzegovina Administrative support and technical editor: Sladjana Vaskovic, Ministry of Security of Bosnia and Herzegovina Editors: Viktor Mravcik, Head of the Czech National Focal Point for Drugs and Drug Addiction Alan Lodwick, Head of the UK National Focal Point for Drugs and Drug Addiction Thanks are also extended to Michael Donmall for his assistance in the analysis of data from treatment registers. English proofreading: Profis d.o.o. Sarajevo Contents SUMMARY ............................................................................................................................... 1 1. DRUG POLICY: LEGISLATION, STRATEGIES AND ECONOMIC ANALYSIS ................................ 3 1.1 1.2 1.3 1.4 2. DRUG USE IN THE GENERAL POPULATION AND SPECIFIC TARGETED GROUPS .................... 9 2.1 2.2 2.3 2.4 3. INTRODUCTION .................................................................................................................................. 23 TREATMENT STRATEGY AND POLICY ....................................................................................................... 23 TREATMENT SYSTEM ........................................................................................................................... 24 TRENDS AND CHARACTERISTICS OF TREATED CLIENTS ................................................................................ 26 HEALTH CORRELATES AND CONSEQUENCES .....................................................................33 6.1 6.2 6.3 6.4 7. INTRODUCTION .................................................................................................................................. 18 PREVALENCE ESTIMATES OF PROBLEM DRUG USE ..................................................................................... 18 DATA ON PROBLEM DRUG USERS FROM NON-TREATMENT SOURCES............................................................ 18 OTHER INTENSIVE, FREQUENT, LONG-TERM AND PROBLEMATIC FORMS OF DRUG USE .................................... 22 DRUG–RELATED TREATMENT DEMAND AND AVAILABILITY ..............................................23 5.1 5.2 5.3 5.4 6. INTRODUCTION .................................................................................................................................. 14 UNIVERSAL PREVENTION ..................................................................................................................... 14 SELECTIVE AND INDICATED PREVENTION IN AT-RISKS GROUPS AND INDIVIDUALS ............................................ 15 NATIONAL AND LOCAL MEDIA CAMPAIGNS ............................................................................................. 16 EVALUATION OF PREVENTION ACTIVITIES ................................................................................................ 17 PROBLEM DRUG USE ........................................................................................................18 4.1 4.2 4.3 4.4 5. INTRODUCTION .................................................................................................................................... 9 DRUG USE IN THE GENERAL POPULATION.................................................................................................. 9 DRUG USE IN THE SCHOOL AND YOUTH POPULATION ................................................................................ 10 DRUG USE AMONG TARGETED GROUPS .................................................................................................. 12 PREVENTION ....................................................................................................................14 3.1 3.2 3.3 3.4 3.5 4. INTRODUCTION .................................................................................................................................... 3 LEGAL FRAMEWORK.............................................................................................................................. 3 NATIONAL ACTION PLAN, STRATEGY, EVALUATION AND COORDINATION ....................................................... 5 ECONOMIC ANALYSIS ............................................................................................................................ 7 INTRODUCTION .................................................................................................................................. 33 DRUG RELATED INFECTIOUS DISEASES .................................................................................................... 33 OTHER DRUG-RELATED HEALTH CORRELATES AND CONSEQUENCES ............................................................. 35 DRUG RELATED DEATHS AND MORTALITY OF DRUG USERS ......................................................................... 36 RESPONSES TO HEALTH CORRELATES AND CONSEQUENCES .............................................39 7.1 INTRODUCTION .................................................................................................................................. 39 7.2 7.3 7.4 8. PREVENTION OF DRUG RELATED EMERGENCIES AND REDUCTION OF DRUG-RELATED DEATHS ........................... 39 PREVENTION AND TREATMENT OF DRUG-RELATED INFECTIOUS DISEASES ..................................................... 39 RESPONSES TO OTHER HEALTH CORRELATES AND CONSEQUENCES .............................................................. 42 SOCIAL CORRELATES AND SOCIAL REINTEGRATION ..........................................................43 8.1 8.2 8.3 9. INTRODUCTION .................................................................................................................................. 43 SOCIAL EXCLUSION AND DRUG USE ........................................................................................................ 43 SOCIAL REINTEGRATION....................................................................................................................... 43 DRUG-RELATED CRIME, PREVENTION OF DRUG RELATED CRIME AND PRISON ..................44 9.1 9.2 9.3 9.4 9.5 9.6 9.7 10. 10.1 10.2 10.3 10.4 INTRODUCTION .................................................................................................................................. 44 DRUG-RELATED CRIME ........................................................................................................................ 44 PREVENTION OF DRUG-RELATED CRIME .................................................................................................. 45 INTERVENTIONS IN THE CRIMINAL JUSTICE SYSTEM ................................................................................... 45 DRUG USE AND PROBLEM DRUG USE IN PRISONS ..................................................................................... 46 RESPONSES TO DRUG RELATED HEALTH ISSUES IN PRISONS......................................................................... 47 REINTEGRATION OF DRUG USERS AFTER RELEASE FROM PRISON.................................................................. 48 DRUG MARKETS ...........................................................................................................49 INTRODUCTION .................................................................................................................................. 49 AVAILABILITY AND SUPPLY ................................................................................................................... 49 SEIZURES .......................................................................................................................................... 50 PRICE AND PURITY .............................................................................................................................. 50 ANNEXES ................................................................................................................................51 ABBREVIATIONS ............................................................................................................................................. 51 LIST OF TABLES .............................................................................................................................................. 52 LIST OF FIGURES ............................................................................................................................................ 53 INDEX .......................................................................................................................................................... 54 BIBLIOGRAPHY ............................................................................................................................................... 55 Summary The main law concerning illicit drugs is the Law on the Prevention and Suppression of Abuse of Narcotic Drugs which came into force in 2006. It provides for establishment of special bodies in this field, the classification of plants and narcotic and psychotropic substances and a framework of measures for counteracting drug crime, In 2010 an amendment of the law was drafted which is dues for adoption in 2011. The amendments provide for clarification of procedures and responsibilities, the establishment of an Office of Drugs and regulations concerning post-mortem toxicological analysis and recording of drug related deaths. There are criminal codes at state and entity levels defining offences related to drugs and the possession of drugs for personal use is not allowed in BiH. A National Strategy on Supervision over Narcotic Drugs, Prevention and Suppression of the Abuse of Narcotic Drugs in Bosnia and Herzegovina for the period 2009-2013 is the first ever drug strategy in BiH. It is followed by an Action Plan covering the same period which sets specific objectives, activities and indicators. At the end of 2010, an intermediate evaluation report on the Action Plan was produced by the Commission on Narcotic Drugs, which is the main inter-Ministerial co-ordination body in the field of drugs. The Department for the suppression of the abuse of narcotic drugs at the Ministry of Security is responsible for day-to-day co-ordination as well as for monitoring the drug situation. Total expenditure on drug policy has not yet been estimated, however the annual cost of drug-related treatment, social rehabilitation and harm reduction at the state level has been very approximately estimated at 18.0 mil. BAM (i.e. 9.2 mil. €). No recent data are available on the prevalence of drug use in the adult population. However, a Health Survey was conducted in the Republic of Srpska in 2010, including questions on illicit drug use, and similar surveys are planned in the Federation of Bosnia and Herzegovina. Results will be presented in future annual reports. ESPAD surveys were conducted in both entities for the first time in 2008. Cannabis, volatile substances and sedatives were the most prevalent substances in both entities. The survey was repeated in the Republic of Srpska in spring 2011 and is planned to take place in the Federation of Bosnia and Herzegovina in November 2011. There is no state-wide uniform prevention programme on substance use, however prevention programmes, including school prevention, are implemented at the local and regional levels with the frequent involvement of NGOs. The Health and Social Protection systems are involved in prevention measures focusing on at risk individuals, families and other groups. It is estimated that there are 7,500 injecting drug users (IDUs) in BiH which represents approximately 0.3% of the population aged 15-64. Surveys suggest that the average age of IDUs is about 30 years, around 90% of them are male and the vast majority inject heroin. One-third of surveyed IDUs reported needle sharing within the last month and recently a positive trend has been observed in increasing safe injection practices, safer sexual behaviour and more contact with harm reduction services. Addiction treatment within the health system is available from eight specialised centres, a network of nearly 60 community mental health centres and also from general practitioners. In addition there are 1 eleven rehabilitation centres which follow the principles of therapeutic communities. Medical treatment is available in both inpatient and outpatient settings. Opioid substitution treatment, using methadone and also, recently, buprenorphine, is available in the eight specialised centres. In 2010 1,544 patients were reported as presenting to the eight specialised treatment centres, 364 of them for the first time in their life (23.6% of the total). The average age of clients was nearly 30 years, 92% were male and the primary substance was predominantly opiates followed by cannabis. Of the total number of clients, 1,183 were in substitution treatment. In 2010, a further 364 clients presented for treatment to therapeutic communities. Up to the end of 2009, 163 HIV-positive individuals had been registered in BiH, 21 of whom (13%) were IDUs. Prevalence studies carried out amongst IDUs in 2007 and 2009 showed prevalence of HIV below 1% and HCV prevalence ranging from around 20% to 50% in the three cities studied. Amongst clients in opioid substitution treatment HCV prevalence was 37% in 2010. Data on drug related deaths collected from forensic medicine departments and district prosecutors’ offices covering about 30% of the population of BiH show that there were a total of eight fatal drug overdoses in 2010, five of them due to illegal drugs. Six cases were male and two female, and all occurred to individuals aged between 20 and 34. There are seven drop in centres providing harm reduction interventions, including injecting equipment distribution and exchange, information provision, counselling, outreach work and distribution of condoms for injecting drug users. Various law enforcement agencies reported a total of 1,300 drug law offences in BiH in 2010. Between 30% and 70% of prisoners are estimated to be dependent on drugs. However specialised drug treatment is not yet available in prisons and there is no general drug strategy or policy for prison settings. Increasingly NGOs are involved in provision of services to prisoners both in prison and post-release. Bosnia and Herzegovina has similar problems to other countries on the “Balkan route” and is a transit country for synthetic drugs and cocaine from the west and heroin and cannabis from the east. The only drug produced in Bosnia and Herzegovina is cannabis with increasing indoor cultivation of genetically modified potent strains of the cannabis plant. 26.5 kilos of heroin, 1.5 kilos each of cocaine and amphetamine and 465.6 kilos of herbal cannabis were seized in 2010 as well as 16,500 ecstasy tablets and 7,800 cannabis plants. Street prices are 15-25 € for one gram of heroin, 2.5-5 € for one gram of herbal cannabis, 50-75 € for one gram of cocaine and 1.5-2.5 € for one tablet of ecstasy. 2 1. Drug policy: legislation, strategies and economic analysis 1.1 Introduction Bosnia and Herzegovina (BiH) is an independent, sovereign and democratic country located in South East Europe, in the western part of the Balkan Peninsula. According to the 1991 census the population was 4,395,643 but the 2006 estimates place the population at 3,842,762, which is a 16% decrease from 1991. The total land area is 51,209.2 square kilometres. BiH borders with Croatia, Serbia and Montenegro. Bosnia and Herzegovina is a multinational state of Bosniaks, Serbs, Croats and other nationalities. With the breakdown of the former Yugoslavia, in March 1992, BiH became a member of the United Nations and in September of the same year was admitted to the World Health Organization. It became a member of the Council of Europe in April 2002. In accordance with the Dayton Peace Agreement, the war in BiH ended in 1995 and the new administrative structure was established, with two entities: the Federation of Bosnia and Herzegovina (hereinafter Federation or Federation of BiH or FBiH) and the Republic of Srpska (hereinafter RS), and the Brcko District, each with a high degree of autonomy. Today, all components of the health system in BiH (users and their rights, the provision of health care, the organizational structure of the health system, financing and management) are the responsibility of the entities - the FBiH and the RS, ten cantons in FBiH and the Brcko District. Therefore, the health system in BiH actually consists of thirteen "subsystems" that cover the health and social needs of the entire population. 1.2 Legal framework The internal structure of BiH, consisting of the two entities (the FBiH and the RS) and the Brcko District, resulted in a fragmented national legislation. It is therefore necessary to review the current legislation and other regulations for prevention of narcotic drug abuse at the state level of BiH, as well as the entities and the District. The Law on Prevention and Suppression of Abuse of Narcotics in Bosnia-Herzegovina came into force on 15 February 2006. Implementation of this Law involves Ministry of Civil Affairs, Ministry of Security, Ministry of Foreign Trade and Economic Relations, Ministry of Finance and Treasury, Ministry of Foreign Affairs, Agency for Medical Products and Medical Devices of BiH, and police and customs authorities. The Ministry of Security set up a dedicated department to work specifically on the implementation of the Law within its area of responsibility and to monitor the implementation of the Law in other ministries. Adoption of the Law has significantly improved coordination of drug-related law enforcement and demand-reduction measures in BiH. Its adoption has been integrated at state level: specific state-level ministries have been put in charge of its implementation as well as the adoption of a system of measures 3 to be implemented by lower levels of government (in both entities and the Brcko District). The law on drugs, as lex specialis in combating the abuse of drugs, provides for: 1. the establishment of special bodies in charge of combating drug crime and drug use; 2. the classification of plants and substances as narcotics, psychotropic substances, plants from which one may obtain drugs or precursors, according to the regime of bans or controls that are applied against them, and according to their types and characteristics; 3. the purpose and conditions allowed for growing plants from which one may obtain drugs, and the conditions for the production, transport and possession of drugs, psychotropic substances and plants from which one may obtain drugs and precursors; 4. the framework measures for combating drug crime. The Law on Prevention and Suppression of the Abuse of Narcotic Drugs contains a list of narcotic drugs, psychotropic substances and plants that can be used to produce narcotic drugs and precursors, listed in Tables I, II, III and IV. Table I "Prohibited substances and plants"; Table II “Substances and plants under strict control"; Table III "Substances and plants under control "and Table IV "Precursors". The Criminal Code of BiH, Article 195 "Illicit trafficking of narcotic drugs” stipulates the criminalization of certain forms of drug trafficking that have an international character. However, the integrity of the criminal law protection from various forms of abuse was ensured through the introduction of drug offences in the criminal codes of the entities and the Brcko District: - In the Criminal Code of the Federation of BiH: Article 238 - Illicit production and trafficking of narcotic drugs and Article 239 - Possession and enabling the use of narcotics. - In the Criminal Code of the Republic of Srpska: Article 224 - Illicit production and trafficking of narcotic drugs and Article 225 - Enabling the use of narcotics. - In the Criminal Code of Brcko District: Article 232 - Illicit production and trafficking of narcotic drugs and Article 233 Possession and enabling the use of narcotics. Police forces do not tolerate possession of drugs for personal use or possession in small quantities. This causes problems when harm reduction measures, such as provision of needles and syringes, are implemented, as possession of dirty syringes might be considered a misdemeanour in the RS and a crime in the FBiH. In 2010, the Draft Law on Amendments to The Law on Prevention and Suppression of the Abuse of Narcotic Drugs was adopted by the Council of Ministers in July 2011. The adoption of this law by parliament is expected at the end of 2011 or the beginning of 2012. The main changes envisaged in the draft law are: - clear division of responsibilities amongst the bodies involved in supervision of production and trade of narcotic drugs and precursors in BiH; 4 - clarification of procedures for the destruction of seized drugs; - introduction of the requirement for autopsy and toxicological analysis of the post-mortem biological samples in all cases of suspected or obvious drug-related deaths; - creation of a register of drug-related deaths in the Ministry of Civil Affairs; - establishment of the Office for Drugs, a professional multidisciplinary team of experts responsible for the coordination and supervision of all activities envisaged under the National Strategy on Supervision over Narcotic Drugs, Prevention and Suppression of the Abuse of Narcotic Drugs in Bosnia and Herzegovina for the period 2009-2013 and its Action Plan, especially in the field of prevention, medical treatment, rehabilitation and social reintegration, training, statistics and research as well as evaluation of interventions. 1.3 National Action Plan, Strategy, evaluation and coordination 1.3.1 National Strategy, Action Plan and evaluation The Parliamentary Assembly of BiH adopted the National Strategy on Supervision over Narcotic Drugs, Prevention and Suppression of the Abuse of Narcotic Drugs in Bosnia and Herzegovina for the period 2009-2013 (the National drug strategy 2009-2013) in March 2009. This is the first such document at state level, showing the intention of the state to make a systematic effort to engage all stakeholders in the society in tackling drug abuse. The National drug strategy 2009-2013 sets priorities of the fight against drugs, through the general objectives: 1. Raising awareness through community education, in order to implement a healthy lifestyle and maintain mental health, 2. Combating and prevention of further spread of drug abuse, 3. Prevention of drug addiction, death and health damage due to drug abuse, 4. Reduction of damage to the community caused by drug abuse, 5. Reduction of drug demand, especially among young people, 6. Strengthening of institutional capacity and responsible involvement of society, 7. Improving legislation and its implementation, 8. Reducing the supply of narcotic drugs, 9. Formation of an independent multi-sector Office for Drugs – Office for the Prevention of Drug Abuse at the state level (see also the chapter on legislation above). In September 2009 the Council of Ministers adopted the National Action Plan for Combating Drug Abuse in BiH for 2009-2013. The Action Plan is structured in such a way that implementation of strategic objectives defined by the National drug strategy 2009-2013 will ensure effective and coordinated combat 5 against drug abuse in BiH in the medium term (2009-2013). For each of the strategic areas, the Action Plan defines specific objectives, implementation activities, timeframes, stakeholders and progress indicators for the implementation of measures and activities. By the end of 2010, the Commission for the Suppression of the Abuse of Narcotic Drugs (see chapter 1.3.2) prepared an evaluation report on the implementation of the Action Plan which was adopted by the Council of Ministers in May 2011. In this report the commission noted that the Action Plan is not feasible enough in the first year of implementation and made several recommendations to the Council of Ministers: - The Council of Ministers will encourage governments of the entities and the Brcko District to increase the planned level of resources for combating drug abuse in their budgets, - For subsequent evaluation of the Action Plan, a working group for evaluation should be established, - More substantial implementation of the Action Plan in the prison system is required , - Necessary steps should be taken as soon as possible to adopt the Draft Law on Amendments to the Law on Prevention and Suppression of Abuse of Narcotic Drugs, and establish the Office for Drugs at the state level. 1.3.2 Coordination The Law on Prevention and Suppression of Abuse of Narcotic Drugs defines the bodies responsible for coordination of the state drug policy as well as operational bodies directly tackling the drug problem. Responsibility is divided amongst several bodies: - The Commission for the Suppression of the Abuse of Narcotic Drugs (the Commission on Narcotic Drugs) coordinates the activities of the ministries and independent administrative organisations involved in the implementation of the Law, which represents the basis for action by authorities, institutions, associations and other legal and natural persons. The Commission on Narcotic Drugs has been established by the Council of Ministers and the members are: Ministries of Health (Federation of BiH, Republic of Srpska and Brcko District), Deputy Minister of Finance and Treasury, Deputy Minister of Foreign Trade and Economic Relations, Deputy Minister of Security, Deputy Minister of Justice and the Head of Department for Drugs from the Ministry of Security (see also below). It is chaired by the Minister of Civil Affairs. - The Department for the Suppression of the Abuse of Narcotic Drugs at the Ministry of Security (the Department for drugs) is in charge of systematic data gathering and monitoring of the phenomena, collection and processing of data required for prevention and combat against illicit drug trafficking and other criminal offences related to the abuse of narcotics, and for coordination of activities conducted by the police, customs and other bodies in the fight against the abuse of narcotics. It also works on international cooperation projects with the countries of the region and with the representatives of the European Union in the domain of security, and monitors the implementation of the Law on Prevention and Suppression of Abuse of Narcotics. The Department for drugs performs 6 tasks assigned by the Commission on Narcotic Drugs. It also maintains a database on the import and export of narcotic substances, plants from which one may obtain narcotic drugs and precursors and cooperates with operational police forces in this regard. - The Agency for Medical Products and Medical Devices of BiH, pursuant to the Law on Prevention and Suppression of Abuse of Narcotics, is responsible for the authorisation of narcotic and psychotropic substances for legitimate (medical) purposes in BiH. - The Ministry of Trade and Economic Relations is responsible for the control of plants containing narcotic and psychotropic substances. - The Customs and the Border Police are responsible for controlling the import and export of drugs and precursors. The Council of Ministers also established the Commission for the Destruction of Narcotic Drugs, which is supposed to draft the guidelines for storing and destroying seized drugs. The guidelines have not yet been adopted and the commission is not operational at present. The Department for drugs at the Ministry of Security shall perform professional and administrative work for both Commissions. 1.4 Economic analysis The total costs of implementing the drug policy in BiH are not known, however the following paragraphs provide estimates of costs of treatment. The standard tariff for in-patient medical addiction treatment in FBiH is 92 BAM per day, which is approximately 2,800 BAM (i.e. 1,400 €) a month. According to the estimated cost of therapeutic communities, the monthly cost per beneficiary is from 500 BAM to 670 BAM (i.e. 260–340 €). Costs include food, hygiene, medical services, rental space, utilities, office supplies, infrastructure investment and the salaries of employees. As an example, expenses of the biggest and longest established addiction treatment centre in BiH – the Institute for alcoholism and substance abuse in Sarajevo – are given (see more in Chapter Drug–related treatment demand and availability at page 23). Total costs covering in-patient and out-patient treatment of alcoholics and drug addicts except substitution treatment (of them 625 drug users)1 were 2.8 mil. BAM (i.e. 1.4 mil. €) in the Institute in 2010. Budget for substitution treatment (359 patients in substitution reatment) in the Institute in 2010 was 350 thousand BAM (i.e. 180 thousand €). After extrapolation to (patients of) 8 specialised medical addiction treatment centres in BiH, total costs of medical addiction treatment in BiH in 2010 can be estimated as 8.0 mil. BAM (i.e. 4.1 mil. €). 1 It is very approximately estimated that these 625 drug users account for about 70% of total costs. The rest can be attributed to alcohol addiction. 7 Information on the costs of treatment is available from 5 therapeutic communities: Kampus Rakovica – Sarajevo, Centar savremenih incijativa – Izlaz in Ilijas, Victoria in Banja Luka, UG PROI in Kakanj, and Izvor – Kruh Svetog Ante in Plehani. They represent approximately half of the capacity of therapeutic communities for the treatment of addiction (there are 11 communities in total in BiH). In the above mentioned therapeutic communities, the annual costs in 2010 were 3.5 mil. BAM (i.e. 1.8 mil. €). After extrapolation to 11 communities in BiH, the total expenses of therapeutic communities in BiH can be estimated as 7.7 mil. BAM (i.e. 3.9 mil. €). According to the UNDP data on IDU Programs, HIV prevention and care activities among the most-at-risk population are planned for 2011 and include: engagement of peer educators (NGOs PROI, Viktorija, Margina), staff in methadone centres, drop-in centre staff (NGOs PROI, Viktorija, Margina, Poenta), harm reduction , health care provider training, procurement of safety box, procurement of harm reduction kits, condoms, procurement of methadone, IT equipment for centres, methadone storage, facility maintenance and reconstruction, rent for drop-in centres, etc. The total expenditure for the above activities in 2011 is expected to be 1.1 mil. US $ (i.e. 1.5 mil. BAM or 780 thousand €). Costs of liquid methadone (total of 11,498 bottles of 150 ml in concentration 10mg/ml, which is 1,724,700 ml liquid methadone in concentration mg/ml) were 280 thousand BAM (i.e. 140 thousand €) in 2010. According to the Agency for Medical Products and Medical Devices of BiH, the cost of imported Suboxone were 450 thousand BAM (i.e. 231 thousand €) in 2010. According to the figures above, a rough estimate of the total cost of specialised medical addiction treatment, social reintegration in therapeutic communities and harm-reduction would be approximately 18.0 mil. BAM (i.e. 9.2 mil. €) in BiH, annually. 8 2. Drug use in the general population and specific targeted groups 2.1 Introduction Collecting data and information on the causes of drug use, trends in drug use risk behaviours and consequences of drug use should be a regular activity of the relevant professional institutions, given that these activities, within the implementation of strategies for drug control, prevent and combat drug abuse in BiH (Official Gazette BiH 31/09). However, during the recent period no research was conducted with primary focus on the use of narcotic substances in the general population of BiH. The conducted surveys were primarily implemented in the framework of larger research projects whose aim was to investigate a broad set of risk-taking behaviours (drug use, smoking, alcohol, population health status, etc.). The population health surveys were carried out periodically with the aim to follow trends and shape the development of risky behaviour among the population of different age categories. Over the past year (2010) in the RS, a survey was conducted in households, which in its form and methodology relies on EHIS (European Health Interview Survey), and an ESPAD study (European Survey Project on Alcohol and Other Drugs) is currently underway. The above research projects provide a solid basis for gaining insight into the trends of use of psychoactive substances in the general population. From the standpoint of vulnerable groups, the largest number of study projects was aimed at testing the form of sexual risk behaviours among female sex workers (SW) and homosexuals (MSM) as well as injecting drug users (IDUs), but more information on the latter will be given in the chapter on infectious diseases related to drug use. In this chapter we will look at the risk behaviour survey of young people living in institutions for collective accommodation (home for abandoned children, dormitories), i.e. young people deprived of direct parental care, and the assessment of substance use among the general population from research aimed at different age populations (elementary, high school, adult population aged 18 and over). 2.2 Drug use in the general population 2.2.1 Health survey in the Federation of BiH The survey of drug use among the adult population in the Federation has not been done yet. Opportunities are checked to implement questions on drug use according to the EMCDDA standard in the appropriate representative survey among the adult population in the Federation. Questions about drug use will be included in the next planned population health study in line with EMCDDA standards, including questions about the use of the substances in their lifetime (lifetime prevalence), in the last 12 months (last year prevalence) and in the last 30 days (last month prevalence). The next major study of population health on a representative sample in the Federation is planned for 2012–2013, and the substance use questions will be added to the study questionnaire. 9 In 2012, a study on the representative sample of the population aged 15–49 will be undertaken in Federation. A module on use of selected drugs in a lifetime and last 12 months will be included. 2.2.2 Health survey in the RS The Survey on Health Conditions in the RS was conducted in 2010 by the Ministry of Health and Social Welfare and the Institute of Public Health of the RS, dealing particularly with the health needs and the utilization of health services in the RS. The main aims of this household survey were to obtain a general health status rating, to identify leading health problems, health needs, health care utilization and satisfaction with health services. The study included population of RS aged 18 years, with a residence status in country for one year or longer. The sampling unit was the household, and respondents were all household members over 18 years of age who were interviewed separately. The questionnaire module titled Substance Use was included, with questions on drug use and the perceived risks associated with drug use. A preliminary investigation of health conditions, health needs and the use of health care in the RS was conducted during 2002, but due to a low prevalence rate of use of psychoactive substances, this section was not included in the report. Thus there is no possibility to compare the results and to track trends between 2002 and 2010. 2.3 Drug use in the school and youth population 2.3.1 ESPAD study ESPAD (European School Survey Project on Alcohol and Other Drugs) is a European survey on the use of drugs, tobacco and alcohol among the secondary school population, i.e. students of the first year of secondary school (15 years of age). This research is conducted in the whole of Europe, in nearly forty countries. The aim of the above research is to investigate and identify trends and habits of tobacco use and drug and alcohol abuse among secondary school population, and to collect relevant data to enable a comparison of these trends with other European countries, members of the ESPAD project. In 2008, the first European School Survey Project on Alcohol and Other Drugs (ESPAD) was carried out in the Federation of BiH (May–June 2008) and in the RS (November–December 2008) by the Institutes of Public Health in both entities. This was the first time that detailed data on substance use among youth populations was collected and the ESPAD methodology was piloted. In the Federation of BiH, the sample consisted of 2,973 first grade secondary school students (born in 1992 and aged 15 or 16 at the time of the survey) residing in urban areas. Rural schools were not included in the study, which may bias the results. In the RS, a stratified random sampling from the entire territory of RS was performed and the sample consisted of 6,181 first grade secondary school students (see Table 2-1). 10 Table 2-1: Lifetime prevalence of drug use, by gender in the Federation of BiH (FBiH) and the RS (RS), 2008 ESPAD survey (%) Drug Cannabis Opiates (heroin) Volatile substances Cocaine (including crack) Amphetamines Ecstasy LSD Magic mushrooms Sedatives Medicaments together with alcohol Anabolic steroids Injecting drug use FBiH Males Females 20.3 9.6 4.0 2.0 12.4 10.4 4.9 2.5 9.6 4.3 8.5 4.4 4.3 2.6 2.6 1.1 11.6 16.2 5.4 5.2 3.2 0.4 2.7 1.6 Total 14.6 3.0 11.3 3.6 6.8 6.4 3.4 1.8 14.1 5.3 1.7 2.2 RS Males Females 7.2 2.5 n.a. n.a. 3.2 1.7 n.a. n.a. 2.9 0.7 2.7 0.7 n.a. n.a. n.a. n.a. 2.8 5.3 3.9 3.2 n.a. n.a. n.a. n.a. Total 4.9 n.a. 2.5 n.a. 1.8 1.7 n.a. n.a. 4.0 3.6 n.a. n.a. Source: ESPAD Surveys 2008 (Šiljak et al. 2009; Public Health Institute of FBiH, 2008) A further ESPAD study was carried out in the RS in April-May 2011; the spring 2011 study in the Federation failed due to objective technical reasons, but conducting the research in the autumn round (October-November 2011) is considered in agreement with the ESPAD European research centre in CAN, Sweden. The 2011 ESPAD study in the RS included a sample of 3550 secondary school students of the first year of secondary school (aged 15-16 years). The 2011 ESPAD results will be included in the next report. 2.3.2 HBSC study In 2002, the Health Behaviour of School Children (HBSC) survey was conducted among 12-, 13- and 15year-old students in the Federation of BiH and the RS. Time periods are designed to represent the beginning of adolescent age (11 years), the challenge of physical and emotional changes (13 years) and the start of making important decisions about life and career (15 years). In the RS, questions about consumption of other drugs apart from cannabis were added to the standard questionnaire2; in Federation, question on drug use were not included. In the RS, a total of 5,134 students from 37 schools (22 primary and 15 secondary) were surveyed. The study included 2,469 boys and 2,638 girls. However, the drug use prevalence rates were found to be very low — the lifetime prevalence rate of psychoactive medicaments was 9.9%, cannabis was 2.2 %; the lifetime prevalence in opiates, cocaine, ecstasy and amphetamines was below 0.5 %. 2 The questionnaire for primary school contained 55 compulsory questions and the questionnaire for high school students included 90 questions. All questions were grouped into appropriate thematic units, such as demographic data, food and nutrition, physical activity, risky behaviours (tobacco, alcohol, and drugs), violence and injuries and the like. Unfortunately, the questionnaire for elementary school students (11 and 13 years) omitted questions about the consumption of narcotic substances, so the information on consumption of narcotic substances among younger school-age population is not available. 11 2.3.3 The study among youth aged 15–25 in the RS The multi-centric survey among youths in seven countries, regions of former Yugoslavia – BiH (Federation of BiH and RS), Montenegro, Croatia, Kosovo, Macedonia and Serbia – was performed during 2002, with a primary objective to determine the prevailing habits and behaviour of young people in relation to their current situation, their future, education, profession and leisure time. The survey in the RS titled Youth of the RS in the Beginning of the XXI Century had been intended as a data source on youth for preparation of the Action Plan for the Youth at the Beginning of the 21st century. The sample in the RS consisted of 1,422 respondents aged 15 to 25, with a balanced sample structure in terms of sex and age, from 11 municipalities in both urban and rural areas. Stratification was performed by sex and age, respectively. The study used a single questionnaire for all countries that were covered by the survey. Besides the unique part of the questionnaire, each country could add an optional module that was considered relevant. One of the modules of the questionnaire contained a set of questions related to the consumption of psychoactive substances. According to the study, 5.6% of 15-19 year olds and 10.3% of 20-24 year olds had ever used cannabis. About half of those who had ever used had only used once in their lifetime. In terms of exposure to effects of psychoactive substances or acquaintance with their peers who consume psychoactive substances, an equal number of young people under the age of 19 (38.7%) and over 19 years of age (36.2%) know peers who consume drugs. Moreover, two questionnaire studies were carried out in 2001 and 2006 among university students (18– 25 years of age) and showed a lifetime prevalence of the use of illicit drugs (cannabis, ecstasy, inhalants, LSD, cocaine) of 22.5 % in 2001, and 31 % in 2006. 2.4 Drug use among targeted groups 2.4.1 Drug use among children without parental care In 2008, UNICEF in BiH coordinated and the entity Institutes for Public Health implemented a study on risk behaviour of children in institutions with collective accommodation. The aim of this study was to investigate and establish the prevalence of different forms of risky behaviour (use of tobacco, alcohol and drugs, and risky sexual behaviour) among this vulnerable group3. The study included 392 children and adolescents (209 boys and 183 girls) aged between 12 and 20 (most frequently 15–17 year olds) living in institutions or with foster parents. Some 5 % of respondents reported using cannabis in their life, while 0.5 % had used amphetamines. Prevalence rates were higher for males and children living in institutions as compared with those living with foster parents. About two-thirds of those who had tried cannabis had 3 The study applied specially designed instruments for boys and girls, which differ in the set of questions about sexual habits. When designing the questionnaire, following factors were taken into account: UNGASS indicators for monitoring the implementation of the Declaration of Commitment on HIV/AIDS, and the indicators recommended by the regional office of UNICEF-II, London School of Hygiene and Tropical Medicine and related follow-up of adolescents in risk of infection (MARA). 12 done so for the first time at the age of 15–16 years. The results showed that cannabis was readily available: 72 % of respondents noted that it could be easily purchased on the street or in the park, 61 % at school, 56 % in clubs and bars and 22 % from dealers at their homes (UNICEF, 2008). Respondents stressed that they can easily obtain cannabis or glue (containing volatile substances to inhale), while other narcotic substances were not so easily available. 13 3. Prevention 3.1 Introduction Prevention of high risk behaviour and use of addictive substances in BiH has been introduced into the National drug strategy 2009-2013. A precautionary approach should be used, with measures and activities to be implemented through various systems: health and social care system, education system, judicial system, media, etc. Special needs of ethnic minorities should be taken into account with respect to possible language barriers and problems with access to health and social services. So far, prevention programs in schools in the RS have occurred through individual classroom lessons where teachers in primary school education spoke about the negative effects of psychoactive solute, which was not enough. In addition, prevention programs have been developed through various projects carried out by non-governmental organizations (youth) and a particular role in preventive activities was played by the association of citizens - Victoria (NGO), which usually focuses on the important tasks of a program of preventive activities related to substance abuse. Also, the present reform in mental health, with the opening of a large number of mental health institutions/centres in both entities, opened up great opportunities for preventive work in this area. 3.2 Universal prevention In BiH, school prevention programmes are formulated and instigated by Ministries of Education and Health at the entity level, at the cantonal level in the Federation of BiH, and at the local level in municipalities. The educational system has enormous possibilities to make a positive impact on children and youth in the process of growing up and forming attitudes, knowledge acquisition and implementation of best practices related to issues of drug abuse. The problem of reducing drug demand through the education system focuses on the prevention of use, especially among the young population. There is no standardised prevention programme being implemented in school curricula or embedded in the school system at the state level in BiH but there are a number of prevention programmes implemented at regional and local levels. Non-governmental organisations (NGOs) are also involved in the implementation of prevention programmes in elementary and secondary schools and also in extracurricular activities (peer programmes, workshops). In Banja Luka (RS), the NGO Victoria has implemented a number of prevention activities in recent years: - In 2003, NGO Victoria organized preventive activities titled Stop Drugs. Made prevention lectures for parents and students in primary schools and secondary schools. These preventive activities included over 2000 primary and secondary schools. - In the period from December 2006 to January 2007, NGO Victoria prepared a project Drugs Yuck, which was funded by the city of Banja Luka and the project was carried out to educate the educators in 11 secondary schools to advise students about drug abuse and its risks. 14 - Between December 2007 and March 2008, NGO Victoria implemented the project of prevention It Is Not Worth Living funded by the city of Banja Luka and worked on educational lectures about drug abuse and its consequences for primary schools in the city of Banja Luka, through showing of a documentary film and distribution of printed educational materials. - In the period from September 2008 to December 2009, the project We are Stronger Together was funded by the city of Banja Luka and implemented by the NGO Victoria. The main goal was education and awareness of high school students about the dangers and risks of drug use as well as reduction of prejudice and misconceptions about this issue. Activities were carried out as workshops with high school student councils, bringing a group of high schools together in preparation and performance of theatre plays and also included the preparation, printing and distribution of educational materials. The Programme for Prevention of Addictions of the Sarajevo Canton is a good example of coordinated preventive activities supported jointly by the Ministry of Health and the Government of the Sarajevo Canton and implemented by a multidisciplinary professional team — the Council for the implementation of the programme. This programme has been running since 1999 and its latest revision was adopted for 2008–2010. The Mental Health Centre Banja Luka (RS) became another important factor in prevention activities in primary schools related to risky behaviour of addicts in the area of Banja Luka. 3.3 Selective and indicated prevention in at-risks groups and individuals 3.3.1 Prevention within the health system It is important to emphasize the importance of early detection of symptoms and behavioural disorders caused by use of psychoactive substances, but not yet clinically visible. In this regard, in addition to education, it is necessary to achieve good cooperation between all institutions and have a connection with young people. Family medicine has a special role in motivating, counselling, early detection of risks and ongoing support. All services in the health sector should be open and friendly for users of psychoactive substances and records should be kept by the agreed indicators. In this field, the preventive activities were also carried out by the NGO Victoria, which implemented the project "Person" funded by CIDA LIP (Canadian organization) in the period from April 2007 to March 2008. Project partners and members of the working group were the Banja Luka Medical Centre and the Association of Family Doctors of the RS (organized education for family medicine teams), based in Banja Luka. The topics concerned drug abuse, HIV, AIDS and other sexually transmitted and blood borne infections. Lectures were given by specialists in the field of substance abuse and the National HIV Coordinator. In the period from September to December 2008, NGO Victoria implemented a project titled Support to the Capacity Building on HIV / AIDS and Programming for MARA in BiH, which was funded by the UNICEF 15 in BiH. The program was designed for HIV stakeholders, NGOs involved in the prevention of HIV, medical workers and relevant institutions and individuals in this field. Basic goals of this project were: design of programs for preventive work with adolescents at high risk of HIV infection (MARA) and persons living with HIV, development of manuals of good practice for VTC staff, and development of a plan to combat stigma and discrimination associated with HIV. 3.3.2 Prevention within the social protection system In the social protection system, the municipal social welfare centres play an important role and they carry out the actions defined by prevention programs, with focus on identified vulnerable groups and individuals with certain risk factors. Particular emphasis and attention should be given to children without parents, pupils and students residing in dormitories, student homes, individuals who live in shelter homes and adoptive/foster families, with noted social needs and additional risk factors. A project titled Improving HIV / AIDS Prevention and Improving the Social Environment for Adolescents Living in Collective Centres in BiH was started in August 2009 and is still ongoing under the sponsorship of UNICEF BIH. In cooperation with the NGO Victoria, the project aims to improve the skills and knowledge of adolescents in children’s homes towards adopting a healthy lifestyle and enhancing the environment where they live. The project will also seek to strengthen the access of adolescents to health services for young people. Project activities include: educational workshops for youth, training for staff working in the collective homes, discussions in primary schools attended by children from the homes, local round tables with municipal bodies, social services centres, school management, pedagogical institutes and the like. 3.4 National and local media campaigns The Programme for Prevention of Addictions of the Sarajevo Canton is in operation since 1999. The emphasis is placed on health promotion as well as public and targeted education. Parts of promotional activities were the media campaigns carried out by the Ministry of Health of the Sarajevo Canton: - 2001-2002: Public campaign "Drugs Kill Dreams", - 2002-2003: Public campaign "What's Your Anti-drug", - 2002: Public campaign "Do Not Let Drugs Control Your Life”. Under the Action Plan for implementation of measures from the Baseline Road Traffic Safety Strategy in the Federation for 2008-2013, the Federal Ministry of Internal Affairs in Sarajevo organized a round table discussion in 2010 on the topic of Drugs as a Cause of Traffic Accidents, and an international conference titled Prevention and System Safety in Road Traffic in BiH with a presentation of the analysis of road traffic safety situation in BiH in 2002–2009. As a result of these activities, the “Love Life, Respect the Rules” public campaign took place in Sarajevo, with screening of drivers in terms of respect for traffic rules (speeding, use of seat belts, etc.) and detection of persons driving under the influence of alcohol or drugs. A large number of activities related to primary prevention of alcohol and drug abuse at the local community level has been accomplished in many cities of BiH (Zenica, Doboj, Gorazde, Tuzla, Banja Luka and others) in the post-war period. 16 3.5 Evaluation of prevention activities Within the evaluation of the implementation of the National Action Plan against Drug Abuse in BiH in 2009-2013, the following conclusions were made regarding the prevention of drug use: - Regarding prevention in schools, activities have been partially implemented. Very little was done regarding work in pre-schools, encouraging peer education and strengthening the role of family medicine. There are partially implemented education programs for teachers and pedagogical workers. - Certain projects were carried out, for example in the RS the Training Program for Prevention of Drug Abuse in Schools was implemented by the Ministry of Internal Affairs and the Ministry of Education and Culture of the RS. - Certain activities have been conducted by institutions in the Cantons of Sarajevo, Zenica-Doboj and Tuzla. - It is acknowledged that more needs to be done in the field of preventing violence such as educating parents. However, some improvement in this field can be seen in the Cantons of Sarajevo, ZenicaDoboj and Tuzla. - As a part of preventive healthcare, a few activities were carried out in relation to healthy lifestyle education and the education of pharmacy staff. Institutions that have implemented certain actions are as follows: entity ministries of health, Public Health Institute of the Federation of BiH, the Ministry of Family, Youth and Sports of the RS, the Cantonal Institute for Substance Abuse Zenica, Sarajevo Canton. - Just a small part of the activities have been carried out within local communities. Certain activities were conducted by the entity ministries of health, ministries of interior, Ministry of Family, Youth and Sports of the RS, the Ministry of Education and Culture, institutions in the Canton of Sarajevo, ZenicaDoboj and Tuzla Canton. The work of NGOs was financially supported. - Regarding prevention in the field of social protection, some activities were implemented by the following institutions: Ministry of Health and Social Welfare of the RS, institutions in the Cantons of Sarajevo, Zenica-Doboj and Tuzla. - Activities related to prevention in prisons have been implemented within the framework of education projects dealing with training of prison staff, education of prisoners about HIV prevention, other blood transmitted infections and improvement of the health of prisoners. 17 4. Problem drug use 4.1 Introduction In the early nineties there were approximately 1,500 registered drug users in BiH and according to experts the assumption was that the total number of users, including unregistered users, was three times higher. Expert estimates suggest the number of injecting drug users in BiH in 2009 ranged from 3,000 to 8,0004, out of which 2,000–3,000 in the Federation of BiH and the Brcko District, and 2,000 to 3,500 in the RS. NGO experts believe that there could be up to 15,000 injecting drug users5. To date, the number of problem drug users is evaluated using standard methods. 4.2 Prevalence estimates of problem drug use In 2009, a second sero-behavioural study among injecting drug users (IDUs) was conducted by UNICEF in three major cities of BiH (Sarajevo, Banja Luka and Zenica). First such study was conducted two years earlier. In 2007, the number of sampled IDUs was 780 and 781 IDUs were sampled in 2009 (UNICEF BiH, 2007). The aim of the studies was to determine the prevalence of HIV and viral hepatitis among IDUs and to monitor behavioural risk factors related to drug injecting. IDU population size estimates in the abovementioned cities were also performed within the 2009 study, using a multiplier method (UNICEF BiH, 2010). The estimated number of IDUs in Sarajevo was 889 (95 % CI: 703–1,075), in Banja Luka 534 (95 % CI: 354– 717) and in Zenica 852 (95 % CI: 809–895). These results were extrapolated to entity and state levels and thus, in 2009, the estimated population of IDUs in the Federation of BiH is 4,900 persons, and in all BiH (i.e. including both entities — the Federation of BiH and the RS), amounts to 7,500 persons (UNICEF BiH, 2010), which is 2,7 persons per 1000 population aged 15–64. 4.3 Data on problem drug users from non-treatment sources 4.3.1 Sero-behavioural studies among IDUs There were two studies performed by UNICEF among IDUs in 2007 and 2009. In 2009, the sample of the sero-behavioural study consisted of 261 IDUs from Sarajevo, 260 from Banja Luka and 260 from Zenica (UNICEF BiH, 2010). The respondents were selected using respondent-driven sampling. Data was collected from October to December 2009. The standard questionnaire had 142 questions and it was administered during face-to-face interviews. The average age of respondents was 29–30 years, men made up to 90 % of the sample in all three cities. A majority of respondents had completed secondary education, had part-time employment or were financially supported by their families. The average age of first drug injection was 21–22 years among the sampled IDUs; the majority had been in contact with the police. Thus, 49 % of respondents in Sarajevo, 43 % in Zenica and 39 % in 4 The Global Fund to Fight AIDS, Tuberculosis and Malaria (GF) consensus workshop, Sarajevo, May 2009 (consensus between NGOs and governmental organisations). 5 NGO Margina during EMCDDA/CARDS assessment mission, May 2008 18 Banja Luka had been arrested or detained during the last year. Around one fifth of respondents in Banja Luka and about half in Zenica and Sarajevo were in prison at one point in their lives. According to the 2007 UNICEF survey in Sarajevo, Banja Luka and Zenica, among a sample of 780 injecting drug users (260 in each city), approximately 95 % of IDUs injected heroin in the last month. The majority of them were aged 25–34, and men formed 90 % of the sample. Approximately 80 % of the sample was unemployed. About one half of IDUs reported that they had been arrested by the police during the last year, although the proportion was almost 70 % in Sarajevo. In 2009 study, it was estimated that 70% of injection drug users in Sarajevo were treated for drug addiction at some point in their lives, 50% in Banja Luka and 48% in Zenica. Of the total percentage of those who have ever been treated for drug addiction approximately 28% in Banja Luka and 63% in Zenica is currently undergoing treatment. In Sarajevo (97%) and Zenica (79%) majority of those being treated are exposed to methadone treatment, while in Banja Luka, most of them (47%) are trying to self-treat their addiction. 70% in all three cities reported that their first drug injection was injected by another person, and in most cases the person was a friend. The reasons most often given for the start of injection drug use were curiosity and desire to achieve the same or better effect with less or the same amount of drugs. More than 90% in Sarajevo and Banja Luka and 80% in Zenica personally knows other injection drug users and has watched as an addict injected himself with drugs before they themselves began to use injection drugs. Findings from in-depth interviews suggest that injection drug users have limited access to health services. Fear of identification as injection drug users, unprofessional attitude of medical staff and the involvement of the police are often cited as reasons to avoid calling for help in emergency situations such as an overdose. Sharing injecting equipment appears to be common, especially between sexual partners. The reasons for this adverse behaviour are usually required beyond personal responsibility. Sometimes they are justified by reasons such as lack of pharmacies in the vicinity of their residence. The women stated that they are married or in a relationship directly or indirectly, are economically dependent on their parents or parents' partners, and most are unemployed. Social contacts were limited and they usually live with the family and partner. Almost all, except one, in conjunction with partners who have or have previously had problems related to drug addiction. Injection equipment is usually bought in pharmacies or acquired for free from local NGOs. Four out of 15 respondents stated that they were providing sexual services in exchange for money or drugs. The provision of sexual services by injection drug users is not uncommon and this is usually with dealers and customers. Most women had been subjected to some kind of treatment aimed at cessation of drug addiction. The surveyed injection drug users reported that they have encountered pharmacists with a lot of prejudice when they wanted to buy equipment for the injection, and similar behaviours of medical staff. The pharmacies sometimes refused to sell the equipment under the pretext that they need a new shipment. They also noted traumatic experiences from psychological or physical abuse by police. A third of respondents in the qualitative component of the survey said that they are infected with HCV. 19 Awareness of risk reduction services, particularly through NGOs Victoria and PROI, is high and survey participants reported that staff in these organizations helps to maintain a pleasant professional atmosphere. There were significant differences in key indicators between surveys conducted in 2007 and in 2009. Survey in 2009 showed a higher proportion of injection drug users who were aware of the organizations involved in preventing the spread of HIV in their cities, a higher number of injection drug users who used sterile equipment for injection and, judging by the responses, a smaller number of those who shared needles and/or syringes. The ratio of those who reported non-governmental organizations as the main source of injection equipment has increased significantly in the last two years. 4.3.2 The survey among men having sex with men and sex workers Research in risk behaviour among populations at increased risk of HIV/STIs has been conducted in the period from January to February 2008 on the sample of 224 respondents from the sub-population of men who have sex with men (MSM) and a sample of 146 respondents from the sub-population of sex workers (SW) in seven urban areas in BiH: Sarajevo, Banja Luka, Mostar, Tuzla, Prijedor, Bijeljina, and Prnjavor (Ravlija et al. 2008). Field work was done by public health and infectious disease clinics in collaboration with NGOs: NGOs Margina from Zenica, Action Against AIDS (AAA) from Banja Luka, Association for Sexual and Reproductive Health - XY and PROI from Sarajevo. The purpose of this study was to sample populations with especially risky behaviours, estimate the prevalence of HIV/STIs, distribution of risk and protective sexual behaviour, which would allow the establishment of base data and planning of targeted prevention programs. Among others, drug use was one of the risk factors surveyed. Drug use in their lifetime was reported by 102 respondents (46%) (FBiH 42%, RS 60%) of which 15 reported drug injecting (all of them were from RS, of which eight reported sharing equipment for injecting drugs). From a total of 92 MSM, 46.7% reported experience with drug use, of which 4 / 42 by injection, of them 2 respondents shared equipment used for injection. As for interaction between sexual behaviour and alcohol and drug use, 22% MSM mentioned sexual intercourse under the influence of drugs in the past six months, however the sexual intercourse under the influence of alcohol was more frequent (56.1%). As far as results among sex workers (SW) are concerned, mean age of subjects was 28 years (19–51), 88.4% was urban population. First sexual services in exchange for money were provided between 17 and 26 years by the majority of respondents (74.4%). Almost half of respondents (47.2%) were exposed to some form of abuse, most of it psychological (42.8%) followed by physical (34.5%), and a significant proportion was exposed to rape (12.4%) and trafficking in women (6.9%) as very severe forms of abuse. Users of sexual services are mostly men of all ages, mostly urban residents (86.9%), then foreigners in the city and travellers in transit. 20 Total of 45 (32.1%) SWs have confirmed that they once used some illegal drug. Of total respondents who ever used drugs, 28.8% injected them – see Figure 4-1. Of those who used drug in injection, over half (53.8%) had once been injected with used needles and syringes. Figure 4-1: Injecting drug use among sex workers in their lifetime in BiH (%) RS 20 FBiH 80 33,3 BiH 66,7 28,8 0% 10% 71,2 20% 30% 40% 50% Yes 60% 70% 80% 90% 100% No Source: Ravlija et al. 2008 Only 15.9% of SWs known that they have had sexual relations with clients who are injection drug users, while 60.7% respondents did not know whether they had such partners. Less than one quarter (23.4%) SWs considered to have provided services to this subpopulation. Nearly a third of respondents (29.6%) had sexual intercourse under the influence of drugs, and 89.7% under the influence of alcohol (see Figure 4-2). 45 (32.1%) respondents have confirmed that they experienced unacceptable and risky sexual behaviour under the influence of drugs. Figure 4-2: Sexual intercourse under influence of drugs and alcohol among sex workers in their lifetime in BiH (%) No answer 5,5 No 4,8 17,6 52,8 Yes 89,7 29,6 0 10 20 30 40 50 Illegal drug 60 70 80 90 100 Alcohol Source: Ravlija et al. 2008 Survey results are available specifically for respondents aged 18-24 years. From a total of 39 young women aged 18-24, 15 (38.5%) used drugs at least once in their lifetime, and only one of them (5.9%) injected the drug, which is less than in the total sample (28.8%). 17.5% of young women had sexual relationships with clients who are injection drug users , more in the FBiH (29.4%) than in the RS (8.7%). A 21 third (33.3%) had sexual intercourse under the influence of drugs, while 89.7% under the influence of alcohol, which is consistent with the basic pattern. 4.4 Other intensive, frequent, long-term and problematic forms of drug use No information available. 22 5. Drug–related treatment demand and availability 5.1 Introduction Drug treatment services in BiH are present, with limited variety and coverage. The public services, such as drug-free medical treatment or counselling, vary in terms of types of services available and their coverage differs from one region, canton or city to another. Similarly, substitution maintenance treatment has been implemented with various coverage and capacity depending on the policy and coordination at the level of the entity, canton, and city, though consistency exists in terms of criteria and rules. Initiatives towards implementation of compulsory treatment in psychiatric health care system and recently in primary health care institutions have been recently launched. Services provided by NGOs are an intensively growing sector of drug services, particularly harm reduction and social rehabilitation services (therapeutic communities). They were funded by the Global Fund and commissioned by UNDP/UNICEF and are advanced in terms of networking and data collection (even if only in terms of their performance for project purposes). Some NGOs have made a step forward and started cooperation with the prison system. Up to 2008, the official system of statistical reports on healthcare was adopted from the former Yugoslav system and is still based on the Yugoslav standards. In some cantons, the data was collected according to standard and form of EMCDAA / Pompidou Group of the Council of Europe. In practice this means that the Institutes of Public Health collected information from treatment institutions, but this system was not operational in the entire territory. In February 2010, a Protocol on Cooperation for the Implementation of the Law on the Prevention and Combat of the Abuse of Narcotics — The Evidence of Drug Addicts and Abusers was adopted in BiH, which provides the conditions for data collection on clients in drug treatment according to EMCDDA standards. 5.2 Treatment strategy and policy The role of the Ministry of Civil Affairs (its Department of Health) is to prepare and to implement regulations in the social and health sector at state level, to carry out the tasks and duties which are under the jurisdiction of BiH, and to determine the basic principles of coordination of activities and harmonizing the plans of entity authorities. It coordinates activities between the entity ministries of health and the Department of Health of the Brcko District. In order to achieve this goal, the Ministerial Conference has been established as the highest advisory body in the health sector in BiH consisted of Minister of Civil Affairs and ministers of health of entities and Brcko District. The Conference appointed a working group with representatives from the entities and the Ministry of Civil Affairs, which are in charge of specific areas. 23 5.3 Treatment system 5.3.1 Medical treatment In the post-war period, the Ministries of Health in the Federation of BiH, RS and the Brcko District, with the assistance of the World Health Organization (WHO), the World Bank, Swedish SIDA and Holland Health Net International, reformed the mental health system through de-institutionalisation of the existing — at that time — mental health system and its re-orientation towards the community psychiatry. There are 40 community mental health centres (MHCs) in 10 cantons in the Federation of BiH, 18 MHCs in the RS, and one in the Brcko District. They provide outpatient treatment and counselling for drug users, though drug users are not their only target group. The number of cases related to the use of drugs which are treated in institutions for mental health is not known, although there are indications that, for example, 200 users, according to experts, are treated in the RS on annual basis, and that about 150 new injecting drug users are registered in the Federation of BiH. Some major mental health centres (e.g. in Sarajevo and Banja Luka) publish their statistics. According to the indicative data, approximately 85% of all users in treatment are heroin users (mostly injecting users), 90% were men, and the average age is 25. There are 8 specialised addiction reatment centers in BiH, 5 of them in FBiH (Sarajevo, Zenica, Mostar, Sanski Most, Odzak), 2 centers in the RS (Banja Luka and Doboj), and 1 in Brcko District. Treatment program for addiction is a complex multi-component process that takes place in phases and is implemented in a multidisciplinary manner. The program contains the following components: development of motivation, pharmacological therapy, individual psychotherapy, family counselling and occupational therapy, group social therapy with emphasis on the cognitive behavioural therapy, therapeutic communities, and various support groups in the community. Experts estimate that the drug treatment is sought only by 20% of all addicts in a country. 6 In areas without specialized drug treatment centres, drug users can receive some support from community mental health centres as well as from the family doctors. Drug treatment has not been implemented in the prison setting so far, but there are plans to implement drug treatment in prisons within the current national drug strategy.7 6 Although according to the results gained within UNICEF’s sero-behavioural study in 2009, an estimated 70 % of the IDU population in Sarajevo, 50 % in Banja Luka and 48 % in Zenica has undergone drug treatment in their lifetime. Out of those who have ever been treated, 28 % in Banja Luka and 63 % in Zenica are currently in treatment. In Sarajevo and Zenica, a large majority (97 % and 79 %, respectively) of those who are currently treated are undergoing MMT, while in Banja Luka 47 % are trying to treat addiction on their own. The survey also found that access to and utilisation of healthcare services by female IDUs is limited. 7 However, special cooperation between drug treatment centres and penitentiaries was achieved and perpetrators in the investigation procedure, who were included in the methadone maintenance program at the time of arrest, can use methadone during the investigation, or undergo methadone detoxification if the perpetrator receives a punitive measure. 24 5.3.1.1 Substitution treatment Methadone treatment was introduced for the first time in Sarajevo in 1989 with 50 opioid addicts in the programme. This program was stopped by the war in BiH and re-established in Sarajevo in 2002. Nowadays, seven centres in seven cities provide methadone detoxification and maintenance treatment in BiH: four in the Federation of BiH (Sarajevo, Zenica, Mostar, Sanski Most), two in the RS (Banja Luka and Doboj) and one in the Brcko District. In 2009, maintenance treatment with buprenorphine (Suboxone) started in Tuzla (the Federation of BiH), and in 2010, it started in Sarajevo (7 patients currently in treatment). The MMT programmes in Sarajevo, Zenica, and Doboj use the liquid form of methadone. In other cantons of the Federation of BiH (Mostar and Sanski Most), tablets are prescribed which increases the risk of misuse and diversion into the black market. The MMT centre in Banja Luka also uses liquid methadone. Methadone tablets are available on prescription in (some) pharmacies in some cities of the RS. The average dose of methadone in the Sarajevo centre is 50.5 mg/day, in Banja Luka, 70 mg/day. In the Sarajevo Canton, the criteria for the provision of MMT are stipulated in the Cantonal Addiction Prevention Programme (other cantons have no officially defined criteria). Criteria for inclusion are that clients must: be over 18; have used opiates for more than two years; exhibit symptoms of addiction according to ICD-10; and have been treated at least twice at hospital-based institutions previously. The programme foresees that the treatment can be provided only through certified health institutions. The same inclusion criteria are used in the MMT in Banja Luka. Four forms of methadone treatment, as recommended by the WHO, are performed in BiH: - Short-term detoxification – reducing doses of methadone within a month or less. - Long-term detoxification – reducing doses of methadone in a period longer than a month. - Short-term continuation – stable prescription of methadone for a period of 6 months or less. - Long-term continuation – stable prescription of methadone for a period longer than 6 months. Decision on the type of treatment should be made on the needs of individual patients and the options available at the centre. A methadone detoxification programme is implemented in inpatient wards in Sarajevo, Zenica and Banja Luka. Methadone detoxification programmes in the Federation of BiH have a total capacity of 21 beds. 5.3.2 Social rehabilitation Rehabilitation programs for drug users are conducted for the period of 1-3 years in a therapeutic community based on occupational therapy with the final aim of social reintegration. There are 11 therapeutic communities in BiH, some operated by religious communities, others by NGOs and one governmental (Campus Rakovica — Sarajevo). Three therapeutic communities (in Aleksandrovac — Banja Luka, in Banja Luka, and in Majcino selo — Medjugorje) accept female users. 25 Two big medical drug treatment centres in Sarajevo and Banja Luka Public Institute for Alcoholism and Substance Abuse of Canton Sarajevo In Sarajevo, existing since 1977, the Public Institute for Alcoholism and Substance Abuse of Canton Sarajevo is a specialised institution for prevention, treatment and rehabilitation of disorders related to drug use and addiction. The Institute has two departments — one for alcoholism and another for drug addiction. The department for drug addiction has an inpatient detoxification unit with 10 beds and an outpatient unit for the MMT programme. The Institute also has two counselling units. The total number of visits (to any form of treatment offered by the Institute) during 2010 was 136,116 which is 12.5% more than during 2009 (119,110 visits). In 2009, the Institute for Alcoholism and Substance Abuse in Sarajevo Canton registered 118 first-time diagnosed drug users, which is a 20 % increase when compared with 2008. In 2009, approximately 9,303 visits were registered in both the counselling centre and the outpatient unit. In 2010, 73 persons were registered as newly diagnosed drug users, while the number of visits to both units was 8,839. The majority of clients (90 %) are male, with primary use of cannabis, followed by heroin and psycho-stimulants; 70–80 % of them are IDUs. In 2009, the MMT programme of the Institute had 349 clients (60 % more than in 2008), and the same number of clients was recorded in MMT in 2010 (of which 26 were female). In addition, 138 and 126 clients participated in a detoxification programme with methadone in 2009 and in 2010, respectively. In 2010, the majority of MMT clients were male (92 %) with the mean age of 33.5 ± 5.9 years (age range 23–50 years). The mean age of first drug use for the clients was 17.8 ± 2.3 years; for heroin use it was 20.7 ± 2.5 years. The majority of addicts contacted the Institute for the first time at the age range 22–25 years. The methadone detoxification program in 2009 included 138 patients and 126 patients during 2010. In addition to the above addiction treatment interventions, approximately 15,000 counselling sessions were administered in the Institute in 2010, which is a 42.3 % increase in comparison with 2009, when 8,752 such interventions were administered. The counselling is mainly administered to persons in experimentation or in the early stage of drug addiction and these persons constitute the main target group of the Programme for Prevention of Addictions in Canton Sarajevo. Psychiatric Clinic of the Clinical Centre in Banja Luka In July 2009, the Detoxification and Methadone Centre in the Psychiatric Clinic of the Clinical Centre in Banja Luka was officially opened. Service beneficiaries are mainly from the territory of Banja Luka and also from Prijedor, Novi Grad, Pale, Trebinje and other surrounding towns and villages. Since the opening of the MMT programme in July 2009 until February 2011, 97 clients have been treated. From July 2009–February 2011, 103 drug users were treated in the detoxification centre; 73 patients in this period came for the first time in their life. The majority were in the 21–30 age group although some clients were older. All clients were heroin/opiate users and 95 % of them injected drugs. 5.4 Trends and characteristics of treated clients In February 2010, the Ministry of Civil Affairs of BiH, the Federal Ministry of Health of BiH, the Ministry of Health and Social Welfare of the RS, and the Department of Health and other services of the Brcko District signed a Protocol on Cooperation for the implementation of the Law on the Prevention and Suppression of the Abuse of Narcotics — The Evidence of Drug Addicts and Abusers (hereinafter: Drug Treatment 26 Register).8 The Protocol defines mutual rights and obligations of the participants to collect, report and share information. A unique drug treatment demand registration form in line with EMCDDA standards was published in the Official Gazette No. 73/09. This form is mandatory for all legal bodies (state, NGO, private) that provide detoxification, drug treatment, rehabilitation, religion-based rehabilitation and other forms of drug treatment. The Ministry of Civil Affairs, together with the Institute of Public Health of the Federation of BiH, the Institute of Public Health of the RS and the Department of Health and other services in the Brcko District, coordinates this information system. Data collection started in November 2010. 5.4.1 Clients in medical addiction treatment centres Data according to the Drug Treatment Register form was collected in spring 2011 retrospectively for 2009 and 2010 patients from 8 specialised centres for addiction treatment9. In 2009, the total number of all requests for treatment was 1,455, and 1,544 in 2010. The number of firsttime applicants for treatment in 2009 amounted to 364, while 326 cases were reported in 2010, as new cases treated for the first time in their life (FTD). From the total number of patients 92% were men and the average age of beneficiaries was from 28 to 29 in 2010 (see Table 5-1 and Figure 5-1 to Figure 5-3). Primary psychoactive substances were predominantly opiates (heroin and morphine) followed by cannabis; other reported substances were misused medical drugs (benzodiazepines, tramadol), ecstasy, and cocaine. The total number of patients in substitution treatment during 2009 amounted to 1,151 clients (in 2009 predominantly on methadone), while the number in 2010 was 1,183 clients, majority of them on methadone. The largest majority of patients were in age groups older than 25 (see Table 5-2). Number of clients in substitution treatment in 2009–2010 by centres is provided in Table 5-3.10 8 According to the Protocol of the Drug Treatment Register, statistical data is submitted to the institutions for the protection of public health in BiH, entity ministries responsible for health or the responsible authority of District and the Ministry of civil affairs, at the end of each quarter of the calendar year; and the Commission on Narcotic Drugs and the Department for Drugs of the Ministry of Security whenever necessary, and at least twice a year. The responsible institutions listed in the Law for Prevention and Suppression of Illicit Drugs, Article 76, paragraph 1, as well as the institutions in charge of public health are: cantonal/regional public health institutes, Department of Public Health of the Federation, Institute of Public Health of the Republic of Srpska and the Ministry of Civil Affairs of Bosnia and Herzegovina. Entity ministries appointed the persons responsible for the TDI register (two people from the Public Health Institute and the Institute of Public Health of Federation, and one representative from the Ministry of Civil Affairs), that constitute a working group for statistical data from the TDI register. This working group, after the establishment of systems in both entities, will provide data to the bodies and institutions mentioned in the protocol. 9 Data was collected from the Institute for Alcoholism and Substance Abuse in Canton Sarajevo, the Cantonal Institute for the Prevention of Drug Addiction in Zenica, Centre for Outpatient Treatment of Addiction in Mostar, Clinical Center in Banja Luka, Association for Prevention and Treatment of Drug Abuse Nova Nada (New Hope) in Sanski Most, Clinical Center in Tuzla, Center for Mental Health in Doboj and the Health Center in Odzak. 10 In 2008, there were 680 heroin users in MMT in Bosnia and Herzegovina: 250 in Sarajevo, 200 in Zenica, 170 in Mostar, 36 in Sanski Most and 28 in Doboj. Majority were in the 24–30 age group, and 80–90 % were males. 27 Table 5-1: Number and average age of treated clients in 8 drug treatment centres Indicator Number of all requests for treatment (ATD) Number of first-time requests for treatment (FTD) Average age of ATD patients Average age of FTD patients 2009 1,455 375 32.1 27.0 2010 1,544 324 29.8 28.2 Source: The Evidence of Drug Addicts and Abusers in BiH (Ministry of civil affairs BiH, 2011) Figure 5-1: All treatment demands in 8 treatment centres 700 600 500 400 300 200 100 0 Dom zdravlja Odzak Zavod za Klinicki centar alkoholizamBanja Luka Sarajevo Doboj Zenica ATD 2009 26 327 7 541 ATD 2010 14 344 17 625 Tuzla Sanski Most Mostar 118 114 41 281 101 134 37 272 Source: The Evidence of Drug Addicts and Abusers in BiH (Ministry of civil affairs BiH, 2011) Figure 5-2: First treatment demands in 8 treatment centres 140 120 100 80 60 40 20 0 Dom zdravlja Zavod za Klinicki Odzak alkoholizam- centar Banja Doboj Zenica FTD 2009 18 54 7 118 FTD 2010 11 60 11 73 Tuzla Sanski Most Mostar 13 96 8 61 10 114 8 37 Source: The Evidence of Drug Addicts and Abusers in BiH (Ministry of civil affairs BiH, 2011) 28 Figure 5-3: Percentage of first treatment demands in all treatment demands by 8 treatment centres 100.0 90.0 80.0 70.0 60.0 50.0 40.0 30.0 20.0 10.0 0.0 Zavod za Dom zdravlja Klinicki centar alkoholizamOdzak Banja Luka Sarajevo Doboj Zenica %FTD 2009 69.2 16.5 100.0 21.8 %FTD 2010 78.6 17.4 64.7 11.7 Tuzla Sanski Most Mostar 11.0 84.2 19.5 21.7 9.9 85.1 21.6 13.6 Source: The Evidence of Drug Addicts and Abusers in BiH (Ministry of civil affairs BiH, 2011) Table 5-2: Opioid substitution treatment in 8 drug treatment centres Indicator All patients on substitution treatment Patients on methadone during the year Patients on Suboxone during the year Patients on methadone at the end of the year (31.12) Patients on Suboxone at the end of the year (31.12) Gender* Males Females Age group* 15-19 20-24 25-29 30-34 35+ 2009 1,151 1,000 151 812 49 2010 1,183 1,022 154 700 130 896 84 1,091 92 5 105 249 205 191 0 61 257 246 226 Note: *In some centres, information on gender and age was not available or not available for all clients during the year. Source: The Evidence of Drug Addicts and Abusers in BiH (Ministry of civil affairs BiH, 2011) 29 Table 5-3: Number of patients in substitution treatment in 8 drug addiction centres in 2010 Centre Doboj Zenica Odzak Sarajevo Banja Luka Tuzla Sanski Most Mostar Total 2009 29 308 7 381 52 52 41 281 1,151 2010 26 307 17 359 58 59 37 320 1,183 Source: The Evidence of Drug Addicts and Abusers in BiH (Ministry of civil affairs BiH, 2011) Approx. 250 patients annually underwent detoxification; approx. 60 of them in a short-term methadone detoxification (see Table 5-4). Table 5-4: Detoxification treatment in 8 drug treatment centres Indicator Number of beds Number of patients in residential treatment (detoxification) Short-term methadone program (detoxification) 2009 23 252 65 2010 21 247 60 Source: The Evidence of Drug Addicts and Abusers in BiH (Ministry of civil affairs BiH, 2011) 5.4.2 Clients in therapeutic communities The total number of clients in 8 therapeutic communities for males11 in 2009 and 2010 was around 364 and 326 beneficiaries, respectively. The average age was 27. Total number of beds was 265 in 2010. 11 Cantonal Therapeutic Community “Kampus”, the Center for Spiritual Rehabilitation “CSI Izlaz”, Center for Rehabilitation of Addicts Smoluca, Association Victoria (Bastasi and Stricici), Centre for Treatment of AddictionUGPROI, Therapeutic Community "Milosrdni otac (Merciful Father)", Therapeutic Community "Izvor – Kruh Svetog Ante (Source-Bread of St. Anthony)”. 30 Figure 5-4: Number of clients treated in 8 therapeutic communities in 2009 and 2010 90 80 70 60 50 40 30 20 10 0 Center for Center for Spiritual Cantonal TC Kampus Rehabilitation "Exit" rehabilitation of Rakovica drug addicts-Smoluća Ilijaš NGO Viktorija Bastasi Stričići Center for Drug Addiction UGPROI Kakanj TC ”Milosrdni otac” Međugorje Center for Drug AddictionMarjanovac ATD 2009 61 49 83 36 33 41 61 ATD 2010 58 33 52 33 29 44 61 TC ”Izvor”-Kruh Svetog Ante Plehani 16 Source: The Evidence of Drug Addicts and Abusers in BiH (Ministry of civil affairs BiH, 2011) 5.4.3 Research on social and emotional characteristics of clients in drug treatment A comparative survey to identify the differences in life experience, priorities in satisfaction of needs, regulation and control of emotions and perceptions of the future among young drug users and non-users aged 18–30 was conducted in BiH in the period from February 2008 until January 2009 (Radetic-Lovric, 2011). The sample consisted of two groups: 232 drug users (heroin addicts involved in drug treatment programs) and control group of 669 respondents who have no experience with drugs. In a sample of drug addicts there were 76.3% men and 23.7% of women, while the control group had 59.9% men and 40.1% women. The study was conducted in drug treatment centres in 5 cities of BiH (Banja Luka, Sarajevo, Zenica, Tuzla and Doboj). The control group consisted of students from various faculties of the University of Banja Luka and Eastern Sarajevo. Various standard instruments were used to measure social and emotional characteristics of both groups. The results showed that the life experience of addicts contained a significantly higher number of stressors then the control group. Of the 28 stressors grouped in clusters (war events, loss of parents, illness and absence of parents, social-pathological phenomenon in the family, material and housing conditions, lack of social support, social pathology of the individual), 24 were more common among drug addicts. Addicts were less satisfied with their life as compared with independents. Drug users usually committed crimes some time after they started consuming drugs in order to obtain money for drugs. However, approx. 15% of drug users were arrested before their first drug consumption and 11 (4.7%) of 232 drug users committed murder before any drug use. 31 Drug users were more socially mobile, and have a lower degree of trust and open communication with parents. Emotional competence (intelligence) was lower in the group of addicts, with a greater effect of negative emotion on thinking, memory and the ability to control emotions. 32 6. Health correlates and consequences 6.1 Introduction BiH has recorded AIDS statistics since 1986/87, with HIV infection also included since 2003. No regular statistics on reported incidence of hepatitis B and hepatitis C related to drug use have been maintained. Results of two sero-behavioural HIV and HCV prevalence surveys conducted by UNICEF among injecting drug users in 2007 and 2009 are available. Moreover, data on HIV, HCV and HBV prevalence among clients in substitution treatment has recently become available. In the recent years, data on drug-related deaths is collected from forensic medicine specialists and the extraction of data on drug-related deaths from general mortality statistics has been performed recently. 6.2 Drug related infectious diseases 6.2.1 Reported incidence of infectious diseases (newly diagnosed cases) By the end of 2009, the total number of registered HIV-positive individuals in BiH was 163 (of that number, 129 were males). In 2009, six new cases, all among males, were recorded. The route of transmission is predominantly heterosexual; 21 IDUs were recorded or 13 % of the total. Of the total of 21 infected IDUs, 19 were male. In 2007–09, no new HIV infection was reported in IDUs (ECDC and WHO, 2010). The surveillance system for viral hepatitis does not allow monitoring of relation of newly diagnosed cases to drug injecting. Nevertheless, for example, total reported cases of viral hepatitis in RS in 2009 were 73 acute HCV cases, 66 acute HBV, 44 HBsAg carriers, and 4 cases of unspecified VH (Public Health Institute of the RS, 2010). 6.2.2 Prevalence of infectious diseases among drug users The prevalence data of HIV and hepatitis C (HCV) among IDUs in BiH is based on two sero-behavioural surveys conducted by UNICEF in 2007 and 2009 in Sarajevo, Banja Luka and Zenica (UNICEF 2007; UNICEF 2010). The prevalence of HIV among IDUs in BiH appears to be very low in both surveys, however, the results of the studies suggest an increase in HCV prevalence among IDUs between 2007 and 2009 (see Table 6-1). The prevalence of HBsAg was found to be 6.9% in Sarajevo, 0.5% in Banja Luka and 3.6% in Zenica in the 2007 study. Table 6-1: HIV and HCV prevalence among IDUs in 3 cities in 2007 and 2009 City Sarajevo Banja Luka Zenica HIV (abs. number/sample size) 2007 2009 1/260 1/261 1/260 2/260 0/260 0/260 HCV (%) [95% CI] 2007 2009 46.2 [37.8;54.0] 49.7 [40.9;58.2] 43.4 [35.8;51.5] 50.6 [42.8;59.0] 18.9 [12.9;27.4] 19.5 [12.3;27.2] Source: Sero-behavioural surveys in IDUs (UNICEF 2007; UNICEF 2010) 33 Prevalence rates of HIV, HCV and HBV can be also obtained from the Drug Treatment Register. Total number of persons in substitution treatment infected with HIV in 2009 and 2010 was 3 and 4 patients (0.3 %), respectively. The percentage of HCV varied between 10% and 50% among the eight treatment centres, with mean values of 27.5% and 37.0% in 2009 and 2010 (see Table 6-2); the highest levels were reported in treatment centres in Sarajevo and Banja Luka. Table 6-2: Prevalence of infectious diseases and mortality among clients of opioid substitution treatment in 8 drug treatment centres Indicator Clients in total HIV+ HCV+ HBV+ Co-infected with HCV and HBV Deceased (mortality rate) 2009 N % 1,151 100.0 3 0.3 316 27.5 56 4.9 17 1.5 15 1.3 2010 N 1,183 4 438 53 10 7 % 100.0 0.3 37.0 4.5 0.8 0.6 Source: The Evidence of Drug Addicts and Abusers in BiH (Ministry of civil affairs BiH, 2011) In the period 2004–2009, the Institute for Alcoholism and Substance Abuse of the Sarajevo Canton treated 878 opiate addicts who were positive for HBV in 36 cases (4.1%) and for HCV in 178 cases (20.3%). Analysis of trends has shown a downward trend in HBV annual prevalence rates from 5.52% to 2.17%, and the increase in HCV annual prevalence rates from 16.33% to 27.78%. Prevalence of infectious diseases in IDUs in prison In 2010, NGO Viktorija conducted a survey on HIV and HCV prevalence in prisons through administration of testing to 143 persons in Tunjice prison. Among those tested, 42 were IDUs, 78 other prisoners and 23 were employees. Approximately 50 % of IDUs tested positive for HCV. One percent of other (non-IDU) prisoners and none of employees tested positive for HCV. No case of HIV infection was detected. 6.2.3 Injecting and sexual risk behaviour Information on risk behaviour is available from sero-behavioural surveys conducted by UNICEF in 2007 and 2009 (UNICEF 2007; UNICEF 2010). Use of sterile injection equipment during the last injection was reported by 86 % of IDUs in Sarajevo, 74 % in Banja Luka and 78 % in Zenica. However, one-third of respondents in 2009 had, within the last month, injected with needles or syringes already used by someone else, and nearly one-third of respondents had given their used needles and syringes to one or more other persons in the past month. In most cases, used needles and syringes were borrowed from close friends or sexual partners. In the month preceding the survey, pharmacies were a more common source of sterile needles and/or syringes than harm reduction services. It is estimated that 41% respondents in Banja Luka, 61% in Sarajevo and 54% in Zenica had two or more sexual partners over the past year. It is estimated that 78% respondents in Sarajevo, 80% in Banja Luka and 71% in Zenica had sexual intercourses with a permanent partner. In all cities, about half had random 34 sexual partners in the last 12 months. Condom during intercourse with random partner over the past year was always used by 21% of respondents in Zenica, 29% in Banja Luka, and 58% in Sarajevo. The main sources of supply of condoms in all three cities are street kiosks and gas stations, while slightly less than half of them in the previous year received condoms from the specialized agencies in this field – NGOs working on harm-reduction and health institutions. It is estimated that 69% of injecting drug users in Banja Luka, 73% in Zenica, and 78% in Sarajevo know where they can get testing for HIV, most of them mentioned a centre for voluntary counselling and testing (VCT) at a clinic for infectious diseases and/or hospital. 39% respondents in Zenica, 45% in Banja Luka and 77% in Sarajevo have at some point done the HIV test. A clinic for infectious diseases and/or hospital is often mentioned as the place where the last test was given. Over 80% clients in Banja Luka and over 90% in Zenica and Sarajevo knew the result of the last HIV test. Testing for HCV was reported by 39% clients in Zenica, 35% in Banja Luka and 79% in Sarajevo, of which 26% in Zenica and about a third in Sarajevo and Banja Luka indicated that they were diagnosed with HCV infection. The 2009 study found a positive trend in the extent of provision of harm reduction interventions, as well as an increase of safe injection practices and sexual behaviour compared with 2007. There was an increase in the proportion of IDUs using condoms with casual sex partners, decreased sharing of injecting equipment and an increase in HIV testing among IDUs. Greater awareness of risk factors and increased use of local harm reduction services were also observed. The proportion of IDUs who received sterile injecting equipment in harm reduction services increased between 2007 and 2009 from 1 % in 2007 to 14 % in 2009 in Banja Luka, from 6 % to 39 % in Sarajevo and from 8 % to 41 % in Zenica. 6.3 Other drug-related health correlates and consequences Disorders related to substance abuse and addiction often occur in combination with other mental, neurological and/or somatic disorders that further complicate the health and social status of drug addicts, both in terms of diagnosis and early detection, and in terms of treatment and rehabilitation. The most common co-morbid conditions that are associated with addiction are behavioural and personality disorders (emotionally unstable personalities prevail), neurotic disorders, stress related, while majority of cases could relate to the post-traumatic stress disorder and adjustment disorder, and affective disorders (mood disorders/swings) with predominantly depressive symptoms. A lower proportion of addicts also had psychotic disorders. In a survey conducted at the Department of Drug Addiction of the Institute for Alcoholism and Substance Abuse of Sarajevo Canton in 2004–2006 in the sample of 366 patients – heroin addicts, psychiatric comorbidity was present in 16% cases. Out of this number there were up to 34 (9.3%) patients who verbalized events during therapeutic process from various periods and had manifested symptoms of posttraumatic stress disorder (PTSD), 8 demonstrated symptoms of psychotic disorder, 2 had organic delusional condition, and 10 emotionally-unstable personality disorder. In another study which was conducted in the same institution in 2005 in a sample of treated heroin addicts, 55–57% had a high depression score, and 36% presented anxiety symptoms. The same study found that adolescents who are addicted to heroin manifest a significant level of depressive symptoms 35 both at baseline and in the phase of abstinence, and that over 50% had symptoms of severe depression in Beck Depression Inventory, 76% moderate to severe depression in Hamilton Depression Rating Scale, and only 5.7–7.9% did not have any symptoms of depression. 6.4 Drug related deaths and mortality of drug users In BiH the statistics of drug related deaths are poor, due to the lack of a reference laboratory for forensic toxicology, incomplete laws relating to DRD, very important role of District Prosecutor (who decides when and what kind of autopsy will be performed) and an inadequate system of data collection. A special register is not legally recognized and approved, and entries by forensic examiners are not mandatory. Complete forensic autopsy together with forensic toxicology is not carried out in all cases of sudden and violent deaths even if there is suspicion of drug abuse. Only the external examination is mandatory. Procedures for autopsy and toxicological analysis have not been standardised, and thus they vary across the country and entities. However, there are recent efforts to deal with and solve those problems. In BiH, there are two forensic medicine institutes — the Institute for Forensic Medicine of the RS in Banja Luka and the Institute of Forensic Medicine, Medical Faculty of Sarajevo University in the Federation of BiH12; they were declared as reference forensic toxicology laboratories in BIH by the Commission on Narcotic Drugs in 2010. However, to date there is still a lack of equipment to equip and make these two laboratories operational.13 The proposed Law on the Prevention and Suppression of Drug Abuse, which is awaiting adoption by the parliament, also specifies that in all drug-related death cases, an autopsy and toxicological analysis of body fluids and internal organs shall be performed. Thus, it is worthwhile to note that the available data presented below is likely to be incomplete, and therefore does not provide a complete overview of drug-related mortality in BiH. 6.4.1 Fatal drug overdoses recorded by forensic medicine departments Until 2010, no data on direct drug-related death has been systematically collected in BiH. Data on drug-induced deaths in 2009 is available from Sarajevo Canton, Una-Sana Canton in the Federation of BiH and Banja Luka in the RS. These regions represent approximately one quarter of the total population of BiH aged 15–64 years. In these three regions, 16 drug-induced deaths were identified in 2009; of 11 with known gender and age, six were male and five were female, aged from 16 to 50 years. Five cases were identified in Banja Luka, all of them among registered drug users (a complete autopsy was performed in one case, external examination was performed in four cases, but toxicological analysis was not undertaken in any of these five cases). Nine cases (five males, four females, aged 17–50) were reported in Sarajevo out of a total of 247 examinations and autopsies performed in 2009 (two fatal 12 The individual forensic pathologists are also located in Tuzla, East Sarajevo, Mostar, Bihac and Trebinje. 13 In December 2010, the first forensic toxicology laboratory opened at a department of the Institute for Occupational Medicine of Canton Sarajevo allowing for quantitative analysis of psychoactive substances in biological samples (blood, urine, tissues and hair) using the GC-MS method; until that time, the biological material samples taken from cadavers were sent to neighbouring countries for analysis. 36 poisonings by antidepressants and three confirmed cases of heroin overdose; in the other cases, toxicological analysis was not performed), and two fatal heroin overdoses were reported from Una-Sana Canton (a 16-year-old female and a 36-year-old male). Data for 2010 was obtained from 1 department of forensic medicine, district prosecutor offices in 7 districts and independent forensic medical examiners. Data collected in these regions represents approximately 31% of the total population in BiH aged 15-64 years. There is no data obtained from pathology departments where forensic medical examiners perform DRDs autopsies. Eight cases of fatal overdoses were identified according to EMCDDA standard (Selection D) in 2010 (see Table 6-3): - 3 due to opioids/opiates, one of them with presence of methadone together with other non-opioid drug, - no case of overdose due to non-opioid drugs was identified (e.g. by inhalants, amphetamines, cocaine, MDMA or other synthetic (dance) drugs or hallucinogens, - in 2 cases the substance was not identified, - 3 cases were due to medical drugs, one of them by benzodiazepine. Table 6-3: Fatal drug overdoses in the BiH in 2010 according to Selection D by groups of drugs, age groups and gender Drug Male Female Total Gender <15 15–19 20–24 25–29 30–34 35–39 40–44 45–49 50–54 55–59 60–64 >64 Unknown Age groups Only opiates/opioids More substances including opiates/opioids Total opiates/opioids One or more substances, excluding opiates/opioids Unspecified / unknown Total illegal drugs and Inhalants Psychoactive medical drugs Total 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 2 1 0 0 0 0 0 0 0 0 0 0 0 2 1 0 0 0 0 0 0 0 0 0 1 2 3 0 0 0 1 2 3 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 2 0 0 0 0 0 0 0 0 0 2 0 2 0 0 2 3 0 0 0 0 0 0 0 0 0 5 0 5 0 0 0 2 1 0 0 0 0 0 0 0 0 0 0 2 5 1 0 0 0 0 0 0 0 0 1 6 2 2 3 8 Source: Data collection on DRDs in forensic medicine agencies (Sarajlic 2011) After extrapolating direct drug-related deaths recorded in 2009 and 2010 to the total population of BiH, the annual overdose-related mortality rate in the country can be estimated approx. as 10–25 deaths per million population aged 15–64. 6.4.2 Drug-related deaths in the general mortality register In all cases of death in BiH, the physician diagnosing the death must complete a death certificate which, in case an autopsy is performed, is augmented by an autopsy diagnosis and sent to the register of births and 37 deaths. At the register of births and deaths, data from the Certificate of Post-mortem Examination is sent to the entity Institutes of Statistics. After the data is fully collected, it is sent to the entity Institutes of Public Health, where WHO recommendations for coding causes of death are applied, and again sent back to the entity Institutes of Statistics. The structure of cases of fatal drug overdoses in the general mortality register in 2010 according to EMCDDA standard (Selection B) by age, gender, and type of drug is presented in Table 6-4. Trend data of Selection B by drugs is shown in Table 6-5. Table 6-4: Fatal drug overdoses in BiH in 2010 according to Selection B in the general death register by groups of drugs, age groups, and gender Opiates/opioids Other drugs Drugs further unspecified Total 0 0 0 0 0 0 0 0 1 0 0 1 2 0 0 2 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 3 0 0 3 Total Drug Female Gender <15 15–19 20–24 25–29 30–34 35–39 40–44 45–49 50–54 55–59 60–64 >64 Unknown Male Age groups 0 0 0 0 3 0 0 3 Source: Data extraction on DRDs from general mortality statistics (Public Health Institute of RS 2011; Public Health Institute of FBiH 2011) Table 6-5: Fatal drug overdoses in BiH according to selection B in the general death register by groups of drugs in 2009 and 2010 Opiates/opioids Year 2009 2010 Total 5 2 Of which methadone 0 1 Other drugs Drugs further unspecified Total 0 0 0 0 5 3 Source: Data extraction on DRDs from general mortality statistics (Public Health Institute of RS 2011; Public Health Institute of FBiH 2011) 6.4.3 Mortality of drug users Mortality study in the group of drug users has not been performed in BiH so far. There is indicative data available on annual mortality rate from all causes in clients in opioid substitution programmes, which reached 1.3% in 2009 and 0.6% in 2010 (see also Table 6-2, page 34). 38 7. Responses to health correlates and consequences 7.1 Introduction Harm reduction programs have been incorporated into the National drug strategy 2009-2013. The goal of harm reduction strategies and approaches is to reduce the negative consequences and outcomes of drug abuse. They help to reduce drug overdoses, risk of HIV and hepatitis infection, and other health and social consequences, such as criminal and other high-risk behaviours. Apart from substitution treatments (see above), harm reduction interventions represent programmes for exchange of needles, syringes and other paraphernalia and injecting equipment, dissemination of information, access to voluntary testing and counselling, vaccination and treatment of infectious diseases, overdose prevention interventions and others. 7.2 Prevention of drug related emergencies and reduction of drugrelated deaths Participation of opiate drug users in substitution treatment (see above), especially by partial agonist buprenorphine (Suboxone), decrease the risk of overdose. Other overdose management strategies in BiH include peer-to-peer education in first aid and resuscitation, establishing collaborations among peers and encouraging peers to seek help and call an ambulance when an overdose is suspected. These activities are promoted and performed especially by NGOs providing harm reduction interventions (see further). 7.3 Prevention and treatment of drug-related infectious diseases 7.3.1 Low-threshold harm reduction programmes Injecting drug users are reached through outreach programmes and drop-in centres. Four NGOs work in the area of harm reduction, employing low-threshold and outreach approaches. Three implement needle and syringe programmes (NSP): - the Association for Assisting Drug Addicts (UG PROI) operates a drop-in centre and outreach programme in Sarajevo; - the NGO Margina operates outreach programmes in Tuzla, Zenica, Mostar, Sarajevo in the Federation of BiH and Doboj in the RS; - the NGO Poenta operates a drop-in centre and outreach programme in Banja Luka. - the NGO Viktorija provides low threshold services in Banja Luka, except a needle and syringe programme. In total, seven drop in centres (in Zenica, Sarajevo, Mostar, Brčko/Tuzla, Bijeljina and two in Banja Luka) have been established. Drop-in centres regularly provide information and counselling in relation to HIV, related harm and needle-exchange. Needle and syringe exchanges are conducted also in the outreach work. 39 Outreach work within the population of IDUs is implemented through the network of outreach workers and gatekeepers.14 Outreach workers and gatekeepers meet in the reference office once a week to get new sterile needles and syringes, condoms, citric acid and other injection materials. All materials for distribution are wrapped in a package called a “safety injection box” for further distribution. Kits consist of a weekly supply of sterile needles and syringes, condoms, citric acid, cooker, cream for veins, latex tourniquets, garter, water for injection, and promotion material with information about the nearest voluntary counselling and testing centre. The outreach work also included visits to sites where young people gather on a daily basis, such as cafes, discos, bars, student dorms, concerts, etc. Other activities performed are: individual and group therapeutic work with addicts and their relatives, daily residence for drug users, SOS phone lines, developing motivation for treatment and abstinence, distribution of condoms and lubricants, distribution of educational material, social services for drug users and referral to other institutions such as methadone treatment, mental health centres, psychiatric clinics, therapeutic communities or social welfare centres. Activities also include prevention activities among non-injecting drug users and at-risk youth in cooperation with other governmental and youth organisations, as well as representatives of the police structure. Apart from injecting drug users (IDU), sex workers (SW), men who have sex with men (MSM), and prisoners are also target groups for harm reduction programmes. Information materials from the needle exchange programmes were also delivered to pharmacies. Educational material consisted of basic information on HIV, Hepatitis B and C, the importance of using sterile equipment for drug injection, the importance of testing for HIV and other STIs, behavioural risk for HIV infection, etc. In seeking new strategies to reach more clients, agreement on collaboration with some central pharmacies in Sarajevo were made, in which pharmacy staff referred IDUs to outreach workers stationed in front of pharmacies during weekend evenings, who then provided all information regarding prevention and provision of needles and syringes. In the framework of the programme Coordinated National Response to HIV/AIDS and Tuberculosis in WarTorn and Highly Stigmatised Settings 2006–2008, 4,326 contacts with IDUs (out of which 825 were new contacts) were registered; 44,247 needles, 26,405 syringes, 9,215 condoms and 690 items of information material were distributed in the Federation of BiH. In the framework of the above-mentioned programme, 1,980 contacts with IDUs were reported (out of which 400 were new contacts), 25,241 condoms and 20,991 items of information material were distributed in the RS during the same period. In 2009, 46,000 harm reduction kits, 145,604 needles (133,537 in the Federation of BiH and 12,067 in the RS), and 96,040 syringes (88,640 in the Federation of BiH and 7,400 in the RS) were distributed in Zenica, Sarajevo, and Banja Luka. In total 557 new clients (516 males, and 41 females) were reached in drop-in centres in BiH in 2009 (Figure 7-1). 14 Gatekeepers are usually people that come from active IDU populations, whereas outreach workers are mostly recovered addicts or non-users. 40 Figure 7-1: New IDU clients reached through drop-in centres in BiH in 2009 600 500 400 300 200 100 0 Females Males Zenica Sarajevo Mostar Banja Luka Bijeljina Tuzla Brčko Total 8 3 2 10 4 5 9 41 107 24 219 67 11 28 60 516 Source: Annual report on activities and results in national response to HIV/AIDS and Tuberculosis (UNDP BiH 2011) The psychologists from drop-in centres in Banja Luka and Doboj provided information on risks related to injecting drugs and unprotected sex through a group session, while individual sessions were provided for drug addicts who wanted to accomplish drug abstinence. In total 275 IDUs received counselling in drop-in centres in Banja Luka and Doboj (see Figure 7-2). Parallel to work with individual drug users, therapists worked with parents and family members of drug addicts. Family members constitute a marginalised group and they also need support and education on the risks and consequences of taking drugs. They frequently participated in weekly educational/informative group meetings. Figure 7-2: New IDU client receiving counselling through drop-in centres in Doboj and Banja Luka 300 200 100 0 Doboj Banja Luka Total Males 58 188 246 Females 14 15 29 Source: Annual report on activities and results in national response to HIV/AIDS and Tuberculosis (UNDP BiH 2011) The project "Choice" funded by UNDP BiH (Global Fund Program in BiH) is being implemented since August 2007. The main goal is to reduce the damage and consequences such as HIV and other blood and sexually transmitted infections in the population at risk (injection drug users). In the drop-in centre in Banja Luka, drug users can get all the information and counselling on HIV, hepatitis B and C, psychosocial support and assistance, condoms, educational print materials and so on. Another one of the activities is to organize training for police officers in BiH on harm reduction in the population of injection drug users. 41 NGO Victoria is implementing the project Protect Yourself (under the sponsorship of UNDP BiH, the Global Fund Program in BiH), whose main goal is education, information and change of behaviour of injection drug users in relation to HIV and other infections. NGO Victoria conducts outreach programmes for injecting drug users and prisoners in the territory of five towns in the RS: Banja Luka, Doboj, Prijedor, Gradiska and Foca, including advice and information on HIV, distribution of condoms and lubricants, distribution of promotional materials, referral to free anonymous HIV testing and so on. The project started in July 2007 and continues to date. 7.3.2 Voluntary counselling and testing centres There is a network of 19 Information, voluntary counselling and testing centres (VCTCs) in BiH located at departments for infectious diseases in hospitals or in public health institutes in major cities. They provide anonymous and free-of-charge HIV testing and pre-test and post-test counselling on the basis of informal consent to various risk groups and individuals. In 2009, 6,943 clients were tested (4,739 males and 2,204 females), 7,158 pre-test (4,894 males and 2,264 females) and 6,355 post-test (4,420 males and 1,935 females) counselling sessions were performed, 19,385 condoms and 9,632 information materials were distributed. In 2010, approximately 7,194 clients were tested (15 were found to be HIV positive), 7,068 pre-test and 6,361 post-test counselling sessions were performed, 22,197 condoms and 12,227 information materials were distributed to clients of VCTCs. The number of clients who were IDUs is not known. 7.3.3 Vaccination against HBV Regulations on Immunization and Chemoprophylaxis Against Infectious Diseases (Official Gazette No. 4/08), Article 32, stipulates mandatory immunization against hepatitis B in various categories such as healthcare workers, patients on haemodialysis, haemophiliacs etc., including injecting drug addicts. Vaccination of persons referred to in Article 32 is done upon previous testing on hepatitis B markers and is not performed in persons which have undergone HBV in past. However, information on HBV vaccination rate in injecting drug users in BiH is not available. 7.4 Responses to other health correlates and consequences Dual diagnosis of the drug abuse and other mental disorders in psychiatric and other health services is present in a high percentage (over 50%) of drug users. Co-morbid disorders present a specific diagnostic and therapeutic problem and require a special integrative, multidisciplinary approach and proper networking between several levels of medical care. In particular, for cases of co-morbidity of addiction and other disorders, treatment is provided primarily in the services for addiction treatment, and depending on other symptoms, cooperation is achieved with specialists from other medical disciplines such as internal medicine, infectious diseases, surgeons, gynaecologists, dentists and others. In recent years, there is an increased number of addicted pregnant women in some treatment programs, which has resulted in intensified cooperation of centres for addiction treatment and gynaecology clinics as well as centres for social work. 42 8. Social correlates and social reintegration 8.1 Introduction Social reintegration is included in the National Action Plan against Drug Abuse in BiH for 2009-2013, within the strategic area of treatment and social reintegration. It involves various measures aimed at housing, employment, education and social reintegration after the release from treatment or imprisonment. Special focus is given to youth and juveniles. 8.2 Social exclusion and drug use According to 2007 UNICEF sero-behavioural study, approx. 80% of problem (injecting) drug users were unemployed. According to the 2009 UNICEF sero-behavioural study, 73% - 77% of participants had high school education and 10-13% had completed elementary school. The main source of income during the last month was family, temporary or a part time job and permanent employment. Average monthly income during the last 12 months rarely exceeds 700 BAM (i.e. 360 €) with almost one half of respondents who had an income from 100 to 700 BAM. Around two thirds of IDU population had been stopped and asked for an identification document by the police during the last year. Estimated 40-49% had been arrested or detained during the last year. Almost half had been exposed to violence or abuse from the police in the last year. More than half is estimated to have been imprisoned (participants in Sarajevo) – see also chapter on Problem drug use, page 18. According to the Institute for Alcoholism and Substance Abuse of Sarajevo Canton, the largest proportion of recovering addicts has no occupation (31.6%), 20% are technicians, 12% traders, 2% servants and students account for 1% of treated clients. 8.3 Social reintegration Information about rehabilitation programs for drug users in therapeutic communities is provided in chapter Social rehabilitation, page 25. Recently, employment bureau in Sarajevo Canton started pilot employment programme for disadvantage groups including drug users. 43 9. Drug-related crime, prevention of drug related crime and prison 9.1 Introduction According to The Law on Prevention and Suppression of Abuse of Narcotic Drugs, the term narcotic drug means any substance of natural or artificial origin, which is included in the list of drugs act under international conventions on drug control or by a decision of competent authorities in BiH. Criminal offences include: cultivation of the plant from which narcotic drug could be obtained, possession of the means for the manufacture of narcotic drug and manufacture, traffic in and possession of a narcotic drug, psychotropic substances, plants or the part of the plant from which a narcotic drug could be obtained or precursors contrary to the provisions of the law, and the use of narcotic drugs outside therapeutic indications, in excessive dose levels, or over an unjustified period of time. Article 77 of The Law on Prevention and Suppression of Abuse of Narcotic Drugs stipulates that registers be kept by various ministries and official bodies; however some of the registers have not been established yet: - Ministry of Security shall keep records on reports of crimes and offences related to narcotic drugs. - Ministry of Justice of BiH shall keep records of persons duly sentenced for crimes and offences relating to narcotic drugs and the execution of sentence of imprisonment and other sanctions and measures against perpetrators of drug crime. - Ministry of Finance and Treasury shall keep records of the quantities of seized drugs, cash and other property from illicit traffic in narcotic drugs. - Ministry of Civil Affairs shall keep the records on social assistance, drug and occasional drug abusers. - The Agency for Medical Products and Medical Devices of BiH shall keep records of licenses issued under this Law. - Customs Sector of the Indirect Taxation Authority of BiH shall keep records of reports of customs violations related to narcotics. 9.2 Drug-related crime Number of crimes related to the abuse of narcotic drugs in 2010 decreased by 88 crime offences (6.3%) as compared with 2009 (see Table 9-1). 44 Table 9-1: Drug criminal offence in BiH in 2009 and 2010 Police Agency BiH Federal Ministry of Internal Affairs Ministry of Internal Affairs of the RS * Police of Brcko District of BiH BiH Border Police BiH State Investigation and Protection Agency (SIPA) Total in BiH 2010 953 213 54 38 42 1 300 2009 1087 197 45 52 7 1 388 Change (%) - 12,3 8,1 20,0 - 26,9 500 - 6,34 Note: * In the RS, the offence of illegally possession of narcotics leads to the criminal offence procedure (Article 42 of the Law on Production and Trade of Narcotic Drugs of the RS). In 2010, infringement proceedings were initiated against 162 persons for illegal possession of narcotics. Source: Analytical data-base of drug crime offences and seizures (Ministry of Security BiH 2011) 9.3 Prevention of drug-related crime In 2010, the police agencies have continuously worked to reduce the supply of narcotic drugs by applying appropriate provisions of the law regulating this area. Along with law enforcement activities, the police agencies have undertaken certain preventive activities with the primary aim of reducing demand for narcotics. Thus the representatives of the Ministry of Internal Affairs of the RS participated in the following projects: Police Activities in Multiethnic Communities, School Police Officer and Opened Doors. In the Federation of BiH preventive activities were implemented through community policing, organizing of a number of lectures for school children and young people, teachers, parents, through the establishment of multidisciplinary local prevention teams, through the exercise of permanent education of police officers, through the exchange of information with other bodies and institutions responsible for the area. 9.4 Interventions in the criminal justice system In 2010, the Criminal Code of BiH received some amendments related to the form of criminal sanctions under Article 195 Illicit Trafficking in Narcotic Drugs, Paragraph 1), 2) and 3) of the Criminal Code of BiH: - Paragraph 1) of Article 195 of the Criminal Code of BiH was amended and a prison sentence of 1 to 10 years of imprisonment was replaced by at least 3 years; - Paragraph 2) of Article 195 of the Criminal Code of BiH was amended and a prison sentence of at least 3 years was replaced by imprisonment of at least 5 years; - Paragraph 3) of Article 195 of the Criminal Code of BiH was amended and a prison sentence of 6 months to 5 years of imprisonment was replaced by a sentence from 1 to 10 years. In addition, it is important to mention the amendments to the Criminal Code of BiH in Article 42a The Substitution of Imprisonment. According to the latest amendments to the Criminal Code of BiH (Official Gazette No. 08/10) it is possible to substitute a sentence of up to one year, at the request of the convicted person, with a fine to be paid in one lump sum within 30 days. Therefore, a prison sentence of one year can be replaced by a fine of 35,000 BAM (i.e. 17,895 €) i.e. 100 BAM (i.e. 51 €) per day. Substitute fines for prison sentences have already been used in certain cases with final decisions. 45 9.5 Drug use and problem drug use in prisons The problem of drug abuse in prisons in BiH is largely tackled by the state-level Strategy for Supervision of Narcotic Drugs, Prevention and Suppression of Narcotic Drug Abuse in BiH in 2009-2013, and State Action Plan against Narcotic Drug Abuse in BiH in 2009-2013. The Strategy and Action Plan provide a wide range of possibilities of introduction of various activities and working with drug addicts in prisons. BiH has implemented a joint project of the European Union and the Council of Europe titled The Efficient Management of Prisons in BiH. As a result of this project, several documents have been prepared and published as a collection in July 2010. As part of the aforementioned project, an analysis has been conducted of the current circumstances in which addicts are serving prison sentences in BiH. In fact, two prison systems in BiH exist, because all persons convicted by the courts on the territory of BiH serve their sentences in penal institutions either in the Federation of BiH or in the RS. Information on the prevalence rate of infectious diseases among prisoners is given in the chapter Prevalence of infectious diseases among drug users, page 33. 9.5.1 Legal basis The Law on Execution of Criminal Sanctions in the Federation, in Articles 183–187 regulates the obligation of treatment of drug addicts and alcoholics by the institutions in which conditions for such treatment or special medical institution exist (Article 167). However, there is no such medical or penal and correctional institution in the Federation of BiH, so the measure has not been applied in practice. The Law on Execution of Criminal Sanctions in the RS, in Articles 194–195 stipulates that the addiction treatment is regulated in a similar manner as in the law in the Federation of BiH. However, the law in the RS in Article 108 provides a legal basis for testing for infectious diseases, alcohol and drugs in a prison setting, although this basis is not precise enough. 9.5.2 Drug users serving a sentence According to the above mentioned review, Efficient Management of Prisons in BiH, the current situation regarding addicts serving prison sentences in BiH shows that an alarming drug problem is present in all the prisons in BiH. On average, from 30% to 70% of sentenced persons are dependent from and addicted to different types of drugs. Addicts are placed in the collectives together with other prisoners. Very little has been done in the field of treatment of drug users in prisons. Medical procedures performed by doctors do not differ from treatment of other prisoners. They perform an examination, determine appropriate therapy and, if needed, the treatment may be changed. If addicts have an abstinence crisis, they are usually sent to external treatment institutions. There are no specific addiction treatment programs, just intensive individual work that includes more counselling with drug addicts than with other prisoners. 46 Prisons do not have any special strategies dealing with security measures for addicts. In some places, a search may be performed in case of suspicion that a prisoner is either smuggling or in possession of narcotic drugs. Otherwise, they perform detailed searches and view packages that are delivered or sent. More attention is paid to the users of external benefits (for example those temporarily allowed out of prison) who are believed to be attempting to bring drugs into the prison. In cases where drug use is discovered, the Ministry of Interior (MoI) is notified and the drug is submitted to the police. Disciplinary and criminal charges are filed against the convicted person. Prisons have not regulated the education of all employees on drug related issues; very few prisons have organized training for prison guards on recognition of drug use, effective responses, how to treat drug addicts in prisons and how to recognize when they are under the effect of drugs, and how to discover the most common places where drugs are hidden. This training was carried out by officials of the Ministry of Interior, Department of Narcotics. 9.6 Responses to drug related health issues in prisons The prisons in BiH have no specific treatment for drug addicts that can be implemented in prisons. According to the criminal laws in both entities of BiH, persons that commit crimes under the influence of drugs and which present a risk of repeating such offences because of their addiction, may have imposed on them a measure of mandatory treatment of addiction during imprisonment. However, when this measure is imposed, it is often implemented inadequately or not implemented at all, or does not meet its primary role of appropriate and effective treatment that would have satisfactory results in terms of preventing the repetition of a crime after leaving the prison. The reasons for inadequate implementation of these measures are inadequate legislation, insufficient financial resources and lack of training of prison staff. The project “Institutional and Post-Penitentiary Treatment of Drug Addicts” was carried out by the NGO Viktorija in the RS prison units in 2009. The project activities were: - Creating a module for working with addicts in the prison system and educational lectures for prison staff. - Training of project staff and experts to provide therapeutic services for addicts and the development, production and printing of educational brochures for the staff in prisons. - Testing for presence of narcotics in urine. - Individual and group psychotherapy work with drug addicts and counselling with psychiatrists, selfhelp groups for families of addicts and supervision of therapeutic activities. - Counselling and testing for HIV, HBV, HCV, distribution of preventive educational materials. - Social service dependents (for the first time provides for monitoring of prisoners after the prison sentence). - Monitoring and evaluation and presentation of project activities and project promotion. 47 The target population were drug addicts in the Banja Luka Prison, family members of addicts, prison staff, representatives of organizations and institutions that deal with addiction treatment, local and entity governments. The expected results were: an impact on the reduction of drug addiction in the community, reduction of crime rates and recidivism in the population of drug users, reduction of risk behaviours related to HIV/AIDS, HBV, HCV and other blood and sexually transmitted infections in prisons, continued treatment and after-care at the end of sentences (treatments available in the external environment), and the sustainability of treatment programs in prisons. During the project, significant attention was devoted to strengthening the capacity of prison staff and increasing their knowledge and skills about drug abuse problems and the promotion of project activities in order to lobby decision makers about the need for therapeutic treatment of addiction within the correctional institutions. Prison staff has a crucial role in motivating drug addicts to accept treatment and prevention of risky behaviour. 9.7 Reintegration of drug users after release from prison After completing prison sentences, drug addicts return to the community environment. Special care should be provided in order to minimise the risks related to drug use in post-penitentiary period or to support and maintain the recovery from addiction. NGO Viktorija, in cooperation with the Prison Service in Banja Luka, implemented the project titled Institutional and Post-penitentiary Treatment of Drug Addicts (see above) which contained elements of post-penitentiary treatment and after-care. This project is supported by the Development Fund of the United Nations and was the first project of this type to be carried out in the penitentiaries in BiH. 48 10. Drug markets 10.1 Introduction BiH has a strategic location on the Balkan route, which connects drug production centres in Asia and the markets in Western Europe. The country has thus become a regional traffic centre for international trafficking of narcotics in Europe. There are two (sub)routes for trafficking of heroin from Turkey to Croatia (via Serbia and also via Kosovo and Montenegro) and three (sub)routes for trafficking of herbal cannabis (one from Serbia and two from Albania to Croatia). Specific events in BiH in recent years (the country emerging from war, trauma, transition, economic downturn, disturbed system of values, unemployment, poverty, lack of perspectives) represent a fertile ground for the spread of drug phenomena, including illegal drug trafficking, organized crime, money laundering and corruption. The existence of several police agencies in BiH, and the resulting problem of coordination, often result in unbalanced cooperation and sometimes even rivalry between individual police agencies in BiH. However, the police agencies in BiH have carried out several joint international operations in combating illicit drug trafficking, in cooperation with law enforcement agencies in Serbia, Croatia, Slovenia and Italy. Although significant results were achieved in 2010, a similar trend in drug trafficking and its counteracting can be predicted. 10.2 Availability and supply On the territory of BiH, the situation with drug abuse and trafficking is largely complicated and is taking on new dimensions. BiH is both a transit and a destination area for drug trade and is on the so-called "Balkan Route" of drug trafficking. Because of its strategic location, BiH generally faces the same problems faced by other countries on the Balkan Route. Thus, BiH is mainly a transit point for smuggling of synthetic drugs and cocaine from the west, and heroin and cannabis products from the east. In BiH, heroin is transported mainly from the territory of Albania and Turkey via Serbia and Montenegro, hidden in shipments of consumer goods or in buses. After being smuggled into BiH, heroin is sold to a buyer, who then engages "couriers" (in most cases persons without criminal records), mainly passengers of motor vehicles, who continue to transport heroin to Western European countries. It is believed that in recent years the above mentioned pattern has changed, because the lack of internal borders within the Schengen space diverted the smuggling route through the EU countries in South East Europe, primarily through Bulgaria, Romania and Hungary. However, different routes through the Balkan countries of South East Europe should not be treated as separate entities, given that organized crime groups in South East Europe and the former Yugoslavia maintain good cooperation with each other so that a criminal group may use different routes for drug shipments. 49 It was observed that cocaine traffickers from South America use ports in Greece, Montenegro and Croatia, and there are already well established land routes, partly through BiH and further to the Western Europe. In BiH recently, the most frequent narcotic drug has been "skunk", genetically modified potent marijuana. Operative findings suggest that this type of narcotic drug arrives into BiH from Albania via Montenegro to Herzegovina and is then transported on to Western Europe. In addition, there is an increasing evidence of indoor cultivation of genetically modified "skunk" in BiH in illegal laboratories that are equipped with sophisticated equipment. In 2010, police agencies in BiH repeatedly discovered and confiscated such laboratories. 10.3 Seizures Table 10-1: Seizures of narcotic drugs in BiH in 2008–2010 Drug Heroin Cocaine Ecstasy Amphetamine Herbal cannabis Cannabis resin Cannabis plants 2008 2009 27 921 g 3 991 g 543 pcs + 225 g 769 g 90 000 g 17 g 3 812 pcs 18 000 g 1 000 g 11 039 pcs 3 583 g 275 000 g 238 g 2 718 pcs + 649 g 2010 26 473 g 1 506 g 16 505 pcs 1 476 g 465 582 g 3g 7 769 pcs Source: Analytical data-base of drug crime offences and seizures (Ministry of Security BiH 2011) 10.4 Price and purity 10.4.1 Price Table 10-2: Street price of narcotic drugs in three towns in BiH in 2010 (in €) Narcotic Drug Heroin (1 g) Herbal cannabis (1 g) Herbal cannabis – skunk (1 g) Cocaine (1 g) Ecstasy (1 tbl.) Amphetamine (1 g) Sarajevo 25 0,7–1 1,5–2 25–50 2,5 10 Banja Luka 15–25 1 2–3 40–60 2,5–5 7,5 Mostar 25 0,5 1,5 50 1,5–5 10 Source: Analytical data-base of drug crime offences and seizures (Ministry of Security BiH 2011) 10.4.2 Purity The purity of seized drugs is not investigated at the moment in BiH due to lack of equipment. In general, heroin is of poor quality, diluted usually with paracetamol and caffeine. The most common additives for amphetamine are lactose and sucrose. Lactose is also the most common additive in ecstasy. Cocaine is commonly cut by lidocaine. However, during the operation in Sarajevo in March 2010, the State Investigation and Protection Agency (SIPA) seized about 1 kg of cocaine hydrochloride with high-purity and without any additives. This may indicate a difference between wholesale and street quality of drugs. 50 Annexes Abbreviations AAA AIDS ATD BAM BiH CIDA CSI DRD EHIS EMCDDA ESPAD FBiH FTD HBSC HBV HCV HIV ICD IDU IPA LIP MARA MHC MMT MSM NGO NSP PTSD RS SIPA STI SW TDI UNDP UNICEF VCTC WHO Action against AIDS Acquired immunodeficiency syndrome All treatment demand (presentation) Bosnian convertible mark Bosnia and Herzegovina Canadian International Development Agency Centre of Contemporary Initiatives (a name of particular drug treatment centre) Drug related deaths European health interview survey European Monitoring Centre for Drugs and Drug Addiction European School Survey Project on Alcohol and Other Drugs Federation of Bosnia and Herzegovina First treatment demand (presentation in treatment for the first time in a client’s life) Health Behaviour of School Children Hepatitis B virus Hepatitis C virus Human immunodeficiency virus International Classification of Diseases Injecting drug user Instrument for pre-accession assistance Local Initiatives Program Most-at-risk adolescents Mental health centre Methadone maintenance treatment Men having sex with men Non-governmental organization Needle and syringe programme Post-traumatic stress disorder Republic of Srpska State investigation and protection agency Sexually transmitted disease Sex worker Treatment demand indicator United Nations Development Programme United Nations Children's Fund Voluntary counselling and testing centre World Health Organization 51 List of Tables Table 2-1: Lifetime prevalence of drug use, by gender in the Federation of BiH (FBiH) and the RS (RS), 2008 ESPAD survey (%)........................................................................................................................................... 11 Table 5-1: Number and average age of treated clients in 8 drug treatment centres ................................... 28 Table 5-2: Opioid substitution treatment in 8 drug treatment centres ........................................................ 29 Table 5-3: Number of patients in substitution treatment in 8 drug addiction centres in 2010 ................... 30 Table 5-4: Detoxification treatment in 8 drug treatment centres ................................................................ 30 Table 6-1: HIV and HCV prevalence among IDUs in 3 cities in 2007 and 2009 ............................................. 33 Table 6-2: Prevalence of infectious diseases and mortality among clients of opioid substitution treatment in 8 drug treatment centres .......................................................................................................................... 34 Table 6-3: Fatal drug overdoses in the BiH in 2010 according to Selection D by groups of drugs, age groups and gender .................................................................................................................................................... 37 Table 6-4: Fatal drug overdoses in BiH in 2010 according to Selection B in the general death register by groups of drugs, age groups, and gender...................................................................................................... 38 Table 6-5: Fatal drug overdoses in BiH according to selection B in the general death register by groups of drugs in 2009 and 2010 ................................................................................................................................. 38 Table 9-1: Drug criminal offence in BiH in 2009 and 2010 ............................................................................ 45 Table 10-1: Seizures of narcotic drugs in BiH in 2008–2010 ......................................................................... 50 Table 10-2: Street price of narcotic drugs in three towns in BiH in 2010 (in €) ............................................ 50 52 List of Figures Figure 4-1: Injecting drug use among sex workers in their lifetime in BiH (%) ............................................. 21 Figure 4-2: Sexual intercourse under influence of drugs and alcohol among sex workers in their lifetime in BiH (%) ........................................................................................................................................................... 21 Figure 5-1: All treatment demands in 8 treatment centres .......................................................................... 28 Figure 5-2: First treatment demands in 8 treatment centres ....................................................................... 28 Figure 5-3: Percentage of first treatment demands in all treatment demands by 8 treatment centres...... 29 Figure 5-4: Number of clients treated in 8 therapeutic communities in 2009 and 2010 ............................. 31 Figure 7-1: New IDU clients reached through drop-in centres in BiH in 2009 .............................................. 41 Figure 7-2: New IDU client receiving counselling through drop-in centres in Doboj and Banja Luka .......... 41 53 Index abstinence, 36, 40, 41, 46 alcohol, 7, 9, 10, 11, 12, 16, 20, 21, 22, 46 amphetamine, 2, 50 buprenorphine, 2, 25, 39 cannabis, 2, 11, 12, 26, 27, 49, 50 cocaine, 2, 11, 12, 27, 37, 49, 50 co-morbidity, 42 convicted, 45, 46, 47 coordination, 3, 5, 6, 23, 49 costs, 7, 8 counselling, 2, 15, 23, 24, 26, 35, 39, 40, 41, 42, 46, 47 crack, 11 criminal law, 4, 47 criminal offence, 6, 45 detoxification, 24, 25, 26, 27, 30 drug use, 1, 2, 4, 7, 9, 10, 11, 15, 17, 18, 19, 20, 21, 22, 24, 25, 26, 31, 33, 35, 36, 38, 39, 40, 41, 42, 43, 46, 47, 48, 57 drug-related crime, 45 drug-related death, 5, 33, 36, 37, 39 ecstasy, 2, 11, 12, 27, 50 EMCDDA, 1, 9, 18, 23, 27, 37, 38 ESPAD, 1, 9, 10, 11 European Union, 6, 46, 49 evaluation, 1, 5, 6, 17, 47 exchange programme, 40 government, 4, 6, 48 hallucinogens, 37 harm reduction, 1, 2, 4, 8, 23, 34, 35, 39, 40, 41 hepatitis, 18, 33, 39, 41, 42 heroin, 1, 2, 11, 19, 24, 26, 27, 31, 35, 37, 49, 50 HIV/AIDS, 2, 8, 12, 15, 16, 17, 18, 20, 33, 34, 35, 39, 40, 41, 42, 47, 48, 55, 56 children, 9, 12, 14, 16, 45 incidence, 33 inhalants, 12, 37 juveniles, 43 law, 1, 2, 3, 4, 44, 45, 46, 49 lifetime prevalence, 9, 11, 12 low-threshold programme, 39 LSD, 11, 12 magic mushrooms, 11 marijuana, 50 MDMA, 37 media, 14, 16 medicaments, 11 methadone, 2, 8, 19, 24, 25, 26, 27, 29, 30, 37, 38, 40 ministry ministry of finance, 3, 44 ministry of health, 2, 10, 15, 16, 17, 26 ministry of justice, 44 minorities, 14 misdemeanour, 4 mortality, 33, 34, 36, 37, 38 narcotic and psychotropic substances, 1, 7 needle and syringe programme, 40 NGOs, 1, 2, 8, 14, 16, 17, 18, 19, 20, 23, 25, 35, 39 opiates, 2, 11, 25, 27, 37 overdose, 19, 37, 39 policy, 1, 2, 3, 6, 7, 23 possession, 1, 4, 44, 45, 47 prevalence, 1, 2, 9, 10, 11, 12, 18, 20, 33, 34, 46 prevention, 1, 3, 5, 6, 8, 14, 15, 16, 17, 20, 26, 39, 40, 44, 45, 48 indicated prevention, 15 prison, 2, 6, 17, 19, 23, 24, 34, 44, 45, 46, 47, 48 problem drug use, 18, 46 psychiatric co-morbidity, 35 public health, 20, 27, 42 institute, 27, 42 research, 5, 9, 10, 11, 57 sentence, 44, 45, 46, 47 school, 1, 9, 10, 11, 13, 14, 15, 16, 17, 43, 45 smoking, 9 social reintegration, 5, 8, 25, 43 study, 9, 10, 11, 12, 18, 19, 20, 24, 31, 33, 35, 38, 43 Suboxone®, 8, 25, 29, 39 survey, 1, 9, 10, 11, 12, 19, 20, 24, 31, 34, 35, 57 synthetic drug, 2, 49 tobacco, 10, 11, 12 trafficking, 4, 6, 20, 47, 49 treatment, 1, 2, 5, 7, 8, 18, 19, 23, 24, 25, 26, 27, 28, 29, 30, 31, 34, 35, 39, 40, 42, 43, 46, 47, 48 outpatient, 24 residential, 30 substitution, 2, 7, 27, 29, 30, 33, 34, 39 treatment demand, 7, 23, 27, 28, 29 vaccination, 39, 42 54 Bibliography Bojanić, J., Jandrić, Lj., Janković, S., Hecker, T., Matović-Miljanović, S., Stojisavljević, D. (2003). Health Behavior of School Children in the The RS. Banja Luka: Institute for Public Health of the The RS. Ceric I, Oruc L. History of Psychiatric Services in Bosnia and Herzegovina, International Conference of Mental Health Reform in BiH, Dubrovnik, Croatia, Book af Abstracts, September 30-October 2, 1999:7-9. Cerić, I., Loga, S., Sinanovic, O. et al. (2001), ‘Reconstruction of Mental Health Services in Bosnia and Herzegovina’, Medicinski Arhiv, Volume 55(1) suppl. 1, pp. 5–23. Cerić, I., Mehić-Basara, N., Oruč, L., Salihović, H. (2007), ‘Zloupotreba psihoaktivnih supstanci i lijekova’, Medicinski fakultet, Sarajevo. European Centre for Disease Prevention and Control (ECDC)/WHO Regional Office for Europe. HIV/AIDS surveillance in Europe 2009. Stockholm: ECDC; 2010. Available from: http://www.ecdc.europa.eu/en/publications/Publications/101129_SUR_HIV_2009.pdf Hasečić, H., Mehić-Basara, N., Pokrajac, M., Marjanović-Čengić, S., Selman, S., Ploskić, S., Ramić, L., Balić, A., Grabovica, M., Havić, E., Šukurović, N. (2003), ‘Iskustva primjene metadonske terapije u Zavodu za alkoholizam i druge toksikomanije Kantona Sarajevo’, Medicinski Arhiv, Volume 57 (5–6, supl.1). Hudolin, V. (1982), ‘Istina o drogama’, Jugoslavenska medicinska naklada, JUMENA, Zagreb. Jensen BS, Ceric I. (1994) Community-Oriented Mental Health care in B&H, Strategy and Model Project. WHO Office for BiH, Sarajevo. Knesper DJ, Riba MB, Schwenk TL. (1997) Primary Care Psychiatry, WB. Saunders. Loga S, Ceric I. (1999) Development of Mental Health Care in FBiH, Ministry of Health of FBiH. Loga, S. et al. (1999) Klinička Psihijatrija [Clinical Psychiatry], Medical Faculty in Sarajevo and Tuzla . Lovrić-Radetić, S. (2011). Drug Addiction of Young People: Social – psychological Approach and Research. Grafomark, Laktaši. Mehić-Basara, N. (2007), ‘Efekti primjene metadonskog tretmana kod ovisnika o opijatima, magistarski rad’, Univerzitet u Sarajevu, Medicinski fakultet, 2007. Ministry of health of Sarajevo Canton (2008) ‘Inovirani Program prevencije narkomanije, alkoholizma i drugih ovisnosti, za period 2008-2012, godine‘ [The Programme for Prevention of Addictions of the Sarajevo Canton in 2008-2012]. Ministry of health of Sarajevo Canton, Sarajevo. Ministry of civil affairs (2011) ‘The Evidence of Drug Addicts and Abusers in BiH‘, unpublished Ministry of Security BiH (2011) ‘Analytical data-base of drug crime offences and seizures‘, unpublished 55 National Strategy on Supervision over Narcotic Drugs, Prevention and Suppression of the Abuse of Narcotic Drugs in Bosnia and Herzegovina for the period 2009-2013 (2009). Oakley LD, Potter C. (1997) ‘Psychiatric Primary Care‘. Mosby, St. Louis. Peat M. (1997) ‘Communtiy Based Rehabilitation‘. WB Saunders, London. Pekić, S., Smailbegović, T. (2006) ‘Priručnik za multdisciplinarni pristup prevenciji zloupotrebe psihoaktvnih supstanci‘ [Guidelines for multidisciplinary approach in drug prevention] Udruženje za prevenciju ovisnost i smanjenje štete LINK, Sarajevo. Public Health Institute of FBiH (2011) ‘Data extraction on DRDs from general mortality statistics in Federation BiH‘, unpublished. Public Health Institute of FBiH (2002) ‘The Health Behaviour of School Children (HBSC) — Federation of Bosnia and Herzegovina‘. Public Health Institute of FBIH, Sarajevo. Public Health Institute of FBiH (2008) ‘ESPAD 08 — The European School Survey Project on Alcohol and Other Drugs, Federation of Bosnia and Herzegovina Country Report‘. Public Health Institute of FBIH, Sarajevo. Public Health Institute of RS (2011) ‘Data extraction on DRDs from general mortality statistics in Republic of Srpska ‘, unpublished Public Health Institute of RS (2011) ‘The Publication on the Health of Population in 2009‘. Public Health Institute of the RS, Banja Luka. Ravlija J., Jandrić, Lj., Kurtović, A. (2008) ‘Survey of Risk Behaviour Related to HIV Prevalence Among Vulnerable Groups‘. Foundation PH Suisse-Partnerships in Health, Institute of Public Health of the RS, Office of Public Health of the Federation BiH. Sarajlic, N. (2011) ‘Data collection on DRDs in forensic medicine agencies‘, unpublished Savić, J., Milosavljević, B., Branković, D., Dimitrijević, S., Đurašinović, P. (2003). ‘The Youth of the RS at the beginning of XXI Century‘.Faculty of Philosophy Banja Luka, NGO “Zdravo da ste”, Banja Luka. Šiljak, S., Niškanović, J. (2011). ‘European Survey of Narcotic Drug Abuse, Tobacco and Alcohol Use among High School Students‘. Public Health Institute of the RS, Banja Luka. Šiljak, S., Stojisavljević, D., Niškanović, J. (2009) ‘European Survey of Narcotic Drug Abuse, Tobacco and Alcohol Use among High School Students‘. Public Health Institute of the RS, Banja Luka The Law on Prevention and Suppression of Abuse of Narcotics in Bosnia-Herzegovina (2006). The Law on Protection of People with Mental Health Problems (2001). UNDP BiH (2008) ‘The curricula of HIV/AIDS courses, training for medical staff in primary health care‘. 56 UNDP BiH (2011) ‘Coordinated National Response to HIV/AIDS and Tuberculosis in a War-torn and Highly Stigmatized Seting‘ – Annual report on activities and results in 2009 UNICEF BiH (2007) ‘Biological and Behavioural Survey among Injection Drug Users, BiH’, UNICEF, Sarajevo. UNICEF BiH (2007b) ‘Review of legislation, policies and practices, access to adolescents to information and health services with regard to HIV/AIDS and SPIs’, UNICEF, Sarajevo/Banja Luka. UNICEF BiH (2008) ‘Behavioural research among adolescents in collective accommodation in BiH’, UNICEF, Sarajevo/Banja Luka. UNICEF BiH (2010) ‘Report on behavioural and biological surveillance among injection drug users in BiH, 2009: A respondent-driven sampling survey’, UNICEF/UNDP, Sarajevo/Banja Luka. UNICEF Bosnia and Herzegovina (2010) ‘Report on behavioural and biological surveillance among injection drug users in Bosnia and Herzegovina, 2009: A respondent-driven sampling survey’, UNICEF/UNDP, Sarajevo/Banja Luka. WHO (2001) ‘Directions for Diagnosis and Treatment of Mental health Disorders in Primary Health Care‘, ICD-10, Chapter V, Version for Primary Health Care. WHO, Sarajevo. World Health Organization, Division of Mental Health (1989) ‘Consumer Involvement in Mental Health and Rehabilitation Services (WHO/MNH/MEP/89.7) ‘. World Health Organization, Geneva. World Health Organization, Division of Mental Health (1993) ‘Doctor-Patient Interaction and Communication‘. World Health Organization, Geneva. World Health Organization, Division of Mental Health and Prevention of Substance Abuse (1996) ‘Public Mental Health, Guidelines for the Elaboration and Management of National Mental Health Programmes‘. WHO, Geneva. 57
 0
0
advertisement
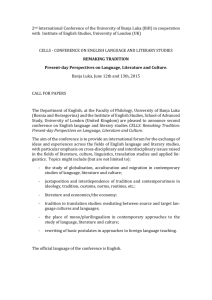



Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users