Running head: INTEGUMENARY DYSFUNCTION - mwsu-wiki
advertisement

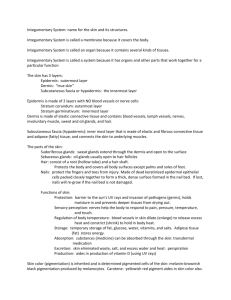
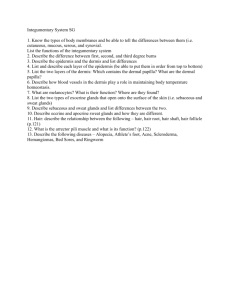
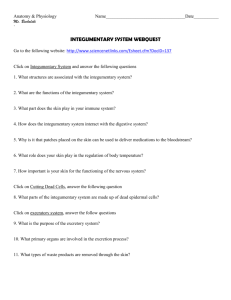
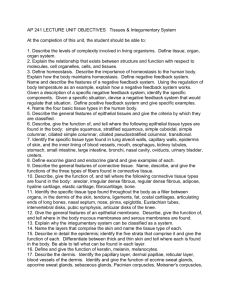
HS Case Study 1 Running head: INTEGUMENARY DYSFUNCTION Case Study: Integumentary Dysfunction Lisa Sheriff, RN Midwestern State University HS Case Study 2 Introduction Family Nurse Practitioners are exposed to a variety of clinical scenarios with many being concerns of the integumentary system. The integumentary system is the largest organ in the body and has vital functions in sustaining life. The skin is a physical barrier against trauma and a window into our sense of identity. To demonstrate a connection with expected normal anatomy and physiology of the integumentary system with one type of dysfunction, a brief review and a case study is presented. Normal Anatomy and Physiology The integumentary system consists of the skin and dermal appendages including nails, hair, sebaceous glands and sweat glands. One centimeter of skin contains three yards of blood vessels, four yards of nerves, ten hair follicles, 15 sebaceous glands, 100 sweat glands, 3,000 sensory cells, and 300,000 epidermal cells (Bryant, 2000). This organ functions as a first line of immunity, allows for excretion of waste, synthesizes vitamins and hormones, regulates body temperature and prevents water and extracellular fluid loss, retrieved 9/17/06 from www.emc.maricopa.edu. Skin is composed of three layers, the epidermis being the outer layer, the dermis, and the hypodermis. See Appendix A for diagram. The epidermis is primarily keratinized stratified squamous epithelium. Other cells in this layer include melanocytes that synthesize and excrete melanin in response to sun exposure, Langerhan cells which initiate immune response with exposure to environmental antigens, and Merkel cells associated with touch receptors. The epidermis is five progressive layers of cells differentiation. These layers include the stratum corneum, stratum luciderm, stratum granulosum, stratum spinosum and stratum basalis (Bryant, 2000). HS Case Study 3 An epidermal-dermal junction separates the epidermis from the dermis with Rete ridges. The dermis layer is the thickest layer and supplies nutrients for the epidermal layer. This layer is where hair follicles, sebaceous glands, sweat glands, blood vessels, and lymph vessels are found. Fibroblasts secrete the connective tissue matrix giving the skin its tensile strength and elastin abilities. Mast cells release histamine in response to antigens, machrophages assist in immunity through phagocytosis, and endothelial cells line the blood vessels (Bryant, 2000). Hair follicles and sebaceous glands are integrated units and are cyclic with periods of growth and rest over different body structures. Sebaceous glands secrete sebum to lubricate the skin and contribute to its ph. Growth is dependent on testosterone. Sweat glands include both the aprocrine located at the axillae, scalp, abdomen, and genital region and the eccrine at the soles of the feet, palms of hands and forehead (McCance and Huether, 2006). The hypodermis attaches the dermis to underlying structures and provides insulation and cushion. This layer contains fibroblasts, machrophages and adipose tissue. Case Study A 55-year-old African American female, V. C., presents to the Family Nurse Practitioner with a chief complaint of “hard bumps at her vagina.” She states, “I have some bumps that come up and hurt terribly around my pubic hairs.” Subjective Data Integumentary dysfunctions require a detailed health history along with identification of the lesions for accurate diagnosis (McCance and Huether, 2006). The patient is asked about chronology of the “bumps”. V.C. states she has had these areas come and go since she started having menstrual cycles at 14 years-old and seem to be worse in the summer. She tends to HS Case Study 4 notice them at her underarms, groin, and breasts without being noticeably more on one side than the other. She remembers the first one started at her underarm. V. C. has pain that is slightly relieved when in the bathtub or running the shower water over the sites. The pain is easy to pinpoint and is at a level four on a zero-to-ten scale. The pain increases to a six with light palpation. She has been using over-the-counter Tylenol and takes Ultram when needed. She has not been diagnosed with any dermatological conditions in her past and denies ever telling a healthcare provided of the condition. She states they are embarrassing and smell bad. She denies lymphangitis. She complains of foul smelling drainage at the bump sites after a couple of weeks and then the sites seem to resolve. She is morbidly obese, diabetic for at least five years and smokes about a pack of cigarettes a day and does not feel like she can stop. She is not currently working. Her children are grown and have families of their own. She takes care of her grandchildren when she is able. Objective Data Physical exam reveals an overall intact integumentary system with exceptions at the axilla and in the folds of the genital region. There are five areas of raised hardened boils. She is not febrile and denies having been recently. One site at the axillae has come to a head and has an obvious malodorous purulent yellow discharge with light palpation. Multiple sites of keloid formation are present bilaterally in areas of aprocrine glands. Pathophysiology of Presented Dysfunction V.C. is suffering from a chronic condition known as Hidradenitis Supprativa (HS). Jamec (2004) states the following: HS Case Study 5 The clinical presentation of the disease is characteristic and allows simple diagnosis. See Appendix B for typical physical presentation of condition. Hidradentitis Supprativa is a “disease of the hair follicle of the inverse areas of the body, predominantly the axillae and genitofemoral areas. The pathogenesis is thought to involve inflammation of diseased follicles and subsequent formation of draining sinus tracts which from the histological main feature of the disease. It has been suggested that specific cells are recruited from the hair follicle epithelium to form sinus tracts following inflammation. ( p. 1767) It is thought that the aprocrine gland may not have completely developed and when the follicle is occluded, the aprocrine gland is occluded leading to perifolliculitis. It is therefore considered a disorder of the terminal follicular epithelium located in the aprocrine gland, retrieved September 17, 2000 from http://www.emedicine.com/emerg/topic259.htm. Caring Holistically V.C. should be educated that this condition is not related to poor hygiene and while it may not be cured, there are treatment options available. She can decrease the severity and frequency of occurrences by not smoking, weight reduction, not shaving in areas of concern, and ensuring clothing is not tight fitting. She should use antibacterial soap to keep the areas clean and dry. An antibiotic may be prescribed and should be completed as directed. Application of a warm wash cloth to the areas is encouraged 3-5 times a day. Once the areas form a head and begin to drain, they will resolve. If the sites become too painful to tolerate, the areas may be incised and drained. Individual lesions generally resolve in 10-30 days, retrieved September 17, 2000 from http://www.emedicine.com/emerg/topic259.htm. HS Case Study 6 Provide V.C. with information on her condition. HS has three stages. The primary stage is when the non-inflamed boil appears. Secondary stage includes the formation of sinus tracts with scaring that may link individual lesions. And tertiary, inflammation and discharge appear. If left untreated, HS can lead to the development of squamous cell carcinoma. Retrieved September 17, 2006 from http://en.wikipedia.org/wiki/Hidradenitis_suppurativa. The incidence rate is not well known, but has been estimated as being between 1:24 (4.1%) and 1:600 (0.2%), retrieved September 17, 2006 from http://en.wikipedia.org/wiki/Hidradenitis_suppurativa. The condition tends to occur more in females than males and more often in African Americans. It is possibly due to the tightly curled hair predisposing the person to ingrown hairs, retrieved September 17, 2000 from http://www.emedicine.com/emerg/topic259.htm. While thought to be a rare condition, it was chosen to be presented because of the three encounters the student has witnessed in the past year. The condition has a profound effect on the patient’s daily life. It is crucial that we as Family Nurse Practitioner assure the patient that they are not to blame and offer hope that they can live a productive life with HS. HS Case Study 7 References American Osteopathic College of Dermatology. (n.d.). Dermatologic Disease Database. Retrieved September 17, 2006 from Web site: http://www.aocd.org/skin/dermatologic_diseases/hidradenitis_suppu.html Bryan, R. (2000). Acute & Chronic Wounds: Nursing Management. Saint Louis: C.V. Mosby. Estrella Mountain Community College. (n.d.). Retrieved September 17, 2006 from ttp://www.emc.maricopa.edu/ Fite, D. (2006, May 22). Hidradenitis Supprativa. Retrieved September 17, 2000 from E Medicine Web site: http://www.emedicine.com/emerg/topic259.htm Hidradenitis Suppurativa. (n.d.). Retrieved 9/17/06 from the Wikipedia Web site: http://en.wikipedia.org/wiki/Hidradenitis_suppurativa McCance, K. & Huether, S. (2006). Pathophysiology: The Biological Basis for Disease in Adults and Children. Saint Louis: C.V. Mosby. HS Case Study 8 Appendix A Diagram of layers of human skin Retrieved from http://en.wikipedia.org/wiki/Image:Skin.jpg HS Case Study 9 Appendix B Retrieved September 17, 2006 from http://www.aocd.org/skin/dermatologic_diseases/hidradenitis_suppu.html