University Graduate Student Plan
advertisement

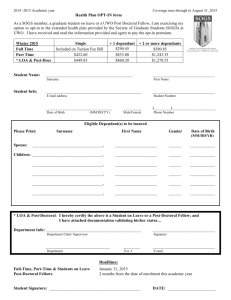
2015 -2016 Academic year Coverage runs through to August 31, 2016 Health Plan OPT-IN form As a SOGS member, a graduate student on leave or a UWO Post Doctoral Fellow, I am exercising my option to opt-in to the extended health plan provided by the Society of Graduate Students (SOGS) at UWO. I have received and read the information provided and agree to pay the opt-in premium. Winter 2016 Full Time FT – Non-residential Part Time * LOA & Post-Docs Student Name: Single Included on Tuition Fee Bill $347.30 $502.20 $532.90 + 1 dependant $347.30 $694.70 $994.40 $1,025.10 + 2 or more dependants $694.70 $1,042.00 $1,486.58 $1,517.30 __________________________________________ Surname Student Info: ______________________________ First Name ______________________________________________ E-mail address ______________________________ Student Number ________________________________ Date of Birth (MM/DD/YY) _________ (________)_____________________ Male/Female Phone Number Eligible Dependant(s) to be insured Please Print: Surname First Name Gender Date of Birth (MM/DD/YR) Spouse: __________________________________, ____________________ ______ ____________ Children: __________________________________, ____________________ ______ ____________ __________________________________, ____________________ ______ ____________ __________________________________, ____________________ ______ ____________ __________________________________, ____________________ ______ ____________ __________________________________, ____________________ ______ ____________ * LOA & Post-Doctoral: I hereby certify the above is a Student on Leave or a Post-Doctoral Fellow; and I have attached documentation validating his/her status… Department Info: ______________________________________________ Department Chair/ Supervisor ______________________________ Signature _______________________________ Department ________ ______________________________ Ext. # E-mail Deadlines: Full-Time, Part-Time & Students on Leave Post-Doctoral Fellows January 31, 2016 2 months from the date of enrolment this academic year Student Signature: ____________________________________________ DATE: _______________________