COPING WITH EXTREMES: From C. difficile to Constipation Daryl
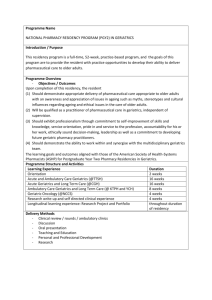
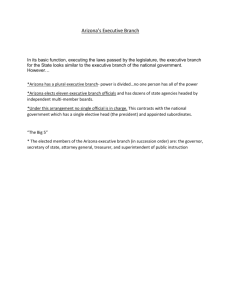
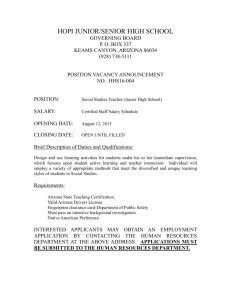
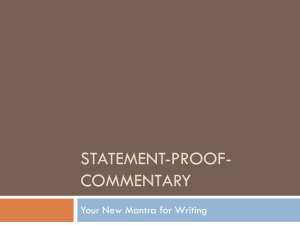
26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society COPING WITH EXTREMES: From C. difficile to Constipation Daryl Hutchinson, MD Arizona Digestive Health Learning Objectives: ● Appropriately evaluate the patient with change in bowel habits, more specifically chronic constipation. ● Become aware and educated on treatment options for chronic constipation. ● Understand the pathogenesis, disease progression and treatment options available for Clostrium difficile colitis. DISCLOSURE OF COMMERCIAL SUPPORT Daryl Hutchinson, MD does not have a significant financial interest or other relationship with manufacturer(s) of commercial product(s) and /or provider(s) of commercial services discussed in this presentation. The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 1 26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society ___________________________________ ___________________________________ Coping with GI Extremes ___________________________________ ___________________________________ Daryl S. Hutchinson, M.D. ___________________________________ Clinic for Digestive Diseases, P.C. A division of ___________________________________ Arizona Digestive Health Sun City and Surprise, AZ ___________________________________ ___________________________________ Epidemiology ___________________________________ • Constipation is a chronic condition causing pain, reduced ability to function and poor overall general health • Estimates of 4-56 million people in the US alone suffering leading to 2.5 million annual medical visits to a primary care physician or gastroenterologist • More common in women & elderly ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ • Johanson JF, Sonnenberg A, Koch TR. Clinical epidemiology of chronic constipation. J Clin Gastroenterol. 1989;11:525–536. • Stewart WF, Liberman JN, Sandler RS, et al. Epidemiology of constipation (EPOC) study in the United States: relation of clinical subtypes to sociodemographic features. Am J Gastroenterol. 1999;94:3530–3540 • Sonnenberg A, Koch TR. Physician visits in the United States for constipation: 1958 to 1986. Dig Dis Sci. 1989;34:606–611 ___________________________________ ___________________________________ ___________________________________ • The prevalence of chronic constipation rises with age (above 65) • In this older age group, approximately 26 percent of men and 34 percent of women complain of constipation ___________________________________ ___________________________________ ___________________________________ • Talley, NJ, Fleming, KC, Evans, JM, et al. Constipation in an elderly community: A study of prevalence and potential risk factors. Am J Gastroenterol 1996; 91:19. • Talley, NJ, O'Keefe, EA, Zinsmeister, AR, Melton, LJ III. Prevalence of gastrointestinal symptoms in the elderly: A population-based study. Gastroenterology 1992; 102:895. ___________________________________ The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 2 26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society ___________________________________ Definition ___________________________________ • Each patient has there own definition of ___________________________________ • ___________________________________ • • • constipation Hard stool, discomfort, reduced frequency of defecation, etc Many patients denote a change in their frequency is termed “constipation” Historically constipation has been interpreted as stool frequency as little as 3 times per week Constipation is a symptom complex and not a disease ___________________________________ ___________________________________ ___________________________________ ___________________________________ Etiology ___________________________________ ___________________________________ • Causative or contributing factors are numerous - Neurogenic/Non-neurogenic ___________________________________ - Drug Induced ___________________________________ - Functional - Mechanical Obstruction ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ • Idiopathic causes as well - normal colonic transit ___________________________________ - slow transit ___________________________________ - dyssynergia (PFD) ___________________________________ ___________________________________ The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 3 26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society ___________________________________ Neurogenic Causes ___________________________________ ___________________________________ • DM, autonomic neuropathy • Multiple sclerosis, Parkinson’s disease, SCI ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Non-Neurogenic Causes ___________________________________ ___________________________________ • Hypothyroidism • Hypokalemia • Hypomagnesaemia ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Drugs ___________________________________ ___________________________________ • Definitely a contributing factor • Can pose a very challenging dilemma; what to stop, ___________________________________ when to stop, etc ___________________________________ ___________________________________ ___________________________________ The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 4 26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society ___________________________________ Drugs - Prescription ___________________________________ • • • • • • • Opiates Anticholinergics Antihistamines Antipsychotics TCA Calcium Channel Blockers Anti Parkinson Agents ___________________________________ • Locke GR 3rd, Pemberton JH, Phillips SF. AGA technical review on constipation. American Gastroenterological Association. Gastroenterology. 2000;119:1766–1778 ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Drugs – Nonprescription • • • • Calcium-containing antacids • Locke GR 3rd, Pemberton JH, Phillips SF. AGA technical review on constipation. American Gastroenterological Association. Gastroenterology. 2000;119:1766–1778 ___________________________________ ___________________________________ Calcium supplements ___________________________________ Iron supplements Anti-diarrheal agents ___________________________________ ___________________________________ ___________________________________ ___________________________________ Clinical Evaluation ___________________________________ • Excellent history ___________________________________ - review of prescribed/non-prescribed drugs - frequency of defecation - character of stool - physical complaints/concerns - level of inactivity - accessibility to proper facilities - psychosocial assessment - consider “bowel function diary” ___________________________________ ___________________________________ ___________________________________ ___________________________________ The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 5 26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society ___________________________________ Clinical Evaluation ___________________________________ ___________________________________ • Degree of straining (? Incomplete evacuation; possible PF disorder) ___________________________________ • Assess need or requirement for manual pressure or disimpaction ___________________________________ • What methods of therapy have or are presently being employed ___________________________________ • Ignoring the urge to defecate ___________________________________ ___________________________________ Physical Examination ___________________________________ ___________________________________ • Assessment of rectal tone • Quality of stool in rectal vault • Rule out distal obstructing lesion ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ http://gastrolab.1g.fi/ja/a025/slides/5.jpg The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 6 26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society ___________________________________ Diagnostic Testing ___________________________________ ___________________________________ • Electrolytes • TSH ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Diagnostic Testing ___________________________________ • ? Colonoscopy recommended only for patients ___________________________________ • General agreement that that all constipated ___________________________________ displaying evidence of mechanical obstruction patients >50yrs of age should undergo CRC screening ___________________________________ • Each case is patient & physician dependent • ___________________________________ ___________________________________ Brenner, DM. Chronic Constipation in 2006: Where we have been, where are we going. The Gastroenterology Report, 2006;1:4-10. ___________________________________ “Red Flags” ___________________________________ • New onset constipation in the elderly • Severe persistent constipation that is ___________________________________ • • • • ___________________________________ • • unresponsive to empiric treatment Hematochezia FOBT (+) Unexplained anemia Weight loss of 10lbs or more ___________________________________ ___________________________________ Cash BD. Fresh perspectives in chronic constipation and other functional bowel disorders. Rev Gastroenterol Disord - 01-JUL-2007; 7(3): 116-33 ___________________________________ Brandt LJ, Prather CM, Quigleu EM, et al. Systematic review on the management of chronic constipation in North America. Am J Gastroenterol. 2005:100 (suppl 1):S5-S21. The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 7 26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society ___________________________________ Diagnostic Testing • • • • ___________________________________ Colonic Transit Studies ___________________________________ Balloon Expulsion ___________________________________ Anorectal Manometry ___________________________________ Defecography ___________________________________ ___________________________________ ___________________________________ Evacuation Disorders ___________________________________ ___________________________________ • What are some other causes? ___________________________________ • Rectocele • Foreign devices • Postsurgical changes ___________________________________ ___________________________________ ___________________________________ ___________________________________ Treatment Options ___________________________________ ___________________________________ • Evaluating & treating potentially causative factors - excluding/treat mechanical obstruction ___________________________________ - discontinuation of medications possibly precipitating constipation ___________________________________ - dietary/lifestyle modification ___________________________________ - addressing psychosocial issues - pharmacotherapy ___________________________________ The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 8 26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society ___________________________________ Treatment Options ___________________________________ ___________________________________ • Biofeedback therapy • Surgical options ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Mechanical Obstruction ___________________________________ ___________________________________ • Colorectal Cancer • Stricture • Solitary Rectal Ulcer Syndrome (SRUS) ___________________________________ ___________________________________ • Manual disimpaction/fragmentation if indicated ___________________________________ ___________________________________ ___________________________________ Impaction ___________________________________ • Can use mineral oil enema to soften stool • Water soluble contrast enema (Gastrograffin) to ___________________________________ exclude proximal obstruction and to eliminate more proximal impactions • ? Endoscopic disimpaction • After disimpaction continue with daily enemas or oral laxative solution to ensure colon gets completely evacuated • ___________________________________ ___________________________________ ___________________________________ ___________________________________ Ward, A. Treatment of constipation in adults. UpToDate Online 17.2 The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 9 26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society ___________________________________ Impaction ___________________________________ ___________________________________ • Patient should then be on daily bowel regimen to try and promote daily bowel movements ___________________________________ • Should use restroom after meals to try and take advantage of natural gastrocolic reflex ___________________________________ ___________________________________ ___________________________________ ___________________________________ Dietary Changes ___________________________________ ___________________________________ • Dietary fiber and bulk laxatives such as psyllium or methylcellulose, together with adequate fluids, are the most physiologic and effective approach to therapy, improving bowel habits in many patients with constipation • Wheat bran is one of the more effective fiber laxatives. • ___________________________________ ___________________________________ ___________________________________ Floch, MH, Wald, A. Clinical evaluation and treatment of constipation. Gastroenterologist 1994; 2:50. ___________________________________ ___________________________________ ___________________________________ • High fiber diet increases stool weight and decreases ___________________________________ • Caution patients that consuming large amounts of ___________________________________ (***from colonic bacterial fermentation***) ___________________________________ colon transit time by stimulating intestinal muscles fiber can cause abdominal bloating, flatulence –why?? • Recommended daily intake ~25 grams ___________________________________ ___________________________________ The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 10 26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society ___________________________________ Bulk Forming Laxatives ___________________________________ • Psyllium, methylcellulose, calcium polycarbophil • Natural or synthetic polysaccharides or cellulose ___________________________________ derivatives that primarily exert their laxative effect by absorbing water and increasing fecal mass • These laxatives are effective in increasing the frequency and softening the consistency of stool with a minimum of adverse effects ___________________________________ • ___________________________________ ___________________________________ ___________________________________ Ward, A. Treatment of constipation in adults. UpToDate Online 17.2 ___________________________________ Bulk Forming Laxatives ___________________________________ ___________________________________ • ? Clear benefit • Most agree that a trial is reasonable ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Laxatives • • • • ___________________________________ Osmotic ___________________________________ Stimulant ___________________________________ Saline ___________________________________ Stool Softeners ___________________________________ ___________________________________ http://www.clinicaladvisor.com/fda-approves-linzess-for-ibs-chronic-constipation/article/256919/# The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 11 26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society ___________________________________ Osmotic Laxatives ___________________________________ • Miralax (PEG 3350) ___________________________________ 17grams (1 tblspn) in 8oz water daily • Lactulose 15-30ml daily up to TID ___________________________________ ___________________________________ • Sorbitol 15-30ml BID ___________________________________ Peura DA. PDR Clinical Handbook: chronic Constipation 1st ed. Montvale, NJ: Thomson PDR; 2007 Brandt LJ, Prather CM, Quigleu EM, et al. Systematic review on the management of chronic constipation in North America. Am J Gastroenterol. 2005:100 (suppl 1):S5-S21. Ramkumar D, Rao SSC. Efficacy and safety of traditional medical therapies for chronic constipation: systemic review. Am J Gastroenterol. 2005;100:936-971 ___________________________________ ___________________________________ Osmotic Laxatives ___________________________________ ___________________________________ • Poorly absorbed substances draw water into the lumen of the bowel from the surrounding tissue along an osmotic gradient. ___________________________________ • This maintains isotonicity with serum plasma, ___________________________________ resulting in increased bulk and a softer stool. • ___________________________________ Brenner, DM. Chronic Constipation in 2006: Where we have been, where are we going. The Gastroenterology Report, 2006;1:4-10 ___________________________________ ___________________________________ Osmotic Laxatives ___________________________________ ___________________________________ • SE: - diarrhea ___________________________________ - electrolyte disturbances (K, Na) ___________________________________ PEG does not cause bloating, gas ___________________________________ ___________________________________ The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 12 26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society ___________________________________ Saline Laxative (also osmotic) ___________________________________ ___________________________________ • Magnesium hydroxide (MOM) 1-2 tblspn daily or BID ___________________________________ Magnesium Citrate ___________________________________ - onset .5-6hrs ___________________________________ ___________________________________ Peura DA. PDR Clinical Handbook: chronic Constipation 1st ed. Montvale, NJ: Thomson PDR; 2007 ___________________________________ Stimulant Laxatives ___________________________________ • Senna (Sennokot) ___________________________________ 2 tablets daily up to 4 tablets BID - also in Smooth Move Tea® - Swiss Kriss® • Bisacodyl (Dulcolax) 5-15mg daily (po or pr) ___________________________________ ___________________________________ stimulate sensory nerves within the colonic mucosa and result in increased motility • Peura DA. PDR Clinical Handbook: chronic Constipation 1st ed. Montvale, NJ: Thomson PDR; 2007 • Brandt LJ, Prather CM, Quigleu EM, et al. Systematic review on the management of chronic constipation in North America. Am J Gastroenterol. 2005:100 (suppl 1):S5-S21. • Brenner, DM. Chronic Constipation in 2006: Where we have been, where are we going. The Gastroenterology Report, 2006;1:4-10. ___________________________________ ___________________________________ ___________________________________ Stimulant Laxatives ___________________________________ ___________________________________ • ? Efficacy • SE: cramping, diarrhea, hepatotoxicity, electrolyte ___________________________________ imbalances • ? Enteric nerve damage with subsequent dilation of the colon and poor motility ___________________________________ • Melanosis coli (senna & cascara – anthraquinonecontaining compounds) ___________________________________ Brenner, DM. Chronic Constipation in 2006: Where we have been, where are we going. The Gastroenterology Report, 2006;1:4-10. • Brandt LJ, Prather CM, Quigleu EM, et al. Systematic review on the management of chronic constipation in North America. Am J Gastroenterol. 2005:100 (suppl 1):S5-S21. • Xing JH, Soffer E. Adverse effects of laxatives. Dis Colon Rectum. 2001;44:1201–1209. • Muller-Lissner SA, Kamm MA, Scarpignato C, Wald A. Myths and misconceptions about chronic constipation. Am J Gastroenterol. 2005;100:232–242. ___________________________________ The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 13 26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ http://www.gastrohep.com/images_pdfs/images/medium/oepstein.jpg ___________________________________ Stimulant Laxatives ___________________________________ ___________________________________ • Some individuals can develop a pyschosocial dependency on stimulant laxatives ___________________________________ • ? Myenteric nerve damage - ? Neurogenic colon ___________________________________ • Cash BD. Fresh perspectives in chronic constipation and other functional bowel disorders. Rev Gastroenterol Disord - 01-JUL-2007; 7(3): 116-33 • Muller-Lissner SA, Kamm MA, Scarpignato C, Wald A. Myths and misconceptions about chronic constipation. Am J Gastroenterol. 2005;100:232-242. ___________________________________ ___________________________________ ___________________________________ Stool Softeners ___________________________________ • Docusate sodium (Colace ) ___________________________________ © 100mg BID - detergents that lower surface tension of the stool which causes an increase in water content of the stool & softens it - minimal SE - ? Benefit - effect in 1-3 days • • ___________________________________ ___________________________________ ___________________________________ Peura DA. PDR Clinical Handbook: chronic Constipation 1st ed. Montvale, NJ: Thomson PDR; 2007 ___________________________________ Brenner, DM. Chronic Constipation in 2006: Where we have been, where are we going. The Gastroenterology Report, 2006;1:4-10. The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 14 26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society ___________________________________ Enemas, Suppositories & Lubricants ___________________________________ ___________________________________ • Mineral oil, tap water, glycerin, bisacodyl ___________________________________ • Peura DA. PDR Clinical Handbook: chronic Constipation 1st ed. Montvale, NJ: Thomson PDR; 2007 ___________________________________ ___________________________________ ___________________________________ ___________________________________ Chloride Channel Activator ___________________________________ ___________________________________ • Lubiprostone (Amitiza ) © 24 mcg BID with food ___________________________________ • Derived from a metabolite of prostaglandin E1 although it has no effects on smooth muscle contraction ___________________________________ ___________________________________ Peura DA. PDR Clinical Handbook: chronic Constipation 1st ed. Montvale, NJ: Thomson PDR; 2007 • ___________________________________ Cash BD. Fresh perspectives in chronic constipation and other functional bowel disorders. Rev Gastroenterol Disord - 01-JUL-2007; 7(3): 116-33 ___________________________________ Chloride Channel Activator ___________________________________ ___________________________________ • Type 2 chloride channel (CIC-2) present in luminal membrane • Potential to increase chloride and fluid secretion into lumen • When activated, chloride and sodium get secreted into lumen with water passively following to maintain isotonicity. • Adds fluid to stool and promotes increased transit • ___________________________________ ___________________________________ ___________________________________ ___________________________________ Cash BD. Fresh perspectives in chronic constipation and other functional bowel disorders. Rev Gastroenterol Disord - 01-JUL-2007; 7(3): 116-33 The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 15 26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society ___________________________________ Linzess (linactolide) © • • • • ___________________________________ Guanylate cyclase-C agonist ___________________________________ 145mg/day for CIC ___________________________________ 290mg/day for IBS-C ___________________________________ Subsequent elevation in intracellular cGAMP stimulates secretion of chloride and bicarbonate ions into intestinal lumen ___________________________________ ___________________________________ http://www.frx.com/pi/linzess_pi.pdf ___________________________________ Opioid Antagonists ___________________________________ ___________________________________ • Methylnaltrexone ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Methylnaltrexone ___________________________________ • Relistor • Functions as a peripherally-acting mu-opioid ___________________________________ © receptor antagonist in tissues such as the gastrointestinal tract, thereby decreasing the constipating effects of opioids without impacting opioid-mediated analgesic effects on the central nervous system. • Administered subcutaneously ___________________________________ • ___________________________________ ___________________________________ ___________________________________ "Relistor Full Prescribing Information". http://www.wyeth.com/content/showlabeling.asp?id=499. Retrieved 2009-05-09 The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 16 26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society ___________________________________ Biofeedback Therapy ___________________________________ • Used to correct inappropriate contraction of the pelvic ___________________________________ floor muscles and EAS used during defecation • Using anal electromyography or sphincter recording pressures • Focuses on retraining, relaxation of sphincter and pelvic floor muscles • May be effective in more than 70% of patients with dyssynergic defecation • Wald A. Chronic constipation:a guide to modern management.Gastroenterology & Endoscopy News Special Edition.2007:89-96. • Cheung O, Wald A. Review article: the management of pelvic floor disorders. Ailment Pharmacol Ther. 2004;19:481-495. ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Surgery ___________________________________ ___________________________________ • Colectomy with IR anastomosis - for slow transit constipation • Repair of rectocele? • Bloating and abdominal pain are less likely to improve with surgery. ___________________________________ ___________________________________ ___________________________________ • Wald A. Chronic constipation:a guide to modern management.Gastroenterology & Endoscopy News Special Edition.2007:89-96. • Knowles CH, Scott M, Lunniss PJ. Outcome of colectomy for slow transit constipation. Ann Surg. 1999;230:627-638. ___________________________________ ___________________________________ Complications from Constipation • • • • • • ___________________________________ Stercoral Ulcer ___________________________________ Perforation ___________________________________ Fecal Impaction/Obstruction ___________________________________ Hemorrhoids Anal Fissures ___________________________________ Prolapse ___________________________________ The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 17 26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society ___________________________________ ___________________________________ ___________________________________ Clostridium difficile ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Basics ___________________________________ ___________________________________ • What is Cdiff? • Gram + • Anaerobe • Spore forming bacillus (spores can live awhile ___________________________________ ___________________________________ outside the human body) ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ • Produces two exotoxins • Responsible for up to 15-25% of all antibiotic associated diarrheas, 50% to 75% of those with antibiotic-associated colitis, and more than 90% of those with antibiotic-associated pseudomembranous colitis ___________________________________ • Important hospital-acquired infection associated ___________________________________ ___________________________________ with an increase in length of hospital stay and cost, and substantial morbidity and mortality. ___________________________________ The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 18 26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society ___________________________________ Basics ___________________________________ ___________________________________ • Spores survive gastric acidity • In small intestine, spores convert into their vegetative ___________________________________ state • In the colon, normal flora has been disrupted by Abx ___________________________________ and spores germinate and flourish ___________________________________ ___________________________________ ___________________________________ What can it do?? • • • • • ___________________________________ pseudomembranous colitis (PMC) ___________________________________ toxic megacolon ___________________________________ perforations of the colon ___________________________________ sepsis death (rarely) ___________________________________ ___________________________________ ___________________________________ Symptoms • • • • • ___________________________________ watery diarrhea ___________________________________ fever ___________________________________ loss of appetite ___________________________________ nausea abdominal pain/tenderness ___________________________________ ___________________________________ The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 19 26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society ___________________________________ Risk factors • • • • • • • ___________________________________ ___________________________________ antibiotic exposure proton pump inhibitors ___________________________________ gastrointestinal surgery/manipulation long length of stay in healthcare settings ___________________________________ a serious underlying illness ___________________________________ immunocompromising conditions advanced age ___________________________________ ___________________________________ Is it there? Is active? ___________________________________ ___________________________________ • Clostridium difficile colonization • patient exhibits NO clinical symptoms • patient tests positive for Clostridium difficile organism and/or its ___________________________________ toxin • more common than Clostridium difficile infection • Studies show that colonization in LTCF can be up to 20%!! ___________________________________ ___________________________________ • Clostridium difficile infection • patient exhibits clinical symptoms • patient tests positive for the Clostridium difficile organism and/or its ___________________________________ toxin ___________________________________ How did I get this??? ___________________________________ ___________________________________ • Shed in feces • Any device contaminated with feces can transmit it • Clostridium difficile spores are transferred to patients mainly ___________________________________ via the hands of healthcare personnel who have touched a contaminated surface or item ___________________________________ • The estimated prevalence of C. difficile colonization may be ___________________________________ as high as 50% in hospitalized patients where CDI is endemic, 5% to 7% in residents of long-term care facilities, and generally less than 2% in ambulatory adults. ___________________________________ The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 20 26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/infectious-disease/clostridium-difficile-infection/ ___________________________________ ___________________________________ • The 1st step is alteration of the normal gut flora, usually as a ___________________________________ • Clindamycin was the first antibiotic to be associated with ___________________________________ • Since that initial observation, almost all antimicrobials have ___________________________________ • Chemotherapeutic agents, particularly those with antimicrobial ___________________________________ result of administration of an antibiotic. pseudomembranous colitis, identified as a precipitant before the establishment of C. difficile as the causal pathogen. been associated with CDI including cephalosporins, penicillins, and the fluoroquinolones. properties, have also been associated with the development of CDI ___________________________________ http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/infectious-disease/clostridium-difficile-infection/ ___________________________________ ___________________________________ ___________________________________ • The second step is acquisition of a toxigenic strain of C. difficile. • The organism is primarily a nosocomially acquired pathogen ___________________________________ and its spores can be found in the hospital environment • Once a patient has acquired C. difficile, he or she will develop clinical disease or will remain asymptomatically colonized, the final step in the process. ___________________________________ • Although the exact incubation time for CDI is unknown, the ___________________________________ time from acquisition to disease is relatively short, perhaps no longer than 7 days ___________________________________ The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 21 26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society ___________________________________ Treatment ___________________________________ ___________________________________ • In about 20% of patients, Clostridium difficile infection will resolve within 2-3 days of discontinuing the antibiotic to which the patient was previously exposed. ___________________________________ • The infection can usually be treated with an appropriate course (about 10-14 days) of antibiotics, including metronidazole, vancomycin (administered orally), or recently approved fidaxomicin. ___________________________________ ___________________________________ • After treatment, repeat Clostridium difficile testing is not recommended if the patients’ symptoms have resolved, as patients may remain colonized ___________________________________ ___________________________________ How can we prevent this ___________________________________ ___________________________________ • Use antibiotics judiciously (are they truly necessary?) • Use Contact Precautions: for patients with known or suspected ___________________________________ Clostridium difficile infection; can stop when diarrhea ceases • Because alcohol does not kill Clostridium difficile spores, use of soap and water is more efficacious than alcohol-based hand rubs. • Use gowns when entering patients’ rooms and during patient care. • Dedicate or perform cleaning of any shared medical equipment ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ • Continue these precautions until diarrhea ceases. • Because Clostridium difficile-infected patients continue to ___________________________________ shed organism for a number of days following cessation of diarrhea, some institutions routinely continue isolation for either several days beyond symptom resolution or until discharge, depending upon the type of setting and average length of stay. ___________________________________ ___________________________________ • Cleansing programs at institutions ___________________________________ The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 22 26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society ___________________________________ Diagnosis ___________________________________ ___________________________________ • Stool analysis: PCR (highly specific and sensitive) • What about sigmoidoscopy or colonoscopy? ___________________________________ • When should this be done?? ___________________________________ ___________________________________ ___________________________________ ___________________________________ Endoscopic view…. ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ http://www.langetextbooks.com/0071774343/gallery.php?id=o-p ___________________________________ Treatment ___________________________________ ___________________________________ • Historically, as many as 50% of patients will respond to stopping the precipitating antibiotic, however the emerging trends of CDI demonstrate that this is a potentially devastating infection that requires treatment. ___________________________________ ___________________________________ • Adequate hydration and electrolyte replenishment should accompany medical and surgical therapy. ___________________________________ • Antiperistaltics should be avoided because these can exacerbate toxin-mediated damage to the mucosa. ___________________________________ The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 23 26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society ___________________________________ Treatment ___________________________________ ___________________________________ • Metronidazole (500mg 1 po TID or IV for 2 weeks) • Effective, comparable to vancomycin but less expensive ___________________________________ (and less chance of developing VRE!) • Oral vanco used for intolerance to metronidazole, lack of ___________________________________ response to metronidazole or more severe disease • No documented resistance to these two drug by Cdiff ___________________________________ • When should we start seeing results?? ___________________________________ • Hopefully by a few days ___________________________________ Treatment ___________________________________ ___________________________________ • Severe disease • Can use vanco enemas ___________________________________ • May need surgical eval ___________________________________ ___________________________________ ___________________________________ ___________________________________ Treatment • • • • ___________________________________ IVIG ___________________________________ Probiotics ___________________________________ Fidaxomicin (Dificid) ___________________________________ Rifaximin: Small case series have suggested that sequential therapy with vancomycin followed by rifaximin may be effective for the treatment of recurrent CDI [ ___________________________________ ___________________________________ The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 24 26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society ___________________________________ Recurrence ___________________________________ ___________________________________ • 20%after 1st episode • 45% after 1st recurrence • 65% after 2 or more recurrences ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Recurrence ___________________________________ ___________________________________ • Historically, we are taught to give another trial of what we first tried ___________________________________ • CDI can recur after treatment with metronidazole or vancomycin with rates ranging from 15% to 30% ___________________________________ • After the first relapse; prolonged vanco taper is recommended ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 25 26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society ___________________________________ Fecal Transplant ___________________________________ ___________________________________ • Fecal bacteriotherapy • Attempts to reconstitute the protective flora with ___________________________________ fecal infusions via nasogastric tube or rectally have been reported to have great success ___________________________________ ___________________________________ ___________________________________ http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/infectious-disease/clostridium-difficile-infection/ ___________________________________ Toxic Megacolon ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ http://graphicwitness.medicalillustration.com/generateexhibit.php?ID=69184 ___________________________________ Toxic Megacolon ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ http://o.quizlet.com/4.GEfAuLHm7ncGlt1lG1lg_m.png The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 26 26th Annual Fall Symposium – New Frontiers in Geriatrics - Arizona Geriatrics Society ___________________________________ Surgery ___________________________________ ___________________________________ • Early surgical consultation should be considered for severe CDI, especially if toxic megacolon is present, because operative intervention can be lifesaving. ___________________________________ • Various surgical procedures have been described, ___________________________________ including diversion of fecal stream by ileostomy, decompressive colostomy, or subtotal colectomy, the procedure of choice with toxic megacolon. ___________________________________ • Cases requiring surgery carry high mortality rates, ranging from 30% to over 50% ___________________________________ http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/infectious-disease/clostridium-difficile-infection/ ___________________________________ ___________________________________ ___________________________________ Thank You ___________________________________ ___________________________________ ___________________________________ ___________________________________ The information in this document may not be reproduced or disclosed to unauthorized parties without the prior consent of the Arizona Geriatrics Society. 2014 Arizona Geriatrics Society All Rights Reserved 27
 0
0

No more boring flashcards learning!
Learn languages, math, history, economics, chemistry and more with free StudyLib Extension!
- Distribute all flashcards reviewing into small sessions
- Get inspired with a daily photo
- Import sets from Anki, Quizlet, etc
- Add Active Recall to your learning and get higher grades!
Related documents
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users