Examination of the Shoulder Complex
advertisement

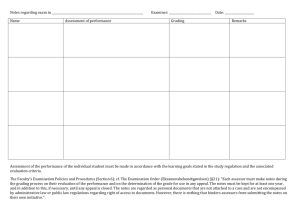
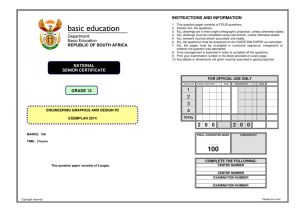
Examination of the Shoulder Complex RICHARD W. BOWLING, PAUL A. ROCKAR, JR., and RICHARD ERHARD This article presents a protocol for the examination of the shoulder complex. The examination is divided into subjective and objective components. A primary focus of this article is on the functional portion of the objective examination and its interpretation. The functional examination consists of active and passive rangeof-motion tests, accessory mobility tests, resisted tests, and palpation. This approach enables the examiner to classify movement disorders of the shoulder complex into dysfunctions of the noncontractile tissues and of the contractile tissues. Factors that enable the examiner to determine the severity of a pathological condition or to identify stages of the healing process are discussed. This information will assist the physical therapist in establishing treatment goals and in selecting appropriate strategies of therapeutic intervention. Key Words: Physical therapy, Shoulder, Shoulder joint. The ability of a physical therapist to manage successfully problems involving the shoulder complex depends on an understanding of functional anatomy, pathokinesiology, principles of examination, and principles of treatment of the musculoskeletal system. The purpose of this article is to present a protocol for the examination of the shoulder region. The primary focus is on those components of the subjective and objective examinations that we believe are most important to the physical therapist. Much of what we will describe is based on the original work of Cyriax,1 and we feel compelled to acknowledge his contribution to orthopedic medicine. The objective of the examination of any part of the musculoskeletal system is to obtain data on which to base decisions regarding management. The naming of a disease process or specific injury often is overemphasized and can be in- Mr. Bowling is Assistant Professor, Department of Physical Therapy, School of Health Related Professions, University of Pittsburgh, Pittsburgh, PA 15261 (USA), and is in private practice at Forest Hills Orthopaedic and Sports Physical Therapy Associates, Inc, 2372 Ardmore Blvd, Pittsburgh, PA 15221. Mr. Rockar is Adjunct Assistant Professor, Department of Physical Therapy, School of Health Related Professions, University of Pittsburgh, and is in private practice at Forest Hills Orthopaedic and Sports Physical Therapy Associates, Inc. Dr. Erhard is Assistant Professor, Department of Physical Therapy, School of Health Related Professions, University of Pittsburgh and is in private practice at 7 N Washington St, Masontown, PA 15461. 1866 adequate because individuals with the same diagnosis may require different treatment. Movement dysfunctions may be classified logically into syndromes or clusters of signs and symptoms revealed by a thorough and systematic examination. Such information is useful in determining the severity of a client's pathological condition or in identifying stages of the healing process. We must emphasize that the examination process is continuous. As an individual's condition progresses, or regresses, the signs and symptoms will alter, therefore dictating changes in management of the problem. SCREENING EXAMINATION One of the primary problems encountered by clinicians when dealing with clients who complain of upper extremity pain is localization of the disorder to a specific region or structure. We have adopted and modified a screening examination procedure developed by Cyriax.1 This procedure is designed to localize rapidly the area or areas of involvement and is outlined in Appendix 1. The screening examination is performed in a manner that allows a considerable amount of information to be gathered in a brief timespan. All resisted tests are performed after the individual has completed his available range of motion. Resistance, thus, is applied with the muscle group tested in a shortened position and the joint at the limit of motion. For example, when resisted ab- duction of the shoulder is being tested, the client is instructed to abduct his arm as far as possible and maintain this position as the examiner attempts to force the arm downward. This procedure enables the examiner to gain information about the client's neuromuscular system, as well as his ROM. Because the resisted tests are performed at the limit of the ROM, both contractile and noncontractile tissues may be stressed and reproduce symptoms. We emphasize, therefore, that the screening examination indicates only the area of involvement and not a specific lesion or structure. The screening examination is designed only to differentiate a shoulder problem from a problem in the cervical spine or elbow complex; further information about the dysfunction will be obtained from the specific examinations of the involved area. Information gathered from the screening examination will indicate whether a specific examination is needed of the cervical spine, shoulder complex, elbow complex, the wrist and hand or more than one of these areas. If one or more of the following findings are present, a specific examination of the shoulder complex is indicated: 1) observable postural abnormality of the shoulder girdle or glenohumeral joint; 2) deformity or wound in the area; 3) abnormal response to active elevation of the upper limb; 4) weakness, pain, or limited ROM on resisted shoulder-girdle elevation; 5) weakness, pain, or limited ROM on resisted glenohumeral joint PHYSICAL THERAPY abduction; and 6) pain on resisted flexion or extension of the elbow joint that is localized to the shoulder region. If no movement or resisted test in the screening examination reproduces or exacerbates the symptoms of nonathletic clients, the examiner must be suspicious of pain referral from sources other than the musculoskeletal system, such as an inflammation of the gall bladder or heart disease.2 Athletes' symptoms often are reproduced only by the application of stresses far greater than those applied during the screening examination. SPECIFIC EXAMINATIONS OF THE SHOULDER COMPLEX The examination protocol that is explained below for the shoulder complex is outlined in Appendix 2. Subjective Examination The objective of the subjective examination is to determine 1) the possible source or sources of the client's complaint, 2) the nature of the complaint, and 3) the severity and stage of the condition. This information is important in planning the objective portion of the examination; that is, the client's responses to specific questions will determine which components of the functional examination should receive emphasis and whether the examination movements will be performed cautiously or vigorously. Most clients, when asked why they consulted a physician, state that the reason was pain, inability to perform a particular functional activity, or both. If the primary problem is pain, its present location must be determined. The location of the pain will provide the examiner with information regarding the source of the problem. The glenohumeral joint and its associated soft tissues, for example, may refer pain into the C5 dermatome. Other joints or structures that refer pain into or that are located in this area may be excluded by a negative response on the screening examination. The examiner, however, must be aware that coexisting problems are common. For example, degenerative joint disease of the cervical spine may refer pain into this area. This condition occurs in the same age group in which an impingement syndrome of the glenohumeral joint may occur. The sternoclavicular and acromioclavicular joints, however, may generate local Volume 66 / Number 12, December 1986 symptoms. The classical example is the athlete who points directly to the acromioclavicular joint as the source of his pain. After the location of the present pain has been determined, the client will be asked whether the pain location has changed since the onset of the problem or whether the pain location changes during the course of the day or with particular movements or activities. If the pain location has changed since the onset of the problem, the pain likely will have spread down the arm into the more distal region of the C5 dermatome, or it will have receded into a more proximal zone of the dermatome. Pain that has spread distally indicates that the problem is worsening, whereas receding pain indicates that the problem is less severe. Proximal pain that expands into the distal portion of the C5 dermatome during the performance of a particular movement or activity also indicates the presence of acute inflammation. Determining the duration of pain is important for providing information about the irritability of the condition and should guide the application of testing movements during the objective examination. If the pain is provoked easily by a light movement or activity and remains for a prolonged period of time, the examination movements should be performed cautiously to avoid exacerbating the condition. If considerable stress is required to elicit pain, however, the examination movements probably should be performed vigorously.3 The examiner also must determine whether the pain is constant or intermittent. If the pain is constant, it may be caused by a nonmechanical disorder, such as a malignancy. Alternatively, constant pain may indicate a severely inflamed joint that may require immobilization. Intermittent pain usually indicates that the problem is mechanical. The pain, generally, is relieved by rest and aggravated by activity. If the pain persists or increases at rest, a serious pathological condition such as a malignancy or bacterial arthritis may be suspected, especially if the pain awakens the client from sleep. If the client's chief complaint is a loss of function, the examiner must determine the nature of the functional deficit. Such deficits may range from an inability to perform simple activities of daily living (eg, combing the hair, completing personal hygiene, reaching into the hip pocket, fastening a bra strap) to diffi- culty performing specific athletic activities (eg, throwing a baseball). Regardless of whether the client complains of pain, a loss of function, or both, the examiner must determine how the problem began. If trauma was associated with the onset of the problem, details of the event may be helpful in diagnosing the disorder and determining its cause. If no specific traumatic incidents can be recalled, the examiner then should consider certain types of activities or actions that may have precipitated the problem, such as overhead painting, occupations involving prolonged abduction (hairdressing), or a change in throwing motion in the athletic client. The examiner also must determine whether the client has problems with other joints, which may indicate a systemic disorder such as rheumatoid arthritis. If the client has undergone surgery at the shoulder or other locations, the nature of these procedures should be ascertained. Particular attention should be given to surgery or other treatment for a malignancy because of the likelihood that the client will have a metastatic tumor. Other systemic disorders such as diabetes mellitus are known to affect the shoulder joint. Clients with this disease are likely to have bilateral involvement and, therefore, to be recalcitrant to treatment. Objective Examination Inspection. The examiner observes the posture of the client's head, spine, and upper limb. It is important to determine whether the client has an increased upper thoracic kyphosis because this deformity may limit the range of upper limb elevation. This limited range of elevation is not caused primarily by joint restriction but rather by the altered starting position for sagittal plane motion of the glenohumeral joint. The altered starting position occurs because of the change in the resting position of the scapula (Figs. 1, 2). In younger clients, the examiner also may observe a concomitant increase of hyperextension of the glenohumeral joint. The contour of the shoulder region also is examined for obvious deformity such as that caused by dislocation of the glenohumeral joint or separation of the acromioclavicular joint. Atrophy of the deltoid, upper trapezius, supraspinatus, and infraspinatus muscles also should be noted. The client must be examined for any limitation of functional activity when being prepared for treatment. The 867 formed best in several planes because pain may occur in one plane and not in others. Assessment of active movement alone is not diagnostic because stress will be placed on both contractile and noncontractile tissues. The contractile tissues include muscles, tendons, and those of the tenoperiosteal junction.1 All other tissues are considered noncontractile. Although both types of tissue will be stressed with active movement, considerable information nevertheless will be provided to the careful observer. These data may be correlated with subsequent portions of the examination to determine the cause of the problem. To clarify this procedure, we will describe the clinical assessment of two distinctly dif- Fig. 1. Normal active elevation of the upper limb. skin is checked for wounds, surgical scars, contusions, or abrasions. The client's use of an assistive device also should be recorded. Functional examination. To the physical therapist, the functional examination is the most important component of the entire examination process. It consists of 1) examination of active movement, 2) examination of passive movement, 3) examination of accessory movement, 4) resisted tests, and 5) palpation.4 Active range of motion. The client's AROM is assessed to determine his willingness or ability to move the joint and, if the ROM is abnormal or painful, to establish a baseline for measuring the effectiveness of treatment. The movements examined actively at the shoulder include 1) elevation of the upper limb; 2) elevation, depression, protraction, and retraction of the shoulder girdle; and 3) flexion, extension, abduction, horizontal adduction, medial (internal) rotation, and lateral (external) rotation of the glenohumeral joint. The term elevation is used to denote the act of placing the upper limb in a vertical position or as near to this position as possible. The client performs this activity while the examiner records any deviation from the normal scapulohumeral rhythm. The movement of elevation may be accomplished in the frontal plane, the sagittal plane, or in the scapular plane. This movement is per1868 Fig. 2. Active elevation of the upper limb when increased thoracic kyphosis is present. Note the decreased range of motion compared with Figure 1. ferent problems. Excessive scapular elevation and upward rotation may occur in combination with limited active elevation of the upper limb in clients with adhesive capsulitis or a rotator cuff tear. Adhesive capsulitis is a lesion of the noncontractile tissues, whereas a rotator cuff tear involves the contractile tissues. In clients with adhesive capsulitis, passive movement of the glenohumeral joint also will be restricted, whereas the resisted tests will be normal. If a rotator cuff tear is present, the passive ROM will be normal, but the resisted tests will demonstrate weakness of the involved muscles. The interdependence of the active motion examination, the examination of passive movement, and resisted testing will be discussed further in subsequent sections of this article. Passive overpressure is the application of a passive stretch in the same direction as the active movement. We do not believe that it is appropriate to perform passive overpressure to convert the AROM test to a PROM test unless no pain is reported by the client. The PROM test, however, may be the most important component of the functional examination and should not be confined to that portion of the passive range available beyond active motion. Passive range of motion. Passive motion testing assesses the integrity of the noncontractile elements of a joint.1 Passive motion testing at the shoulder, as at any other joint of the musculoskeletal system, provides the examiner with a wealth of information. The same movements, with the addition of scapular distraction, that were performed in the examination of active movements also are performed passively (Figs. 3-14). While the client is performing the passive movements, the examiner must assess three factors: 1) ROM, 2) the nature of the motion barrier, and 3) the sequence of pain to the motion barrier.1 1. Range of motion. Range of motion may be excessive, normal, or limited. If the ROM is excessive, instability should be suspected. If the ROM is limited, if may be limited in either a capsular or a noncapsular pattern. The term capsular pattern was introduced by Cyriax to denote a total joint reaction to an inflammatory process (eg, arthritis).1 An inflammatory process has been shown to produce a reflex imbalance of the muscles that control the knee.5 Preliminary research by Dunn (J. S. Dunn, unpublished data, March 1980) leads us to believe that this muscle imbalance may involve any joint with facilitation of the physiological flexors (flexors, adductors, and medial rotators) and inhibition of the physiological extensors (extensors, abductors, and lateral rotators). This muscle imbalance results in a proportional limitation of movements of the joint. Each joint has a characteristic capsular pattern of restriction. The capsular pattern of the shoulder joint is such that the most restricted movement is lateral rotation followed by abduction and extension. The least restricted movements are medial rotation and adduction. PHYSICAL THERAPY Fig. 3. Passive elevation of the shoulder girdle. The shoulder girdle is moved passively in a cranial direction. Fig. 4. Passive depression of the shoulder girdle. The shoulder girdle is moved passively in a caudal direction. Fig. 5. Passive protraction of the shoulder girdle. The shoulder girdleismoved passively in an anterior direction. Fig. 7. Passive distraction of the scapulothoracic joint. The scapula is moved away from the thoracic wall. Fig. 6. Passive retraction of the shoulder girdle. The shoulder girdle is moved passively in a posterior direction. Although the concept of a capsular pattern has proven valuable in the diagnosis of disorders of the musculoskeletal system, the term itself has caused some confusion. The restriction may or may not be caused by a contracture of the joint capsule, and the presence of a capsular pattern may or may not be an indication for joint mobilization. In the acute stages of an inflammatory process, the pattern of restriction is produced and maintained by abnormal muscle tone, and the motion barrier at this time is muscle guarding. During the natural progression of the condition, a capsular contracture will occur. The capsular pattern then will be maintained by contracVolume 66 / Number 12, December 1986 ture of connective tissue, and the motion barrier will be capsular (Tab. 1). A capsular pattern is an indication of a joint inflammation or arthritis, and its most common cause is traumatic synovitis. If the client has no history of trauma, systemic diseases such as rheumatoid arthritis, psoriatic arthritis, and diabetes mellitus should be investigated with an appropriate examination. Interestingly, clients with diabetes mellitus often have bilateral involvement of the shoulders.6-7 Additionally, the restriction of medial rotation often is greater than the restriction that usually occurs in a capsular pattern (H. Tien, unpublished data, March 1978). Any restriction of motion that does not fit the capsular proportions is termed a noncapsular pattern.1 In contrast with the total joint involvement of the capsular pattern, noncapsular pat- Fig. 8. Passive flexion of the glenohumeral joint. Note that the examiner is stabilizing the scapula to prevent scapulothoracic movement. terns of restriction are caused by lesions that affect isolated portions of the joint or by extra-articular lesions. The most common cause of a noncapsular pattern of restriction of the shoulder is acute subdeltoid bursitis. When this condition is present, the client's ROM during glenohumeral abduction is disproportionately more limited than that occurring during lateral rotation. Cyriax and Cyriax have described other causes of a noncapsular pattern of restriction at the shoulder; however, these are uncommon.8 2. Nature of the motion barrier. As the client completes the passive movement being tested, the sensation im1869 TABLE 1 Correlation of Events in inflammatory Process with Clinical Examination Findings and Treatment of Synovial Joints Stage of Inflammation Early Intermediate Late constant felt at rest predominant feature distal reference zone before motion barrier intermittent felt during movement synchronous with motion barrier may become more intense and more distal with repeated forceful movement pain not severe only felt with forceful movement after motion barrier proximal extent of reference zone parted to the examiner's hands must be assessed. Cyriax has described motion barriers as different types of "end feel."1 He has identified the following types of sensation: 1) bone-to-bone, 2) capsular, 3) muscle guarding, 4) springy, 5) soft tissue-approximation, and 6) empty. A bone-to-bone motion barrier is caused by approximation of the bony members of a joint. This approximation causes the joint motion to come to an abrupt stop with no give on forced stretching. This type of barrier is not present on any movement of the shoulder under normal circumstances. It usually is caused by malalignment of fracture fragments of the proximal humerus. This malalignment results in impingement of the humerus against the acromion process of the scapula during abduction or flexion. Regardless of the cause, a finding of a bone-to-bone motion barrier is a contraindication to attempts at actively or passively increasing the ROM in the direction of the motion barrier. A capsular motion barrier is the normal end feel for most motions of the glenohumeral joint. Cyriax has described the capsular end feel as similar to the sensation imparted by stretching a piece of leather.1 This type of motion barrier is abnormal when it occurs prematurely in the ROM and generally is indicative of capsular contracture. When this type of motion barrier is present concurrently with a capsular pattern of limitation, it represents the late stage of adhesive capsulitis. The capsular nature of the motion barrier is an important factor in the differentiation of the late stage of this syndrome from the 1870 Range of Motion Pain Motion Barrier Treatment capsular pattern muscular (fast guarding) empty pain control modalities immobilization capsular pattern muscular (fastslow guarding) pain control gentle movement capsular pattern capsular vigorous mobilization exercise (automobilization) Fig. 9. Passive extension of the glenohumeral joint. The scapula is stabilized by the table. Fig. 10. Passive abduction of the glenohumeral joint. The examiner is stabilizing the scapula with the right hand. The scapula also can be stabilized by contacting the axillary border. acute and intermediate stages (Tab. 1). In the acute and intermediate stages, the motion barrier will be muscle guarding. Two types of muscle guarding occur. The "fast-guarding" type is characterized by sudden twinges of muscle activity as the joint is moved passively. Fast guarding may occur at any point in the ROM but becomes most severe as the terminal range is approached. The other type of muscular motion barrier is "slow guarding." Slow guarding usually occurs throughout the ROM and lacks the sudden twinges of fast guarding. A muscle that is too short may produce an end feel that is similar to a capsular motion barrier. If a muscle's length is insufficient to permit the attainment of a full PROM, the connective tissue components of the muscle will be stretched as the joint is moved. Another type of motion barrier that commonly affects the shoulder joint is the empty end feel. An empty end feel implies that no motion barrier was felt.1 This type usually occurs because severe pain prevents the client from attaining sufficient ROM to enable the examiner to sense a physical limitation to movement. This type of motion barrier typically occurs in clients with acute subdeltoid bursitis. The movement of glenohumeral abduction is limited by intense pain before the full range of abduction can be reached. We would expect muscle guarding to accompany this type of motion barrier, but it does not. We have observed marked subluxation of the glenohumeral joint on anteroposterior radiographs of clients with acute subdeltoid bursitis that did not occur after the condition had been rePHYSICAL THERAPY Fig. 13. Passive horizontal adduction of the glenohumeral joint. Fig. 11. Passive lateral rotation of the glenohumeral joint. Fig. 12. Passive medial rotation of the glenohumeral joint. solved. This inferior subluxation leads us to believe that the activity of the supraspinatus muscle is inhibited by the pain and may provide an explanation for the lack of muscle guarding. As stated previously, two other types of motion barriers are encountered. Soft tissue approximation may limit movement as opposing body surfaces come into contact. This type of end feel occurs commonly during knee flexion and elbow flexion. This motion barrier may occur in the shoulder with horizontal adduction as the anterior surface of the arm contacts the pectoral region of the chest. A springy motion barrier usually results from an internal derangement of the joint. It is common at the knee and elbow. The sensation that is imparted to the examiner's hand is that of a rebound Volume 66 / Number 12, December 1986 Fig. 14. Passive elevation of the upper limb. as the movement is forced through the last few degrees of the ROM. 3. Sequence of pain in relation to the motion barrier. The final factor to be considered in the examination of passive movement is the sequence of pain to the motion barrier. The client's experience of pain may be related temporally to the motion barrier in three ways1: It can occur 1) after the motion barrier has been met, 2) at the same time the motion barrier is met, or 3) before the motion barrier is met. Pain that occurs after the motion barrier has been met usually is caused by stretching contracted connective tissue. This is a common finding in the late stage of adhesive capsulitis. Pain that occurs concurrently with the motion barrier is indicative of a more acute lesion. It commonly occurs in the intermediate stage of adhesive capsulitis and usually is associated with an end feel of muscular guarding. Pain occurring before the motion barrier is met is indicative of an acute condition. Clients with such pain must be handled cautiously because the symptoms may be exacerbated by the examination. The motion barrier must be examined carefully to ensure that the pain is not the result of a painful arc. A painful arc usually occurs between 70 and 110 degrees of abduction as the greater tuberosity of the humerus is passing under the coracoacromial arch. Sensitive tissues located between these bony structures are compressed and produce pain. As the movement progresses and the greater tuberosity clears the coracoacromial arch, movement will become pain free. A painful arc usually is associated with the following disorders: 1) chronic subdeltoid bursitis, 2) supraspinatus tendinitis, 3) subscapularis tendinitis (upper portion of insertion), and 4) infraspinatus tendinitis.1 Cyriax also has described other, less common conditions that cause a painful arc at the shoulder.1 Examiners sometimes encounter athletic clients who complain of pain during the performance of a specific activity or event, but whose symptoms cannot be reproduced by PROM tests. The examiners also may be unable to reproduce these clients' symptoms with accessory movements or with resisted tests. Maitland has described two examination procedures—the quadrant and locking tests—that may be useful in the examination and treatment of these individuals.3 Accessory motion (mobility tests). The purpose of mobility testing is to examine the range of "joint play" or accessory movements.4,9 These procedures further assess the condition of the ligaments and capsule of the joint. The accessory motions that are examined at the shoulder complex are shown in Figures 15 through 23. The ROM of the accessory movements of the involved upper limb must be compared with that of the uninvolved contralateral limb. Examination of these movements may reveal normal, limited, or excessive ROM. Limited mobility indicates contracture of connective tissue, whereas excessive mobility indicates connective tissue laxity or rupture. The ROM of the accessory movements also must be correlated with the results of passive movement testing to determine the status of the joint. For example, a client may demonstrate a capsular pattern of limitation of the glenohumeral joint secondary to a recent anterior dislocation. After the reduction of the dislocation, the individual may have a capsular pattern of restriction associated with a muscle-guarding motion barrier. Accessory movements most likely will reveal excessive gliding (hypermobility) of the humeral head in both anterior and inferior directions. The client with a recent anterior dislocation may be compared with a client with a similar injury who is examined after reduction and a sufficient period 1871 Fig. 15. Superior glide of the medial clavicle. The medial end of the clavicle is moved in a cranial direction by the examiner's left hand. The examiner palpates the movement at the sternoclavicular joint with the right index finger. Fig. 18. Anterior glide of the medial clavicle. The medial end of the clavicle is pulled in an anterior direction by the examiner's left hand. The examiner palpates the movement at the sternoclavicular joint with the right index finger. Fig. 16. Inferior glide of the medial clavicle. The medial end of the clavicle is moved in a caudal direction by the examiner's right hand. The examiner palpates the movement at the sternoclavicular joint with the left index finger. Fig. 17. Posterior glide of the medial clavicle. The medial end of the clavicle is pushed in a posterior direction. Fig. 19. Hand placement for performance of anterior and posterior glide of the lateral clavicle on the acromion process. The distal end of the clavicle can be moved in an anterior and a posterior direction. Fig. 20. Distraction of the humeral head from the glenoid fossa. The examiner attempts to move the humeral head in a lateral direction. of immobilization. The period of immobilization may have allowed the damaged portion of the articular capsule to heal in a shortened position. Passive testing again may reveal a capsular pattern of restriction, but the motion barrier is most likely to be capsular, and the accessory movements are likely to be restricted. The clients, thus, must be treated quite differently even though they both exhibit a capsular pattern of restriction of passive movements after an anterior dislocation of the shoulder joint. Individuals with normal or excessive PROMs may demonstrate hypermobility on examination of passive movements. These clients must be questioned in detail concerning previous injuries of the shoulder joint. On close questioning, these clients often report a past traumatic episode. They may describe re- current episodes involving a "locking" sensation with a subsequent "clicking" during particular postures or movements. Such episodes may be indicative of an anteriorly subluxating glenohumeral joint, which, in contrast with a recurrent dislocating joint, often is difficult to diagnose. Special studies have been described in the literature that may be helpful in determining the cause of 1872 PHYSICAL THERAPY TABLE 2 Interpretation of Resisted Test Resultsa at Glenohumeral Joint for Common Contractile Lesions Resisted Test Muscle Deltoid Supraspinatus Infraspinatus Subscapularis Pectoralis major Teres minor Teres major Latissimus dorsib Biceps brachii Triceps brachii Abduction Adduction + ++ + + + + External Rotation Internal Rotation +/+/++ +/- Elbow Flexion Elbow Extension ++ + + +/- + + +/- ++ c + a Key: + = muscle performs function but rarely involved, + / - = muscle can produce pain with test but more painful with a different resisted test, ++ = muscle usually responsible for positive test results. b Also produces pain with resisted shoulder-girdle depression. c Many false negative test results. Fig. 21. Posterior glide of the humeral head, The examiner attempts to move the humeral head in a posterior direction. Fig. 22. Anterior glide of the humeral head. The examiner attempts to move the humeral head in an anterior direction. Fig. 23. Inferior glide of the humeral head. The examiner attempts to move the humeral head in an inferior direction. these problems, which appears to be an injury of the glenoid labrum.10 Resisted testing. Resisted tests are designed to stress the contractile tissues of a joint. The resisted tests performed at the shoulder complex are outlined in Appendix 2, and the resisted tests of the glenohumeral joint are depicted in Figures 24 through 29. Resisted tests in a specific examination of a joint are performed differently from the procedures described for the screening examination. In a specific examination, the resisted tests are performed in a mid-range or neutral position, in contrast with the end-range position that was used in the screening examination. The purpose of placing the joint in a neutral position is to eliminate any stress on the noncontractile tissues. When the patient performs an isometric contraction of a muscle group with the joint in this position, tensile stress is produced in the contractile tissues. If a painful condition involves the contractile tissues, the patient's symptoms will be reproduced with this maneuver. We must emphasize that the examiner is seeking replication of the client's symptoms. Although a test may produce slight pain, Volume 66 / Number 12, December 1986 the client will be able to distinguish it from the pain produced by his disorder, and it must not be interpreted by the examiner as a positive test result. The joint to be tested should be stabilized as much as possible. We generally place our clients in the supine position to achieve this stabilization. Theoretically, resisted testing of a muscle with an isometric contraction will produce pain only if a lesion is located within that muscle. In practice, difficulties sometimes arise that may lead to false positive test results. An isometric contraction of a muscle produces compressive stresses across the articular surfaces of the joint, in addition to shear stresses of the joint. Thus, acute inflammatory conditions around the joint may produce false positive resisted test results. Another source of error during resisted testing is a fracture near the insertion of the tested muscle, such as an avulsion fracture of the greater tuberosity. When administering resisted testing, we generally instruct the client to begin with a minimal contraction and gradually increase the resistance to elicit the symptoms of a painful condition. If the client begins with an initial contraction that is too strong, other muscles that also perform the movement may become involved. We have not found that standard muscle testing procedures are useful in the isolation of muscles that perform similar movements. Muscles that perform one movement often perform other movements at multiaxial joints, such as the shoulder, and this fact 1873 Fig. 25. Resisted glenohumeral adduction. The client resists the examiner's attempt to pull the elbow away from the side. Fig. 24. Resisted glenohumeral abduction. The client resists the examiner's attempt to force the elbow into the side. can be used to isolate the involved muscle after all resisted tests have been performed (Tab. 2). The problems associated with a painful resisted contraction can be minimized by careful performance of the procedures and by correlation of the test results with other portions of the examination. When false positive test results are produced by an acute inflammation of the joint, passive movements usually are more painful than the resisted tests. When false positive test results are produced by a fracture near the insertion of the tested muscle, the fracture usually is the result of a traumatic injury. When a client with a history of traumatic injury has positive resisted test results, therefore, the examiner must ensure that an adequate radiological examination has been performed. False negative test results also may occur. Pain that is reproduced by resisted elbow flexion indicates tendinitis of the long head of the biceps brachii muscle (Tab. 2). The occurrence of pain on this test, however, is uncommon. We do not believe that pain produced by elbow flexion always is symptomatic of bicipital tendinitis. We have found clinically that this test will produce positive results in only the most acute cases and that symptoms of bicipital tendinitis can be reproduced best by movement of the humerus in the sagittal plane. These 1874 symptoms can be reproduced either with activeflexionin the supine position or with active extension in the erect position. Resistance applied during flexion may be required to reproduce symptoms in less acute cases. Bicipital tendinitis can be confirmed by palpation for tenderness of the tendon. During the performance of resisted testing, the examiner should record whether the contraction elicits pain and also whether the contraction is strong or weak. Five patterns or possible combinations of strength and pain have been described by Cyriax.1 The test results may be 1) strong and painless, 2) strong and painful, 3) weak and painless, 4) weak and painful, or 5) all test results may be painful (Tab. 3). The classic positive finding for a contractile lesion or tendinitis is a strong, painful contraction on one or two resisted tests. The common tendinous inflammations at the shoulder complex involve the supraspinatus, infraspinatus, subscapularis, and long head of the biceps brachii muscles. Table 2 lists the specific resisted tests that are painful for each of these muscles. If the results are pain and weakness, a serious disorder may exist. At the shoulder complex, these findings may be produced by a recent tear of the rotator cuff, a fracture of one of the tuberosities of the humerus, or a neoplasm near the joint.1 A painless and weak contraction may indicate a neurological disorder or a long-standing tear of a musculotendinous unit. A painless and strong response usually indicates that the musculotendinous Fig. 26. Resisted glenohumeral internal rotation. The client resists the examiner's attempt to move the hand in a lateral direction. The hand that applies resistance is proximal to the client's wrist joint. unit is not involved. In some overuse syndromes, particularly in those involving athletes, however, manually applied resistance does not produce sufficient stress to reproduce the subject's symptoms. In these cases, examining the individual after the condition has been aggravated by activity may be helpful. These problems may be evaluated further with isokinetic testing and, in cases that are particularly difficult to diagnose, referral to a sports medicine specialist may be indicated. Pain reported on all resisted tests at a joint may indicate an acute inflammation of the joint or a surrounding structure, or the possible existence of a psychogenic problem.1 Palpation. Palpation for tenderness of involved structures should be reserved until the preceding components of the functional examination have been completed. This precaution prevents implicating a structure as being involved before completing a systematic, logical examination. Palpation, thus, is used as a confirmatory test of earlierfindingsof the functional examination. The following structures are palpated for tenderness at the shoulder girdle: 1) sternoclavicular joint, 2) clavicle, and 3) acromioclavicular joint. At the glenohumeral joint, the following structures PHYSICAL THERAPY TABLE 3 Interpretation of Pattern of Responses to Resisted Testing1 Combined Test Results Strong and painless Strong and painful Weak and painless Weak and painful All tests painful Status of Nervous System Status of Muscular System no abnormality no abnormality nerve compression or peripheral neuropathy serious pathological condition (fracture, tumor) no abnormality contractile lesion present longstanding rupture or tendon avulsion serious pathological condition (fracture, tumor, recent severe tear) acute inflammation or psychogenic condition APPENDIX 1 Upper Quarter Screening Examination Fig. 27. Resisted glenohurneral external rotation. The client resists the examiner's attempt to move the hand in a medial direction. The hand that applies resistance is proximal to the client's wrist joint. Fig. 28. Resisted elbow flexion. The client resists the examiner's attempt to extend the elbow. Fig. 29. Resisted elbow extension. The client resists the examiner's attempt to flex the elbow. Volume 66 / Number 12, December 1986 Observation Posture of head, spine and rib cage, and upper limb Contour (atrophy or deformity) Skin (color, wounds, abrasions) Active range of motion Elevation of upper limbs Cervical spine (passive overpressure on rotation) Resisted testing Shoulder-girdle elevation Shoulder abduction Elbow flexion Elbow extension Wrist extension Wrist flexion Thumb extension Finger adduction are palpated: 1) the subdeltoid bursa, 2) the supraspinatus tendon, 3) the subscapularis tendon, 4) the infraspinatus tendon, 5) the teres minor tendon, and 6) the tendon of the long head of the biceps brachii muscle. Cyriax and Hoppenfeld have described specific palpation techniques.1,11 Neurological examination. A neurological examination should be conducted if indicated by the screening or specific examinations. Factors that indicate the necessity of a neurological examination include 1) weakness of a muscle on resisted testing, 2) subjective complaints of paresthesia or anesthesia in the upper limb, and 3) a history of an injury that is known to produce neurological insult. The neurological examination includes testing of the client's motor function, sensation, and reflexes. If one or more muscles are found to be weak, the examiner must test the deep tendon reflexes of the upper limb, including reflexes of the biceps brachii, triceps brachii, and brachioradialis muscles. Sensation of all dermatomes from the C4 segment through the Tl segment are examined, as are the distributions of all peripheral nerves of the upper limb. Common neurological disorders of the shoulder complex include 1) axillary nerve injury secondary to fracture or dislocation of the proximal humerus and 2) brachial plexus involvement secondary to traction injury or to compromise at the thoracic outlet. In the latter case, investigation of the circulatory status of the upper limb is warranted. A complete description of the syndromes associated with these neurological insults is beyond the scope of this article. These and other neurological problems of the shoulder complex have been described thoroughly by Haymaker and Woodhall12 and by Pratt (see the article by N. E. Pratt in this issue). Additional examinations. Clinical signs that indicate the need for neurological assessment also may require electrophysiological testing for a definitive diagnosis. Any familial history of a systemic disease such as rheumatoid arthritis or diabetes mellitis should be investigated further by an appropriate specialist. Further required evaluation procedures may include various radiological techniques and aspiration of joint fluid. 1875 APPENDIX 2 Examination of the Shoulder Complex Subjective Examination Specific Questions General Questions What caused you to consult a physician? If pain: Where is the pain felt? Has the pain spread? Does it go below the elbow? Does it reach the wrist? Is it constant or intermittent? If constant: Does it vary in intensity? What makes it worse? Can you sleep on the involved side? What eases the pain? What brings on the pain? Once present, how long does it remain? At what time of day is the pain worst? Does the pain awaken you from sleep? If intermittent: If loss of function: What are your functional limitations? Do you have difficulty combing your hair? Do you have difficulty with personal hygiene? What other specific tasks give you difficulty? How did this problem begin? Was there an injury? If so, when and how did it occur? If not, can you identify a precipitating factor (habitual, repetitive, or uncommon, prolonged activity)? How long has this problem been present? Have you ever had this problem or a similar problem in the past? Do you have any related problems? How is your health other than the problem with your shoulder? Are you diabetic? Do you have problems with other joints? Have you had any operations? If so, why were they performed? Objective Examination Inspection Posture Contour Activities of daily living Skin Assistive devices Accessory movements Sternoclavicular joint superior glide of medial clavicle inferior glide of medial clavicle posterior glide of medial clavicle anterior glide of medial clavicle Functional examination Active range of motion Shoulder girdle elevation depression protraction retraction Shoulder flexion extension abduction external rotation internal rotation horizontal adduction elevation 1876 Acromioclavicular joint anterior glide of lateral clavicle posterior glide of lateral clavicle inferior glide of acromion (stress test) Glenohumeral joint distraction of humeral head posterior glide of humeral head anterior glide of humeral head superior glide of humeral head inferior glide of humeral head PHYSICAL THERAPY APPENDIX 2 Examination of the Shoulder Complex Objective Examination Resisted tests Shoulder girdle elevation depression protraction retraction Passive ROM Shoulder girdle elevation depression protraction retraction distraction (scapulothoracic) Shoulder flexion extension abduction adduction internal rotation external rotation elbow flexion elbow extension Shoulder flexion extension abduction external rotation internal rotation horizontal adduction elevation Neurological examination Reflexes Motor Sensory Palpation Sternoclavicular joint Clavicle Acromioclavicular joint Subscapularis tendon Biceps brachii tendon (long head) Supraspinatus tendon Infraspinatus tendon Teres minor tendon Palpable portion of subdeltoid bursa CONCLUSION An outline of the examination of the shoulder complex has been provided with emphasis on the functional examination and interpretation of this portion of the examination. Attention to the details of this examination should enable the physical therapist to identify movement disorders of the shoulder complex. These disorders can be divided into dysfunctions of the contractile tissues and dysfunctions of the noncontractile tissues. Interpretation of the results of the examination is important. The physical therapist must determine not only which tissues are involved but also the stage of the pathological process. Appropriate treatment goals then may be esVolume 66 / Number 12, December 1986 Additional examinations Radiology Laboratory examination Electrodiagnosis Punctures (biopsy, aspiration) Special examination (referral to other specialists) tablished on the basis of this evaluation. If the examination principles we have described are followed, they will lead to treatment with the potential to optimize the client's function. REFERENCES 1. Cyriax J: Textbook of Orthopaedic Medicine: Diagnosis of Soft Tissue Lesions, ed 5. Baltimore, MD, Williams & Wilkins, 1970, vol 1, pp 217-274 2. Cailliet R: Shoulder Pain. Philadelphia, PA, F A Davis Co, 1966 3. Maitland GD: Peripheral Manipulation. Boston, MA, Butterworth Publishers, 1977 4. Kaltenborn FM: Manual Therapy for the Extremity Joints: Specialized Tests, Techniques, and Joint Mobilization, ed 2. Oslo, Norway, Olaf Norlis Bokhandel A/S, 1976 5. deAndrade JR, Grant C, Dixon SJ: Joint distension and reflex muscle inhibition in the knee. J Bone Joint Surg [Am] 47:313, 1965 6. Lequesne M:Increasedassociation of diabetes mellitus with capsulitis of the shoulder and shoulder-hand syndrome. Scand J Rheumatol 6:53-56, 1977 7. Laul VS, referred to in Gray RC, Gottlieg NL: Rheumatic disorders associated with diabetes mellitus: Literature review. Semin Arthritis Rheum 6:19-34, 1976 8. Cyriax J, Cyriax P: Illustrated Manual of Orthopaedic Medicine. London, England, Butterworth & Co Ltd, 1983, pp 29-46 9. Mennell JM: Joint Pain: Diagnosis and Treatment Using Manipulative Techniques. Boston, MA, Little, Brown & Co, 1964 10. McGlynn FJ, El-Khoury G, Albright JP: Arthrotomography of the glenoid labium in shoulder instability. J Bone Joint Surg [Am] 64:506518,1982 11. Hoppenfeld S: Physical Examination of the Spine and Extremities. East Norwalk, CT, Appleton-Century-Crofts, 1976 12. Haymaker W, Woodhall B: Peripheral Nerve Injuries: Principles of Diagnosis, ed 2. Philadelphia, PA, W B Saunders Co, 1953 1877