International Journal for Quality in Health Care Advance Access published September 2, 2011
International Journal for Quality in Health Care 2011; pp. 1 –10
10.1093/intqhc/mzr050
Are United States and Canadian cancer
screening rates consistent with guideline
information regarding the age of screening
initiation?
SRIKANTH KADIYALA1 AND ERIN C. STRUMPF2,3
1
Rand Corporation, 1776 Main Street, Santa Monica, CA 90401, USA, 2Department of Economics, McGill University, Leacock Building,
Rm 418, 855 Sherbrooke Street West, Montreal, QC, Canada H3A 2T7, and 3Departments of Epidemiology, Biostatistics, and
Occupational Health, McGill University, Leacock Building, Rm 418, 855 Sherbrooke Street West, Montreal, QC, Canada H3A 2T7
Address reprint requests to: Srikanth Kadiyala, Rand Corporation, 1776 Main Street, Santa Monica, CA 90401, USA.
Tel: þ1-301-393-0411; Fax: þ1-310-393-4818; E-mail: kadiyala@rand.org
Accepted for publication 4 July 2011
Abstract
Objective. To understand whether US and Canadian breast, colorectal and prostate cancer screening test utilization is consistent with US and Canadian cancer screening guideline information with respect to the age of screening initiation.
Setting. Canada and the US.
Participants. Canadian and American women of ages 30 –60 and men of ages 40 – 60.
Interventions. None.
Main Outcomes Measures. Mammography, prostate-specific antigen (PSA) and colorectal cancer test use within the past 2 years.
Methods. We identify US and Canadian compliance with age screening information in a novel manner, by comparing test utilization rates of individuals who are immediately on either side of the guideline recommended initiation ages.
Results. US mammography utilization within the last 2 years increased from 33% at age 39 to 48% at age 40 and 60% at age 41.
US colorectal cancer test utilization, within the last 2 years, increased from 15% at age 49 to 18% at age 50 and 28% at age 51.
US PSA utilization within the last 2 years increased from 37% at age 49 to 44% at age 50 and 54% at age 51. In Canada, mammography utilization within the last 2 years increased from 47% at age 49 to 57% at age 50 and 66% at age 51.
Conclusion. American and Canadian cancer screening utilization is generally consistent with each country’s guideline recommendations regarding age. US and Canadian differences in screening due to guidelines can potentially explain cross-country differences
in breast cancer mortality and affect interpretation of international comparisons of cancer statistics.
Keywords: health policy, guidelines, cancers, prevention (incl. screening)
Introduction
Cancer screening guidelines provide important information
to physicians and patients regarding optimal medical treatment. Given the rapid pace at which new medical information is generated, guidelines are also useful tools for
disseminating information resulting from advances in
medical research. In this study we examine whether US and
Canadian physicians and patients follow cancer screening
guideline information with respect to the age at which
screening is recommended to begin. We analyze US and
Canadian screening patterns simultaneously because guideline
information varies across the two countries both regarding
whether a screening test is recommended as effective ( prostate cancer) and the age when screening is recommended to
begin (breast cancer).
While many professional organizations publish cancer
screening guidelines (e.g. American Urological Association,
Canadian Association of Gastroenterology), Federal agencies
and national cancer associations in both countries generally
International Journal for Quality in Health Care
# The Author 2011. Published by Oxford University Press in association with the International Society for Quality in Health Care;
all rights reserved
Page 1 of 10
Downloaded from by guest on March 6, 2016
Design. Cross-sectional, regression discontinuity.
Kadiyala and Strumpf
Page 2 of 10
We contribute to this area of research by focusing on
whether breast, colorectal and prostate cancer screening test
rates are consistent with guideline age information. By specifying an age at which screening should begin, the guidelines
implicitly recommend that screening does not occur for
asymptomatic individuals below that age, often due to low
specificity of the test and the health consequences of
unnecessary intervention and treatment [31]. We approach
this question of age-appropriate screening in both countries
by comparing cancer test utilization rates for individuals
close to and on either side of the guideline recommended
initiation ages. Cross-country differences in the levels and
timing of screening utilization have the potential to generate
differences in population health and affect comparisons of
cancer survival statistics across countries.
Methods
Study sample
We calculate US cancer test rates using the 2006 BRFSS and
the 2003 National Health Interview Survey (NHIS) [32, 33].
For Canada, we calculate test rates from the 2003 and 2005
Canadian Community Health Surveys (CCHS) [34, 35]. All
three are nationally representative surveys that measure
health-care utilization in their respective countries. Sample
sizes from the BRFSS are significantly larger than the NHIS,
but only the NHIS questions individuals below the age of 50
about colorectal cancer test use. We use 2 years of the CCHS
survey because the colorectal and prostate cancer test questions were asked in different provinces in different years.
Survey response rates for the cancer test questions are extremely high in all of these surveys—approximately 95%.
Finally, the BRFSS, NHIS and the CCHS all use complex
survey designs to collect information. All of the following
analyses take the surveys’ complex sampling frames into
account via weighting and adjusted standard errors.
Outcome measures
For breast, colorectal and prostate cancers we examine
cancer test use within the past 2 years, using this timeframe
due to the biennial periodicity recommended in the Canadian
guidelines. For breast cancer we calculated the proportion of
women who received a mammogram in the past 2 years. For
colorectal cancer, none of the guidelines takes a stance on
which colorectal screening test to perform. Consequently, we
calculated the proportion of individuals who received a
home FOBT, sigmoidoscopy or colonoscopy in the past 2
years. For prostate cancer the proportion of men who
received a PSA test in the previous 2 years was the primary
measure examined. The CCHS and NHIS surveys also ask
individuals about the reasons for using cancer tests. Cancer
tests can be used for both screening reasons, i.e. cancer
detection in asymptomatic individuals and for non-screening
reasons if individuals have symptoms that must be evaluated.
We also use information detailing the reason for testing
Downloaded from by guest on March 6, 2016
set the standard. The US Preventive Services Task Force
(USPSTF) and the Canadian Task Force on Preventive
Health Care (CTFPHC) base their guidelines on the quality
of evidence from clinical trials and rate their recommendations accordingly [1 – 7]. The American Cancer Society
(ACS) and the Canadian Cancer Society (CCS) also publish
guidelines based on evidence from clinical trials, but also
base recommendations on evidence from observational
studies [6– 10]. From each of these guidelines we focus on
the screening recommendations for breast, colorectal and
prostate cancers because these are the three largest cancers in
terms of incidence.
Table 1 summarizes breast, colorectal and prostate cancer
screening guidelines from the ACS, CCS, CTFPHC and the
USPSTF that were in effect during the time of data used for
analyses in this study. For breast cancer, the ACS and
USPSTF recommend mammography screening be initiated at
age 40 for asymptomatic women, while the CTFPHC and
CCS recommend that mammography screening be initiated
for women starting at age 50. In 2009, the USPSTF changed
its position and now recommends against routine screening
mammography in women ages of 40 – 49 and that physicians
and patients make decisions on an individual case-by-case
basis regarding screening between ages of 40 and 49 [11].
The CTFPHC and the CCS do not recommend mammography screening for women after age 69. For colorectal cancer,
all four guidelines recommend that screening begin at age 50
for asymptomatic men and women. For prostate cancer the
ACS recommends that physician offer prostate specific
antigen (PSA) screening to men aged 50 and older. The
other three organizations recommend either not using the
PSA test (CTFPHC), recommend discussion of the test with
physicians (CCS) or conclude that there is insufficient evidence regarding whether or not PSA testing is effective
(USPSTF).
An extensive literature has evaluated cancer test rates for
targeted age groups in the US and Canada. All of these
studies interpret high test rates among the targeted age group
as guideline compliance. In Canada, Zarychanski et al. [12]
report that 17.6% of asymptomatic individuals of ages 50 and
older were up to date on their colorectal screening in 2003
and Beaulac et al. [13] report that 24.7% of men of ages 40
and older had a recent PSA screening test within the last year
in the years 2000 and 2001. In 2001, approximately half of
Canadian women age 50 – 69 reported mammography screening in the past 2 years [14]. In the US, a recent paper by
Smith et al. [15] uses the 2004 Behavioral Risk Factor
Surveillance System (BRFSS) data to evaluate screening. They
find that 58% of women of ages 50 – 64 received a mammogram within the previous year, 19% of women and men of
ages 50 – 64 received a home fecal occult blood test (FOBT)
within the previous year, and 54% of men of ages 50 – 64
received a PSA test within the previous year. A number of
other studies have evaluated US breast [16–22], colorectal
[11–18, 20, 21, 23–27] and prostate [17, 18, 20, 21, 24, 28–30]
cancer test use in the 1990s and 2000s. The overarching conclusion from all of these studies in both countries is that
cancer test rates are below the ideal for targeted ages.
Table 1 ACS, CCS, CTFPHC and USPSTF Cancer Screening Guidelines (effective during data survey years)
US
Canada
............................................................................................................................................................................................................................................
Breast cancer
Colorectal cancer
Prostate cancer
CTFPHC (2001)
Test: mammography, every 1– 2 years
Population: asymptomatic women ages 50 – 69
American Cancer Society (2004)
Test: mammography, annually
Population: asymptomatic women age 40þ
Canadian Cancer Society (2008)
Test: mammography, every 2 years
Population: asymptomatic women of ages 50 – 69
USPSTF (2002)
Test(s): FOBT (good evidence) annually and or sigmoidoscopy (fair evidence)
every 5 years; no direct evidence for colonoscopy
Population: asymptomatic individuals age 50þ
CTFPHC (2001)
Test(s): FOBT (good evidence) every 1– 2 years,
sigmoidoscopy (fair evidence) periodicity unspecified,
insufficient evidence to include or exclude colonoscopy
Population: asymptomatic individuals age 50þ
American Cancer Society (2004)
Tests and frequency: FOBT annually, flexible sigmoidoscopy every 5 years,
colonoscopy every 10 years, double contrast barium enema every 5 years,
Population: asymptomatic individuals age 50þ
Canadian Cancer Society (2008)
Test and frequency: FOBT at least every 2 years
Population: asymptomatic individuals age 50þ
USPSTF (2002)
Insufficient evidence to recommend or not recommend the test
CTFPHC (2000)
PSA testing not to be used due to low positive predictive
value and risk of adverse affects associated with treatment
Canadian Cancer Society (2000)
Test: PSA
Population: men age 50þ should discuss with
physician the benefits and risks of PSA
American Cancer Society (2004)
Test: offer PSA, annually
Population: 50þ men who have at least a 10-year life expectancy
Source: U.S. Screening Guidelines: ACS Breast, Colorectal, Prostate Cancer (8). USPSTF Breast Cancer, Colorectal, Prostate Cancer (1,2,3). Canadian Screening Guidelines: CTFPHC Breast
Cancer (4), CTFPHC Colorectal Cancer (5), CTFPHC Prostate Cancer (6), CCS Breast Cancer (9), CCS Colorectal Cancer (10), CCS Prostate Cancer (6).
Page 3 of 10
US and Canadian cancer screening
USPSTF (2002)
Test: mammography, every 1 –2 years
Population: asymptomatic women age 40þ
Downloaded from by guest on March 6, 2016
Kadiyala and Strumpf
when available to understand U.S and Canadian cancer test
use at the guideline recommended ages.
Analytic strategy
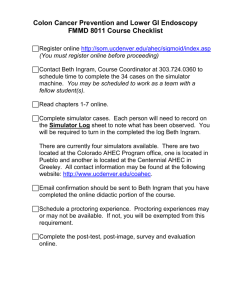
Figure 1 Canada and US mammography test use.
Page 4 of 10
Results
Breast cancer
Figure 1 plots mammography test rates in the past 2 years by
age for women in Canada and the US, revealing several interesting patterns. At every age, the probability of a woman
receiving a mammogram is higher in the US than in Canada.
Between ages 40 and 50, where the countries’ guidelines
differ, test use varies by as much as 42 percentage points at
age 45. Consistent with the USPSTF and ACS guidelines,
there is a large discrete increase in mammography rates
in the US near age 40, rising from 33% at age 39 to 48%
(P , 0.001) at age 40 and 60% (P , 0.001) at age 41. In
Canada, mammography rates rise significantly at age 50,
Downloaded from by guest on March 6, 2016
The guidelines’ specification of a screening initiation age
implies that, if the guideline information is being followed by
physicians and patients, cancer screening rates should
increase sharply at, or near, the recommended ages. Not
finding such discontinuities would suggest that patients and
physicians are not using guideline age information in their
cancer screening decisions. While a high screening rate
among the target group would suggest compliance with
respect to those who should be screened, a similarly high
rate among the non-targeted group would suggest lack of
compliance with respect to the initiation age. If the age
thresholds are important for physician and patient decisionmaking for mammography utilization, one should observe a
sharp increase in utilization for women near age 40 in the
US and near age 50 in Canada. Similarly in the case of colorectal cancer we look for a discrete change in the colorectal
cancer screening rate near age 50 in both the US and
Canadian data. For the PSA test, consistent with the ACS
guideline information, we look for a change in screening near
age 50 for men in the US. While the CTFPHC does not recommend PSA testing, high PSA screening rates indicate that
many men are indeed using the test in Canada, so we test to
see whether screening behavior in Canada is consistent with
the ACS guideline.
In our analyses we first plot cancer test rates within the
past 2 years by age for each of the cancer types. We then formally test for a break at the specified ages using logistic
regression models with test use in the last 2 years as the
dependent variable. Our key independent variable is an indicator variable that assumes a value of 1 if the individual is
above the recommended initiation age and zero otherwise.
Our regression samples include individuals within 10 years
of age on either side of the initiation age, so the non-targeted
group is similar to the targeted group in terms of their age
cohort and in demographic, socio-economic and health
characteristics that may also impact cancer screening rates. To
control for any remaining differences between the two
groups, we control for age trends (age, age-squared, agecubed), sex (for colorectal cancer test use), race, education,
family income, health insurance and marital status. Linear
and non-linear age trends are included to control for the
linear relationship between age and screening rates over
shorter age ranges and the potential for non-linear relationships over longer age spans. In the regression specification,
race is an indicator variable that assumes a value of 1 if the
individual is non-white and zero otherwise. Education is
defined by four variables: less than high school, high school
graduate, some college and college graduate or higher. We
adjust for marital status by using the following categories:
married, divorced or separated, widowed, never married and
a member of an unmarried couple. In the US, we adjust for
whether or not an individual has private or public health
insurance. For family income we group individuals into
income quartiles.
US and Canadian cancer screening
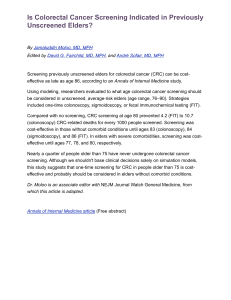
Colorectal cancer
Figure 2 plots colorectal cancer test use in the past 2 years
by age for men and women in Canada and the US. Unlike
mammography, Canadian and US colorectal test rates are
similar across the entire age distribution. Even though the
test rates are similar, the changes in test rates near the age 50
threshold are larger in the US than in Canada. The US data
show that colorectal cancer test rates rise from 15% at age
49 to 18% (P ¼ 0.199) at age 50 and 28% at age 51 (P ,
0.001). In Canada the shift in test use is less striking, rising
from 15% at age 49 to 17% at age 50 (P ¼ 0.367) and 21%
at age 51 (P ¼ 0.02).
Table 2 presents regression results for the Canadian and
US data with colorectal test use as the dependent variable of
interest. In addition to age trends and other covariates from
the mammography regressions, we include a dummy variable
for females. Holding all the other covariates constant, being
above the age threshold only increases the probability of
being tested by 1.3 percentage points in Canada, but this
difference is not statistically significant (OR ¼ 1.11; P ¼
0.53). In the US, all else equal, being above the recommended initiation age increases the probability of colorectal test use in the past 2 years by 4.7 percentage points
(OR ¼ 1.39; P ¼ 0.049).
Prostate cancer
Figure 3 shows that age-specific PSA test rates are generally
high in both countries, but higher in the US. PSA test rates
increase substantially near the guideline recommended age in
the US, from 37% at age 49 to 44% (P ¼ 0.007) at age 50
and 54% (P , 0.001) at age 51. In Canada, there does not
appear to be a discrete increase at the particular age of 50 that
is separate from the increasing trend with age. Thirty-five
percent of men are tested at age 49 and at age 51 (P ¼ 0.921).
Table 2 presents regression results for the Canadian and
US data with prostate cancer test use as the dependent variable. Consistent with Fig. 3, the US regression results indicate
that holding all other covariates constant, being above the
age threshold increases the probability of being tested in the
last 2 years by 9.4 percentage points (OR ¼ 1.48; P ,
0.001). There is no similar effect above the ACS recommended age for Canadian men (OR ¼ 1.043; P ¼ 0.843).
Discussion
We draw three conclusions from the results presented in the
previous section. First, except in the case of colorectal cancer
in Canada, each country’s screening practices are consistent
with its own guideline age of initiation information. Second,
in the US, relative to test rates below the initiation age, compliance with guideline age information is strongest for mammography and colorectal cancer test use. This is consistent
with the randomized control trial evidence showing that
these tests are effective in increasing survival. Third, for each
of the cancer types, there are differences in the timing of test
initiation between the US and Canada. The starkest difference is seen in the case of mammography, where test rates
increase dramatically for women at age 40 in the US and at
age 50 in Canada. Cancer test use differences are also noticeable across the two countries for colorectal and prostate
cancer test use, due in part to higher US compliance with
US guideline age information.
What are the implications of the differences in crosscountry test rates identified in this paper? First, the significant difference in breast cancer screening rates among
women of ages 40 – 50 may contribute to differences in
health outcomes. Meta-analyses of randomized control trials
indicate that mammography screening in the under-age-50
population reduces 10-year mortality by 15 – 20% [36],
although we note that there is disagreement in the literature
on this important question [37]. If the 15 – 20% figures are
applicable to the general population, the 34 percentage point
difference in mammography rates for women of ages 40 – 50
between the US and Canada may explain a part of the 6.9%
(2000 – 2004) breast cancer mortality gap between Canada
and the US for the 50 – 54 age group [38 – 43]. We also identified cross-country differences in the timing of colorectal
cancer test use, although the smaller gap of 6 percentage
points within the 10 years after age 50 indicates less potential
for resulting differences in health outcomes than for mammography. Cross-country differences in prostate cancer test
Page 5 of 10
Downloaded from by guest on March 6, 2016
from 47% at age 49 to 57% (P ¼ 0.008) at 50 and 66% by
age 51 (P , 0.001). The graph also indicates that mammography rates in Canada begin to decrease starting at age 70, a
finding that is consistent with the CTFPHC and CCS guidelines. The US data do not show a similar decrease in mammography rates until a woman reaches her late 70s.
The mammography rates suggest that physicians and
women in both countries are following the guidelines for
breast cancer screening. However, the graphs also show a
clear upward trend in mammography rates as women age, as
well as possible discrete shifts at ages other than those specified in the guidelines. For example, Canadian rates rise from
13% at age 39 to 24% (P , 0.001) at age 41, potentially indicating a second trend break. Regression analysis allows us to
test whether the breaks that are apparent in the graph persist
after controlling for age trends and other covariates.
Table 2 shows that, even after adjusting for all the other
covariates, being above the age threshold in Canada increases
the probability of being tested within the last 2 years by 9.9
percentage points (OR ¼ 1.49; P ¼ 0.002). Similarly, in the
US data being above the recommended initiation age
increases the probability of being tested by 10.7 percentage
points (OR ¼ 1.55; P , 0.001). Since the results in Fig. 1
show a non-trivial increase in mammography rates at age 40
in Canada, we also estimated a regression model that tests
for a break at age 40. After controlling for trends in age, we
did not find a statistically significant break (results not
shown) at age 40 in Canada. Similarly, the apparent decrease
at age 70 is not significant after controlling for a linear age
trend. Overall, these results indicate that significant breaks in
mammography rates occur at the initiation ages indicated by
each country’s guideline information.
Kadiyala and Strumpf
Page 6 of 10
Table 2 Impact of guideline initiation age on cancer test use
Mammograma
Colorectal cancer test usea
...................................................................
.................................................................
....................................................................
Canada
Canada
Adjusted
odds ratios
(95% CIs)
Canada
Adjusted
odds ratios
(95% CIs)
US
Adjusted
odds ratios
(95% CIs)
PSA
Adjusted
odds ratios
(95% CIs)
US
Adjusted
odds ratios
(95% CIs)
US
Adjusted
odds ratios
(95% CIs)
1.107
0.017**
1.088**
0.999**
0.951
0.945
1.021
(0.806, 1.521)
(0.001, 0.375)
(1.022, 1.160)
(0.999, 1.000)
(0.848, 1.067)
(0.775, 1.152)
(0.813, 1.281)
1.390*
0.157
1.04
1.000
0.970
1.050
1.006
(1.002, 1.930)
(0.004, 5.49)
(0.969, 1.119)
(0.9992, 1.000)
(0.863, 1.091)
(0.893, 1.23)
(0.768, 1.319)
1.043
(0.689, 1.578)
0.920
(0.011, 75.134)
1.007
(0.922, 1.101)
1.000
(0.999, 1.001)
Not applicable
0.720*
(0.544, 0.952)
0.852
(0.597, 1.217)
1.480*** (1.212, 1.80)
4.61
(0.458, 46.328)
0.972
(0.928, 1.019)
1.000
(0.999, 1.000)
Not applicable
1.291*** (1.155, 1.443)
1.130
(0.979, 1.305)
............................................................................................................................................................................................................................................
Age cutoff
Age
Age 2
Age 3
Sex
Race non-white
Hhold income
quartile 2
Hhold income
quartile 3
Hhold income
quartile 4
Unmarried couple
Widowed
Never married
Divorced/separated
Secondary education
Secondary þ
Secondary graduate
and higher
Health insurance
N
1.489** (1.151,
0.609
(0.036,
1.016
(0.960,
1.000
(0.999,
Not applicable
1.077
(0.898,
1.150
(0.958,
1.927)
10.268)
1.076)
1.000)
1.291)
1.380)
1.55***
(1.311,
0.031*** (0.008,
1.102*** (1.065,
0.999*** (0.999,
Not applicable
1.356*** (1.242,
1.048
(0.925,
1.837)
0.119)
1.140)
0.999)
1.481)
1.187)
1.284**
(1.088, 1.516)
1.153*
(1.007, 1.320)
0.986
(0.810, 1.199)
0.875
(0.682, 1.124)
1.147
(0.815, 1.614)
1.271*
(1.094, 1.477)
1.412***
(1.180, 1.688)
1.303***
(1.138, 1.491)
1.240*
(1.018, 1.510)
1.044
(0.907, 1.201)
1.343
(0.946, 1.908)
1.576***
(1.350, 1.840)
0.777**
0.603***
0.817*
0.877
1.303**
1.338*
1.320***
(0.663,
(0.465,
(0.699,
(0.753,
(1.089,
(1.055,
(1.129,
0.921
0.853
1.055
1.017
1.031
1.067
1.143
(0.716,
(0.670,
(0.926,
(0.916,
(0.845,
(0.874,
(0.934,
1.070
0.903
0.931
1.059
1.047
0.893
1.185
(0.858, 1.334)
(0.651, 1.253)
(0.776, 1.115)
(0.873, 1.284)
(0.850, 1.290)
(0.690, 1.157)
(0.995, 1.411)
1.258*
1.175
0.827
0.977
1.626***
1.660***
1.984***
(0.9230, 1.713)
(0.8600, 1.606)
(0.860, 1.610)
(0.842, 1.133)
(1.278, 2.068)
(1.306, 2.105)
(1.571, 2.506)
0.718*
0.771
0.669**
0.671**
1.403*
1.361
1.479***
(0.540, 0.955)
(0.387, 1.534)
(0.493, 0.908)
(0.523, 0.862)
(1.051, 1.874)
(0.952, 1.944)
(1.153, 1.897)
1.139
1.195
0.855*
0.844*
1.236*
1.534***
1.568***
(0.864, 1.500)
(0.925, 1.542)
(0.744, 0.983)
(0.741, 0.962)
(1.003, 1.523)
(1.233, 1.909)
(1.260, 1.952)
2.286***
69 547
(2.016, 2.593)
3.427***
10 127
(2.634, 4.460)
Not applicable
7 564
2.370***
50 028
(2.029, 2.769)
Not applicable
20 554
0.911)
0.780)
0.955)
1.020)
1.558)
1.697)
1.544)
1.183)
1.086)
1.202)
1.128)
1.258)
1.301)
1.400)
Not applicable
23 802
a
Age-cutoffs-breast cancer: Canada ¼ 50, US ¼ 40. Colorectal cancer: Canada ¼ 50; US ¼ 50. Prostate cancer: Canada ¼ 50; US ¼ 50. Colorectal cancer screening includes FOBT,
sigmoidoscopy and colonoscopy. Marginal effect for the age cutoff variable from the logistic regression models from above: Canada Breast 9.9, US Breast 10.7; Canada Colorectal 1.7; US
Colorectal 4.7; US Prostate 9.4. Notes: logistic regression. Dependent variable: test use in the past 2 years.
***P 0.001, **P 0.01, *P 0.05.
Downloaded from by guest on March 6, 2016
US and Canadian cancer screening
Figure 2 Canada and US colorectal cancer test rates.
Downloaded from by guest on March 6, 2016
Figure 3 Canada and US PSA test use.
use may also affect health outcomes, although this is extremely uncertain. While observational studies indicate that
medical treatment conditional on identifying cancer does
increase survival [44], two recent randomized control trials
regarding the effects of PSA screening test on survival have
arrived at conflicting results regarding the effectiveness of
the test in increasing survival [45, 46].
A second implication of these results is that differences
across countries in the timing of screening initiation may
affect the interpretation of cross-country cancer survival statistics. Just as lead-time bias is an important problem in comparing statistics within a country over time [47], differences
across countries in the timing of screening initiation imply
that US and Canadian cancer survival statistics conditional
on detection could differ spuriously, simply because breast,
colorectal and prostate cancers are detected at an earlier age
in the US than in Canada. This is potentially an important
issue in both breast and prostate cancers as these test rates
are higher in the US relative to Canada across the entire age
distribution.
Furthermore, the methodology applied in this study can
also be used to inform comparisons of cancer statistics
between the US and other OECD countries. In the case of
breast cancer, countries including England, Scotland and
France either recommend screening near, or have national
breast cancer screening programs centered on, women aged
50 and older. Similarly in the case of prostate cancer national
guidelines in other OECD countries do not recommended
screening for men aged 50 and older. These differences can
yet again potentially aid in understanding comparisons of
cancer survival statistics between the US and other OECD
countries.
Page 7 of 10
Kadiyala and Strumpf
Limitations
In this study, we used several nationally representative
surveys to calculate age-specific cancer test rates. Test rates
are self-reported, and therefore may suffer from recall bias.
However, unless problems with recall arose or increased in
severity precisely at the recommended screening initiation
ages, this issue is unlikely to bias our results. Furthermore,
analysis based on US insurance claims data, which would not
be subject to recall bias, finds very similar results to the ones
presented here [53]. A second potential limitation in this
study is that guideline recommendations apply to asymptomatic individuals and our results include test use for nonasymptomatic reasons. We are able to separate out screening
done for routine, preventive purposes versus test use for
symptomatic reasons in the CCS and the NHIS surveys but
not the BRFSS. In the CCHS surveys, only examining
routine screening as the dependent variable and adjusting for
the other covariates as defined above, the sharp increase at
the age of recommended screening initiation persists
(OR ¼ 1.516; P ¼ 0.003). Conversely, among women
Page 8 of 10
receiving a mammography for diagnostic reasons, test rates
increase slowly and smoothly with age and do not change in
a discrete manner at the guideline recommended ages
(OR ¼ .998; P ¼ 0.990). We find similar results for colorectal cancer test use in the US. Routine screening increases in a
discrete manner at age 50 (OR ¼ 1.58; P ¼ 0.012) and diagnostic test use does not (OR ¼ .757; P ¼ 0.366). These
results indicate that changes in test use identified at the
guideline recommended initiation ages are primarily due to
changes in the screening of asymptomatic individuals.
Conclusion
This study compares US and Canadian compliance with
guideline information with respect to the age of cancer
screening initiation. We showed that compliance is strongest
for breast and colorectal cancer screening in the US and for
breast cancer screening in Canada. Compliance with colorectal screening guideline age information is mixed across
countries as colorectal screening in the US rises at the
expected age but Canadian colorectal cancer screening does
not. In the case of breast cancer, existing knowledge regarding the effect of mammography screening on mortality
suggests that the large test use differences identified between
the two countries have the potential to generate population
health differences. For colorectal and prostate cancers, the
identified differences in test use are potentially less likely to
lead to differences in population health due to the smaller
identified differences in magnitudes and the uncertainty in
the effectiveness of the PSA test. Finally, due to lead-time
bias, differences in the timing of screening utilization across
countries have the potential to affect the interpretation of
cross-country comparisons of cancer survival statistics.
Funding
Funding support from McGill University (Strumpf ) and the
University of Washington and RAND (Kadiyala) is gratefully
acknowledged.
References
1. USPSTF (United States Preventive Services Task Force).
Screening for colorectal cancer: recommendations and rationale.
Ann Intern Med 2002;137:129 –31.
2. USPSTF (United States Preventive Services Task Force).
Screening for prostate cancer: recommendations and rationale.
Ann Intern Med 2002;137:915 –6.
3. USPSTF (United States Preventive Services Task Force).
Screening for breast cancer: recommendations and rationale.
Ann Intern Med 2002;137(5 Part I):344– 46.
4. Ringash J, CTFPHC (Canadian Task Force Preventive Health
Care). Preventive health care, 2001 update: screening
Downloaded from by guest on March 6, 2016
These results also raise several questions regarding the
effectiveness of recommendations to stop screening after a
certain age. The CTFPHC and CCS guidelines do not recommend mammography screening after age 69 and the
USPSTF also notes that at the older ages the benefits of
screening older women decrease relative to the costs. The
rationale behind this recommendation is that older women
are more likely to die of other causes than from breast
cancer [48]. Our findings indicate that in the US mammography test use stays at a very high level until a woman reaches
her late 70s. In contrast, mammography test use in Canada
begins a slow decline starting at the CTPFHC recommended
stopping age. While there is no sharp decline at age 70 that
is directly attributable to guideline age information, these
results suggest that physicians or patients in Canada have
mechanisms for moderating the use of mammography at the
older ages.
Finally, Canadian physicians and patients are less likely to
comply with the colorectal cancer screening age information
than US physicians and patients. Specifically colorectal cancer
test use in Canada does not increase in a discrete manner at
the guideline recommended age of 50. This difference could
be due to country-level differences such as supply of gastroenterologists [49, 50], physician payment incentives (including
under managed care), malpractice systems or reductions in
the price of screening at the guideline recommended ages
due to insurance coverage in the US [51]. Another potential
explanation is that variation in Canadian province-specific
screening programs, professional recommendations, payment
rates may result in no single guideline being followed
country-wide [52]. What the US and Canada share in the colorectal context, however, are age-specific screening rates that
are far below those for either breast or prostate cancer.
Opportunities to increase colorectal cancer screening rates,
and compliance with clinical guidelines, should be considered
in both countries.
US and Canadian cancer screening
mammography among women aged 40 –49 years at average
risk of breast cancer. CMAJ 2001;164:469 –76.
5. CTFPHC (Canadian Task Force Preventive Health Care).
Preventive health care colorectal cancer screening. CMAJ
2001;165:206 –8.
6. Lipskie TL. Resource file A summary of cancer screening
guidelines. Chronic Dis Canada 1998;19:112– 30.
7. Franco E, Duarte-Franco E, Rohan TE. Evidence-based policy
recommendations on cancer screening and prevention. Cancer
Detect Prev 2002;26:350 –61.
8. Smith RA, Cokkinides V, Eyre HJ. American cancer society
guidelines for the early detection of cancer, 2004. CA Cancer J
Clin 2004;54:41 – 52.
9. Early screening and detection for breast cancer. http://www.
cancer.ca/Canada-wide/Prevention/Get%20screened/Early%
20detection%20and%20screening%20for%20breast%20cancer.
aspx?sc_lang=en (15 December 2008, date last accessed).
10. Screening for colorectal cancer. http://www.cancer.ca/
Canada-wide/About%20cancer/Types%20of%20cancer/Screening%
20for%20colorectal%20cancer.aspx?sc_lang=en (15 December
2008, date last accessed).
22. Wallace AE, Mackenzie TA, Weeks WB. Women’s primary care
providers and breast cancer screening: who’s following the
guidelines?. Am J Obstet Gynecol 2006;194:744– 8.
23. Ioannou GN, Chapko MK, Dominitz JA. Predictors of colorectal cancer screening participation in the United States. Am J
Gastroenterol 2003;98:2082 –91.
24. Sirovich BE, Schwartz LM, Woloshin S. Screening men for
prostate and colorectal cancer in the United States. Does practice reflect the evidence?. JAMA 2003;289:1414 – 20.
25. Chao A, Connell CJ, Cokkinides V et al. Underuse of screening
sigmoidoscopy and colonoscopy in a large cohort of US adults.
Am J Public Health 2004;94:1775 –81.
26. Seeff LC, Nadel MR, Klabunde CN et al. Patterns and predictors of colorectal cancer test use in the adult U.S. population.
Cancer 2004;100:2093 –2102.
27. Peterson NB, Murff HJ, Ness RM et al. Colorectal cancer
screening among men and women in the United States. J
Womens Health 2007;16:57– 65.
28. Moran WP, Cohen SJ, Preisser JS et al. Factors influencing the
use of the prostate-specific antigen screening test in primary
care. Am J Manag Care 2000;6:315 –24.
29. Dyche DJ, Ness J, West M et al. Prevalence of prostate specific
antigen testing for prostate cancer in elderly men. J Urol
2006;175:2078 –82.
12. Zarychanski R, Chen Y, Bernstein CN et al. Frequency of colorectal cancer screening and the impact of family physicians on
screening behavior. CMAJ 2007;77:593–97.
30. Meissner HI, Breen N, Klabunde CN et al. Patterns of colorectal cancer screening uptake among men and women in
the United States. Cancer Epidemiol Biomarkers Prev
2006;15:389– 94.
13. Beaulac JA, Fry RN, Onysko J. Lifetime and recent prostate
specific antigen(PSA) screening of men for prostate cancer in
Canada. Can J Public Health 2006;97:171 –76.
14. Health Canada. Progress report on cancer control in Canada.
Ottawa, ON, 2004.
15. Smith RA, Cokkinides V, Eyre HJ. Cancer screening in the
United States, 2007. CA Cancer J Clin 2007;57:90 –104.
16. Anderson LM, May DS. Has the use of cervical: breast and colorectal cancer screening increased in the United States?. Am J
Public Health 1995;85:840– 42.
17. Ruffin MT, Gorenflo DW, Woodman B. Predictors of screening
for breast, cervical, colorectal, and prostate cancer among
community-based primary care practices. J Am Board Fam Pract
2000;13:1 –10.
18. Lemon S, Zapka J, Puleo E et al. Colorectal cancer screening participation: comparisons with mammography and
prostate-specific antigen screening. Am J Public Health
2001;91:1264 –72.
19. Adams EK, Florence CS, Thorpe KE et al. Preventive care:
female cancer screening, 1996 –2000. Am J Prev Med
2003;25:301 –7.
20. Swan J, Breen N, Coates RJ et al. Progress in cancer screening
practices in the United States: results from the 2000 national
health interview survey. Cancer 2003;97:1528 –40.
21. Jerant AF, Franks P, Jackson JE et al. Age-related disparities in
cancer screening: analysis of 2001 behavioral risk factor surveillance system data. Ann Fam Med 2004;2:481 –87.
31. USPSTF (United States Preventive Services Task Force).
Screening for prostate cancer: USPSTF Recommendation
Statement. Ann Intern Med 2008;149:185–91.
32. BRFSS (Behavioral Risk Factor Surveillance System) (online
database:
http://www.cdc.gov/brfss/technical_infodata/
surveydata.htm). Atlanta, GA: Centers for Disease Control and
Prevention, 2006.
33. NHIS (National Health Interview Survey) (online database: http
://www.cdc.gov/nchs/nhis.htm). Atlanta, GA: Centers for
Disease Control and Prevention, 2003.
34. Statistics Canada. Canadian Community Health Survey Cycle
2.1 (2003). Microdata File User Guide, 2005. http://prod.
library.utoronto.ca:8090/datalib/codebooks/cstdli/cchs/cycle2_1/
guide_e.pdf.
35. Statistics Canada. Canadian Community Health Survey Cycle
3.1 (2005). Microdata File User Guide, 2006. http://prod.
library.utoronto.ca:8090/datalib/codebooks/cstdli/cchs/cycle3_1/
Documentation/GUIDE_E.pdf.
36. Armstrong K, Moye E, Williams S et al. Screening mammography in women 40–49 years of age: a systematic review for the
American College of Physicians. Ann Intern Med
2007;146:516 –26.
37. Kerlikowske K, Grady D, Rubin SM et al. Efficacy of screening
mammography. JAMA 1995;273:149 –54.
38. U.S 2000 Cancer Mortality. http://www.cdc.gov/nchs/data/
dvs/table210.pdf (15 December 2008, date last accessed).
Page 9 of 10
Downloaded from by guest on March 6, 2016
11. USPSTF (United States Preventive Services Task Force).
Screening for breast cancer: U.S. Preventive Services Task Force
recommendation statement. Ann Intern Med 2009a;151:716–26.
Kadiyala and Strumpf
39. U.S. 2001 Cancer Mortality. http://www.cdc.gov/nchs/data/
dvs/table210.pdf (15 December 2008, date last accessed).
40. U.S. 2002 Cancer Mortality. http://www.cdc.gov/nchs/data/
dvs/mortfinal2002_work210r.pdf (15 December 2008, date last
accessed).
41. U.S. 2003 Cancer Mortality. http://www.cdc.gov/nchs/data/
statab/Mortfinal2003_worktable210r.pdf (15 December 2008,
date last accessed).
42. U.S. 2004 Cancer Mortality. http://www.cdc.gov/nchs/data/
dvs/mortfinal2004_worktbl210R.pdf (15 December 2008, date
last accessed).
43. Canada 2000 –2004 Mortality. http://dsol-smed.phac-aspc.gc.
ca/dsol-smed/cancer/d_age_e.html (15 December 2008, date
last accessed).
44. Ilic D, O’Connor D, Green S et al. Screening for prostate
cancer: a Cochrane systematic review. Cancer Causes Control
2007;18(3):279 –85.
45. Andriole GL, Grubb RL, Buys SS et al. Mortality results from a
randomized prostate-cancer screening trial. N Engl J Med
2009;360:1310 – 19.
46. Schroder FH et al. Screening and prostate cancer mortality in a
randomized European study. N Engl J Med 2009;360:1320 – 28.
47. Telesca D, Etzioni R, Gulati R. Estimating lead time and overdiagnosis associated with PSA screening from Prostate Cancer
Incidence Trends. Biometrics 2008;64:10–19.
48. Mandelblatt J, Saha S, Teutsch S et al. The cost effectiveness of
screening mammography beyond age 65 years: a systematic
review for the U.S. Preventive Services Task Fore. Ann Intern
Med 2003;139:835–43.
49. Moayyedi P, Tepper J, Hilsden R et al. ‘International comparisons of manpower in gastroenterology’. Am J Gastroenterol
2007;102:478 –81.
50. Hilsden R, McGregor E, Murray A et al. Colorectal Cancer
Screening: practices and attitudes of gastroenterologists, internists and surgeons. Can J Surg 2005;48:434 –40.
51. Rathore SS, McGreevey JD, III, Schulman KA et al. Mandated
coverage for cancer-screening services: whose guidelines do
states follow?. Am J Prev Med 2000;19:71 –8.
52. McGregor S, Hilsden R, Yang H et al. Physician barriers to
population-based, fecal occult blood test-based cancer screening
programs
for average-patients.
Can
J
Gastroenterol
2010;24:359 –64.
53. Kadiyala S, Miller G. Managed care and prevention: the physician selection hypothesis. Working Paper.
Downloaded from by guest on March 6, 2016
Page 10 of 10