A Twin Study of Attention-Deficit/Hyperactivity Disorder Dimensions
advertisement

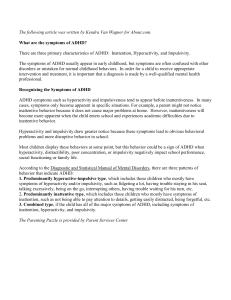
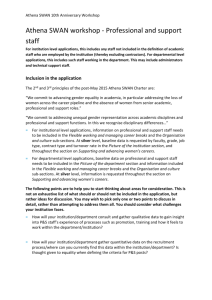
A Twin Study of Attention-Deficit/Hyperactivity Disorder Dimensions Rated by the Strengths and Weaknesses of ADHD-Symptoms and Normal-Behavior (SWAN) Scale David A. Hay, Kellie S. Bennett, Florence Levy, Joseph Sergeant, and James Swanson Background: When symptom rating scales are used in the general population, there is severe skewness, with many individuals having no symptoms. While this has major implications for genetic designs that require extremely discordant and concordant (EDAC) siblings, little is known of the genetics of scales which seek to differentiate within the “no ADHD symptom” group. Methods: Parents of Australian twins completed two attention-deficit/hyperactivity disorder (ADHD) questionnaires, the Australian Twin Behaviour Rating Scale (ATBRS), based on conventional DSM-IV symptom scores, and the Strengths and Weaknesses of ADHD-Symptoms and Normal-Behavior (SWAN) scale, which includes above-average performance on attention and activity. The two scales were compared in two age groups of same-sex twins, 528 pairs aged 6 to 9 and 488 pairs aged 12 to 20. Results: Parents reported higher levels of activity and attention in their twins when reporting using the SWAN scale than when using the ATBRS, and while the monozygotic (MZ) correlations were similar on both scales, the dizygotic (DZ) correlations were consistently higher on the SWAN. On DSM-IV based scales, parents exaggerated differences within those sibling pairs in the “with few ADHD symptoms” category. Conclusions: The SWAN may provide a more realistic description of the ADHD phenotype for the selection of twin and sibling pairs for genetic analysis. Key Words: ADHD, EDAC, genetic analysis, SWAN, symptom rating scales, twins A ttention-deficit/hyperactivity disorder (ADHD) is one of the most common psychiatric disorders in childhood. Graetz et al (2001) surveyed 3597 Australian children and adolescents (6 to 17 years of age) and found that approximately 7.5% of the group sampled had ADHD. Attention-deficit/hyperactivity disorder is defined by elevated levels of inattention and/or hyperactive and impulsive behavior, and the DSM-IV (American Psychiatric Association 1994) recognizes three distinct subtypes within ADHD, the inattentive, hyperactive-impulsive, and combined forms. Graetz et al (2001) found that the inattentive subtype of ADHD was more commonly identified than the hyperactive-impulsive or combined subtypes. Many twin studies (reviewed in Bennett et al, in press) indicate the very substantial genetic component to ADHD. However, there has been some questioning of whether the DSM-IV subtypes are the most realistic approach to ADHD for the purposes of genetic analyses, and one alternative proposed is that of empirically based latent classes (Todd 2000). Such latent classes have proved robust at both the phenotypic (Rasmussen et al 2002) and genetic (Rasmussen et al 2004) levels across Missouri and Australian twin studies where the families were From the School of Psychology (DAH, KSB), Curtin University of Technology, Perth, Western Australia; School of Psychiatry (FL), University of New South Wales, Sydney, New South Wales, Australia; Department of Clinical Neuropsychology (JSe), Vrije Universiteit, Amsterdam, The Netherlands; and Child Development Center (JSw), University of California, Irvine, California. Address reprint requests to David A. Hay, Ph.D., School of Psychology, Curtin University of Technology, GPO Box U 1987, Perth 6845, Western Australia; E-mail: d.hay@curtin.edu.au. Received December 12, 2005; revised April 10, 2006; accepted April 13, 2006. 0006-3223/07/$32.00 doi:10.1016/j.biopsych.2006.04.040 identified and assessed in very different ways by telephone interview and rating scale, respectively. But there is a much broader issue for genetic studies than just the DSM-IV classification of symptoms. Whether assessed by rating scales or interview, most scales measuring ADHD are based on the 18-item diagnostic criteria of the DSM-IV (Murphy and Adler 2004). Such scales assess ADHD using a three-, four-, or five-point scale to rate symptom severity from, for example, 0 ⫽ never or not at all to 3 ⫽ symptom occurs very often. In a general population, most people will have a low score on many of the items, indicating that they have low or no attention problems. If, as described by Levy et al (1997), ADHD comprises a continuous dimension of behavior, then it is likely that some individuals will actually be performing better than average on attention behaviors. Therefore, the use of such rating systems can result in limited (and skewed) data about individuals who are considered to be nonaffected by ADHD, as they are all assigned the same score of 0. This has major implications for molecular genetic studies of ADHD and other behaviors. Increasingly, genetic studies of behavior are selecting sibling pairs using the Extreme Discordant and Concordant (EDAC) design to maximize power to detect linkage (Kirk et al 2000). While concordant affected pairs are easily identified using conventional DSM-IV scales, the ability to define concordant unaffected pairs and extremely discordant pairs will be limited. The same problem goes for association studies. For example, in their study of selection strategies for quantitative trait locus (QTL) mapping in pooled DNA samples, Jawaid et al (2002) demonstrated the most effective comparison was of the top 27% with the bottom 27% of the sample. There are many examples in ADHD (including the present study; Table 1) where much more than 27% of a population sample will have a score of 0. Swanson et al (2005) developed the Strengths and Weaknesses of ADHD-Symptoms and Normal-Behavior (SWAN) scale BIOL PSYCHIATRY 2007;61:700 –705 © 2007 Society of Biological Psychiatry BIOL PSYCHIATRY 2007;61:700 –705 701 D.A. Hay et al Table 1. Monozygotic and Dizygotic Twins Mean Scores in Two Age Groups on the Australian Twin Behaviour Rating Scale and Strengths and Weaknesses of ADHD-Symptoms and Normal-Behavior Rating Scale ATBRS (Range 0 to 3) Younger Age Group MZ DZ Older Age Group MZ DZ SWAN (Range ⫺3 to ⫹3) SWAN Recoded (Range 0 to 3) Inattention Hyperactivity-Impulsivity Inattention Hyperactivity-Impulsivity Inattention Hyperactivity-Impulsivity .63 (.54) .66 (.58) .75 (.46) .76 (.49) ⫺.50 (.89) ⫺.50 (.93) ⫺.53 (.86) ⫺.52 (.84) .12 (.40) .14 (.44) .08 (.35) .09 (.34) .65 (.62) .65 (.61) .46 (.54) .44 (.51) ⫺.71 (1.17) ⫺.64 (1.15) ⫺.86 (1.17) ⫺.75 (1.12) .16 (.47) .18 (.53) .11 (.38) .10 (.40) ATBRS, Australian Twin Behaviour Rating Scale; SWAN, Strengths and Weaknesses of ADHD-Symptoms and Normal-Behavior; MZ, monozygotic; DZ, dizygotic. to help overcome the limitations identified in the earlier rating scales of ADHD. While also based on the 18 ADHD items in the DSM-IV (American Psychiatric Association 1994), the SWAN was designed to measure a wider range of population variation by extending the four-point rating scale to seven points, using ⫺3 ⫽ far above average to ⫹3 ⫽ far below average in severity. This extended rating system allows reporting of areas where individuals perform well above average, as well as areas where they are struggling. Extending the range of responses results in additional data on individuals who are nonaffected by ADHD and does not truncate the data. Therefore, the full range of behavior in the general population is measured. This study aims to investigate the genetic utility of the SWAN by comparing twin data from the SWAN to that of a traditional four-point scale for the assessment of DSM-IV ADHD, the Australian Twin Behaviour Rating Scale (ATBRS). same-sex twins and complete data are analyzed in the current study. Forty-nine percent of the sample was male. Approximately 60% of this group were MZ twin pairs and 40% were DZ twin pairs. The slightly lower rate of DZ twins in this older sample is consistent with MacFarlane and Blondel (2005), who reported there has been a marked increase in DZ twin rates since the 1980s and only a small increase in the rates of MZ twins. Methods and Materials Assessment of ADHD The data on ADHD were collected by mailed questionnaires sent to parents for completion. Parents were asked to provide information on the behavior of their twins and similar-aged siblings, though the latter are not analyzed here. The two ADHD scales were the ATBRS and the SWAN. The Australian Twin Behaviour Rating Scale is based on the DSM-IV criteria for the diagnosis of ADHD. The relationship of this measure to diagnosis of ADHD by formal psychiatric interview has been described in Levy et al (1997, 2005). More discussion of the scale and its genetics can be found in Levy et al (2001). It contains 18 items measuring ADHD behaviors, which ask a parent to rate their child’s behavior on a four-point scale from “never” to “very much or very often.” For example, each parent was asked to answer the following about their children: “Has trouble following through on instructions and doesn’t finish schoolwork, chores or duties?” Parents indicated their response as 0 ⫽ not at all, 1 ⫽ just a little or sometimes, 2 ⫽ pretty much or often, or 3 ⫽ very much or very often. The individual’s total score on the nine inattention and nine hyperactivity-impulsivity items were then averaged to range from 0 to 3, with a higher score indicating a higher level of ADHD symptoms. Previous comparison with interview data indicate this questionnaire provides a more conservative symptom score, with parents identifying more ADHD problems at interview (Levy et al 1997). The Strengths and Weaknesses of ADHD-Symptoms and Normal-Behavior scale contains 18 reworded items to measure ADHD. Based on the previous Swanson, Nolan, and Pelham (SNAP) rating scale (Swanson 1992), items were reworded from the categorical approach of ATBRS (This child: “Has trouble following through on instructions and doesn’t finish schoolwork, Two different-aged samples of Australian twins were selected to investigate differences between the two scales of ADHD, given indications (Hay et al 2004) that there may be differences in the genetic determinants of ADHD during development. Both samples came from the Australian Twin ADHD Project (ATAP) described in Levy and Hay (2001). This research was approved both by the Curtin University Human Research Ethics Committee and by the Australian Twin Registry (ATR). Younger Age Group In 2001, a cohort of 1042 families were approached through the Australian Twin Registry. Of these, 707 families completed the ATBRS and the SWAN rating scale of ADHD. The data from 528 consenting families with same-sex twins are analyzed in the current article. Opposite-sex pairs were excluded to avoid complications of modeling around the gender difference in symptom number (Levy et al 1996; Rhee et al 2001). Referred to as the younger age group, these families had twins aged between 6 and 9 years (mean age ⫽ 7.6 years, SD ⫽ .91). There were approximately equal numbers of male and female twin pairs (262 and 266 pairs, respectively) in the sample with 52% being monozygotic (MZ) twin pairs and 48% being dizygotic (DZ) twin pairs. Older Age Group In 1999, data were collected from 887 twin pairs aged 12 to 20 years (mean age ⫽ 15.2 years, SD ⫽ 2.54), the older age group. These were the initial ATAP cohort, studied from 1991 when all 4- to 12-year-old twin pairs in the Australian Twin Registry were screened (Levy et al 1996). The data from 488 families with Assessment of Zygosity Zygosity was established using discriminant function analysis based on a questionnaire by Cohen et al (1975). This scale had six questions on similarity of features and six questions on frequency of confusion by the mother. There was individual follow-up where ambiguity remained. A more detailed description of this scale can be found in Levy et al (1997) and Hay et al (2001). www.sobp.org/journal 702 BIOL PSYCHIATRY 2007;61:700 –705 The analyses are based on the dimensional constructs of inattention and hyperactivity-impulsivity to illustrate the differences between the ATBRS and the SWAN, while not addressing the issue of the DSM-IV defined subtypes. Comparison Between the ATBRS and SWAN Figure 1 shows the inattentive ratings from children in the younger age group and typifies the differences between the ATBRS and the SWAN. The majority of the ATBRS scores cluster around .0 to .5. As well as being highly skewed (1.387), there is high kurtosis (2.302), indicating that not only are there many values clustered near the center of the distribution but there are fewer scores than expected in the “affected” part of the distribution. On the SWAN scale, scores range from ⫺3 to ⫹3 and have a distribution approximating normality with much lower skew and kurtosis scores (⫺.063 and .371, respectively). This illustrates the extent of data lost when the truncated rating scores (0 to 3) are used to measure ADHD. To further demonstrate this in a genetically informative context, Figures 2A and 2B show scatterplots of scores of DZ twins in the older age group on the inattention scale of the ATBRS and SWAN scales. The highlighted section in Figure 2B indicates the quadrant which is the focus when the 0 to 3 rating scale of the ATBRS is used. Twin 2 Inattention (0 to +3) Results (A) 3 2 1 0 0 1 2 3 Twin 1 Inattention (0 to 3) (B) 3 2 Twin 2 Inattention (-3 to +3) chores or duties?”) to a dimensional approach (Does this child: “Follow through on instructions and finish school work or chores?”). On the SWAN scale, parents rated items on a sevenpoint scale (⫺3 ⫽ far above average; ⫺2 ⫽ above average; ⫺1 ⫽ somewhat above average; 0 ⫽ average; 1 ⫽ somewhat below average; 2 ⫽ below average; 3 ⫽ far below average) (Swanson et al 2005). An individual’s total score on the inattention and hyperactivity-impulsivity dimensions of the SWAN scale were then averaged to range from ⫺3 to ⫹3, with a high score indicating a higher level of ADHD symptoms or problem behaviors. A negative score on the SWAN scale indicates that the child has better than average attention behaviors. D.A. Hay et al 1 0 -1 -2 -3 -3 -2 -1 0 1 2 3 Twin 1 Inattention (-3 to +3) Figure 2. (A) Scatterplot of inattention in older dizygotic children measured on the ATBRS rating scale. (B) Scatterplot of inattention in older dizygotic children measured on the SWAN rating scale. ATBRS, Australian Twin Behaviour Rating Scale; SWAN, Strengths and Weaknesses of ADHD-Symptoms and Normal-Behavior. Figure 1. Percentage of inattention scores from young children on the ATBRS and SWAN rating scales. ATBRS, Australian Twin Behaviour Rating Scale; SWAN, Strengths and Weaknesses of ADHD-Symptoms and NormalBehavior. www.sobp.org/journal Comparison Between Twins at Two Age Groups on the ATBRS and SWAN Table 1 shows the mean scores of the MZ and DZ twins on both the ATBRS and the SWAN. A higher score indicates that more problem behaviors were reported. There were no significant differences between the MZ and DZ twins on the ATBRS or SWAN scales for any area of ADHD. To allow for more direct comparison between the scores on the ATBRS and the SWAN BIOL PSYCHIATRY 2007;61:700 –705 703 D.A. Hay et al scales, the ⫺3 to 0 categories from the SWAN were collapsed to 0 to match the 0 to ⫹3 scoring system of the ATBRS and labeled “SWAN Recoded.” This recoding was conducted to ensure that the positive wording used in the SWAN was not responsible for the reported findings and to allow for a more direct comparison between the scales in the areas of inattention and hyperactivityimpulsivity. The mean scores on the ATBRS and the SWAN recoded data were compared. On the SWAN recoded scale, the younger age group had significantly lower scores on the inattention (t ⫽ ⫺38.506, p ⬍ .001) and also on the hyperactivity-impulsivity subscales (t ⫽ ⫺50.276 and t ⫽ ⫺22.042, p ⬍ .001, respectively). Lower scores indicate that parents were reporting fewer attention problems in their children on the SWAN. This is more than just due to the positively as well as negatively worded questions in the SWAN scale. As shown in Figure 1, only about half as many children have a score of 1 on the SWAN as on the ATBRS. Comparison Between the Younger and Older Age Groups Data from the two age groups on the ATBRS and the SWAN scale were compared. The younger children had higher scores than the older children on the hyperactivity-impulsivity subscale of ATBRS (F ⫽ 178.88, p ⬍ .001) but not on the ATBRS inattention subscale. The younger children scored higher than the older children on the SWAN for both inattention (F ⫽ 14.87, p ⬍ .001) and hyperactivity-impulsivity (F ⫽ 40.83, p ⬍ .001). Generally, this is consistent with the finding of Graetz et al (2001) that younger children (aged 6 to 12 years) had significantly higher levels of ADHD symptoms than adolescents (aged 13 to 17 years). Genetic Models Table 2 shows the twin-twin correlations for maternal report on both the ATBRS and the SWAN, which form the basis for the genetic analysis of ADHD from the two scales in Table 3. There were only modest differences in correlations between the genders and the data are combined across girls and boys to maximize the sample size. Using the conventional formula (Hay 1985) of h2 ⫽ 2(rmz ⫺ rdz), the heritability on the ATBRS for younger children was .96 for inattention and .57 for hyperactivity-impulsivity, similar to those reported by Thapar et al (2000) and our previous Australian Twin Registry studies. However, on the SWAN scale, the heritability for inattention in younger children was .61 and for hyperactivity-impulsivity only .42, due to much higher DZ correlations. Such a large DZ correlation (.7) has not been described before (Thapar et al 2000) and seems specific to the SWAN scale. Similar correlations and heritabilities for the older children were also found in the hyperactivity- impulsivity scale of the SWAN for MZ and DZ twins (.74 and .30, respectively). This difference is not specific to the ⫺3 to ⫹3 scale. On the SWAN recoded scale, the MZ correlations were little changed, but the DZ correlations all were higher, though not always significantly. Table 3 shows the univariate genetic modeling of inattention and hyperactivity-impulsivity for both younger and older children on the ATBRS and the SWAN. The usual procedure for model fitting is based around an additive genetic-common environment-unique environment (ACE) model. Estimates of the effects of each are derived from the model and the chi-square and root mean square error of approximation (RMSEA) plus Akaike’s information criterion (AIC) used to compare the alternative hypothesized models. With enough degrees of freedom, more complex models can be fitted, including such issues as sibling interactions, the “b” component, in one subscale of Table 3. Prelis 2 (Scientific Software International, Chicago, Illinois) (Jöreskog and Sörbom 1993) was used to calculate polychoric correlations between scores, and the computer program MX (Neale et al 1999; Virginia Commonwealth University, Richmond, Virginia) was used for the subsequent model fitting to these correlations. The analysis begins by comparing the ACE model with the submodels AE and CE. Under the principle of parsimony, if the submodel cannot be rejected, then it is used in preference to the ACE model. The results of these analyses indicate strong genetic influences (A) and weak common environmental influences (C) on inattention in the older children on both the ATBRS and the SWAN. Data from the ATBRS show no contribution of C in young children. Instead, the correlation of the DZ twins was so much less than half the MZ correlation on the ATBRS, the best model was one which included a “b” (contrast) parameter. That is, the more one child was perceived by the rater (usually the mother in this case) as being inattentive, the more the co-twin was reported as being the opposite. While the AE model was adequate, the addition of the “b” term improved the chi-square and the AIC. Common environment (C) is identified from a DZ correlation that is significantly more than half the MZ correlation (Table 2). While a C term was identified for all but the older children’s inattention scores on the SWAN, the only effect on the ATBRS was for hyperactivity-impulsivity in the younger twins. Discussion The only previous twin study comparison of ADHD rating scales was by Thapar et al (2000). There they focused on the contrast effects of some measures where DZ twin correlations were less than expected, given the MZ values. The one case of a Table 2. Twin-Twin Correlations for Mother’s Report on Australian Twin Behaviour Rating Scale and Strengths and Weaknesses of ADHD-Symptoms and Normal-Behavior Rating Scale ATBRS (Range 0 to 3) Younger Age Group MZ DZ Older Age Group MZ DZ SWAN (Range ⫺3 to ⫹3) Inattention Hyperactivity-Impulsivity Inattention Hyperactivity-Impulsivity .797 .317 .846 .559 .810 .503 .910 .701 .799 .384 .843 .369 .871 .502 .938 .786 ATBRS, Australian Twin Behaviour Rating Scale; SWAN, Strengths and Weaknesses of ADHD-Symptoms and Normal-Behavior; MZ, monozygotic twins; DZ, dizygotic twins. www.sobp.org/journal 704 BIOL PSYCHIATRY 2007;61:700 –705 D.A. Hay et al Table 3. Univariate Analysis of Inattention and Hyperactivity-Impulsivity for Young and Older Children on the Australian Twin Behaviour Rating Scale and Strengths and Weaknesses of ADHD-Symptoms and Normal-Behavior Rating Scale Younger Age Group ATBRS (Range ⫺0 to ⫹3) Inattention Hyp-Imp SWAN (Range ⫺3 to ⫹3) Inattention Hyp-Imp Older Age Group ATBRS (Range ⫺0 to ⫹3) Inattention Hyp-Imp SWAN (Range ⫺3 to ⫹3) Inattention Hyp-Imp Model 2 df p a2 c2 e2 RMSEA AIC ACE AE CE AE ⫹ b ACE AE CE .154 .154 189.871 .01 0 38.670 175.138 3 4 4 3 3 4 4 .985 .997 0 1 1 0 0 .90 .90 — .91 .47 .94 — ⬍.001 — .68 — .48 — .84 .10 .10 .32 .09 .05 .05 .16 0 0 .407 0 0 .133 .390 ⫺5.846 ⫺7.846 181.871 ⫺5.990 ⫺6.0 30.670 167.138 ACE AE CE ACE AE CE 0 8.712 48.532 0 52.652 531.683 3 4 4 3 4 4 1 .069 0 1 0 0 .53 .81 — .46 .99 — .28 — .68 .53 — .88 .19 .19 .32 .01 .01 .12 0 .057 .205 0 .157 .651 ⫺6.0 .712 40.532 ⫺6.0 44.652 523.683 ACE AE CE ACE AE CE 0 2.131 121.624 0 3.032 199.583 3 4 4 3 4 4 1 .712 0 1 .552 0 .73 .89 — .76 .93 — .16 — .74 .18 — .78 .11 .11 .26 .06 .07 .22 0 .006 .353 0 .025 .448 ⫺6.0 ⫺5.869 113.624 ⫺6.0 ⫺4.968 191.583 ACE AE CE ACE AE CE 0 4.987 113.191 0 70.28 167.503 3 4 4 3 4 4 1 .289 0 1 0 0 .66 .889 — .31 .963 — .23 — .758 .656 — .904 .11 .111 .242 .034 .037 .096 0 .043 .337 0 .216 .407 ⫺6.0 ⫺3.013 105.191 ⫺6.0 62.280 159.503 Bold indicates the best-fitting model; —indicates parameter not used in this model. ATBRS, Australian Twin Behaviour Rating Scale; SWAN, Strengths and Weaknesses of ADHD-Symptoms and Normal-Behavior; A, additive genetic effects; C, common environment effects; E, unique individual environmental effects; Hyp-Imp, hyperactivity-impulsivity; RMSEA, root mean square error of approximation; AIC, Akaike information criterion. contrast effect in the current article was a modest effect on the ATBRS inattention score. Rather, here the most common situation was the converse with the DZ twin correlation being more than half the MZ. This can be explained in three ways. As it occurred for all the hyperactivity-impulsivity scales except the older ATBRS scores, it can be explained as an obvious environmental effect of growing up in the same family. You can hardly be an overactive twin in the home without your co-twin also being influenced by your behavior. An alternative possibility with more implications for measures of ADHD is that parents are rating DZ twins as more similar on the SWAN because they can. In the ATBRS and other conventional DSM-IV based scales, when children are low on ADHD symptoms, then it may be easy to rate one as “0” and one as “1,” whereas there is, in fact, little difference between them. And this may apply on all ADHD measures of multiple family members, whether by questionnaire or interview. A third possibility is that the SWAN is assessing the genetics of activity more than hyperactivity and possibly of attention more than inattention. While this can be examined by bivariate genetic modeling, the sample sizes here were not sufficient to obtain reliable and consistent estimates, though the younger age group is currently being expanded threefold as part of a new research initiative, which will include studies of test-retest reliability and of validity. The www.sobp.org/journal preliminary bivariate analyses suggested more of an overlap than a distinction between the underlying genetic constructs on the ATBRS and the SWAN. Thus, the SWAN may be a more accurate reflection of the “real” ADHD phenotype than the more conventional symptom scales both within the family as shown by the genetic analyses here and perhaps also for individuals. The distribution in Table 1 showed more individuals were classified as having “moderate” levels of ADHD on the SWAN than on the ATBRS, with there being significantly less kurtosis, and the development of age and gender norms for the SWAN is currently underway. The SWAN certainly has significant potential for the identification of extreme phenotypes, but more molecular genetic studies using the SWAN are needed (Cornish et al 2005) to determine its ultimate utility for genetic studies. The research project was funded by a grant (ID 111119) from the National Health & Medical Research Council (NHMRC). The Australian Twin Registry is supported by a grant from the NHMRC administered by The University of Melbourne. American Psychiatric Association (1994): Diagnostic and Statistical Manual of Mental Disorders, 4th ed. Washington, DC: American Psychiatric Press. D.A. Hay et al Bennett KS, Levy F, Hay D (in press): Behaviour genetic approaches to the study of ADHD. In: Fitzgerald M, Bellgrove M, Gill M, editors. Handbook of Attention Deficit Hyperactivity Disorder. John Wiley and Sons. Cohen DJ, Dibble E, Grawe JM, Pollin W (1975): Reliably separating identical from fraternal twins. Arch Gen Psychiatry 32:1371–1375. Cornish KM, Manly T, Savage R, Swanson J, Morisano D, Butler N, et al (2005): Association of the dopamine transporter (DAT1) 10/10-repeat genotype with ADHD symptoms and response inhibition in a general population sample. Mol Psychiatry 10:1–13. Graetz BW, Sawyer MG, Hazell PL, Arney F, Baghurst P (2001): Validity of DSM-IV ADHD subtypes in a nationally representative sample of Australian children and adolescents. J Am Acad Child Adolesc Psychiatry 40: 1410 –1417. Hay DA (1985): Essentials of Behaviour Genetics. Oxford, England: Blackwells. Hay DA, Bennett KS, McStephen M, Rooney R, Levy F (2004): Attentiondeficit hyperactivity disorder in twins: A developmental genetic analysis. Aust J Psychol 56:99 –107. Hay DA, McStephen M, Levy F (2001): Introduction to the genetic analysis of attentional disorders. In: Levy F, Hay D, editors. Attention, Genes and ADHD. East Sussex, England: Brunner-Routledge, 7–34. Jawaid A, Bader JS, Purcell S, Cherny SS, Sham P (2002): Optimal selection strategies for QTL mapping using pooled DNA samples. Eur J Hum Genet 10:125–132. Jöreskog KG, Sörbom D (1993): Prelis 2: A Preprocessor for Lisrel, 2nd ed [computer software]. Chicago: Scientific Software International Inc. Kirk KM, Birley AJ, Statham DJ, Haddon B, Lake RIE, Andrews JG, et al (2000): Anxiety and depression in twin and sib pairs extremely discordant and concordant for neuroticism: Prodromus to a linkage study. Twin Res 3:299 –309. Levy F, Hay D (2001): Attention, Genes and ADHD. East Sussex, England: Brunner-Routledge. Levy F, Hay DA, Bennett KS, McStephen M (2005): Gender differences in ADHD subtype comorbidity. J Am Acad Child Adolesc Psychiatry 44:368 – 376. Levy F, Hay DA, McLaughlin M, Wood C, Waldman ID (1996): Twin-sibling differences in parental reports of ADHD, speech, reading and behaviour problems. J Child Psychol Psychiatry 37:569 –578. BIOL PSYCHIATRY 2007;61:700 –705 705 Levy F, Hay DA, McStephen M, Wood C, Waldman I (1997): ADHD: A category or a continuum? Genetic analysis of a large-scale twin study. J Am Acad Child Adolesc Psychiatry 36:737–744. Levy F, McStephen M, Hay DA (2001): The diagnostic genetics of ADHD symptoms and subtypes. In: Levy F, Hay D, editors. Attention, Genes and ADHD. East Sussex, England: Brunner-Routledge, 35–57. MacFarlane A, Blondel B (2005): Demographic trends in Western European countries. In: Blickstein I, Keith LG, editors. Multiple Pregnancy - Epidemiology, Gestation, and Perinatal Outcome, 2nd ed. London and New York: Taylor & Francis Group, 11–21. Murphy KR, Adler LA (2004): Assessing attention-deficit/hyperactivity disorder in adults: Focus on rating scales. J Clin Psychiatry 65:12–17. Neale MC, Boker SM, Xie G, Maes HH (1999): Mx: Statistical Modeling, 5th ed. Richmond, VA: Department of Psychiatry, Virginia Commonwealth University. Rasmussen E, Neuman R, Heath A, Levy F, Hay D, Todd R (2002): Replication of the latent class structure of attention-deficit/hyperactivity disorder (ADHD) subtypes in a sample of Australian twins. J Child Psychol Psychiatry 43:1018 –1028. Rasmussen ER, Neuman RJ, Heath AC, Levy F, Hay DA, Todd RD (2004): Familial clustering of latent class and DSM-IV defined attention-deficit/ hyperactivity disorder (ADHD) subtypes. J Child Psychol Psychiatry 45: 589 –598. Rhee SH, Waldman ID, Hay DA, Levy F (2001): Aetiology of the sex difference in the prevalence of DSM-III-R attention-deficit hyperactivity disorder: A comparison of two models. In: Levy F, Hay DA, editors. Attention, Genes, and ADHD. East Sussex, England: Brunner-Routledge, 139 –156. Swanson JM (1992): School-Based Assessments and Interventions for ADD Students. Irvine, CA: KC Publishing. Swanson J, Schuck S, Mann M, Carlson C, Hartman K, Sergeant J, et al (2005): Categorical and dimensional definitions and evaluations of symptoms of ADHD: The SNAP and the SWAN Ratings Scales [Draft]. Available at: http://www.adhd.net/SNAP_SWAN.pdf. Accessed May 25, 2005. Thapar A, Harrington R, Ross K, McGuffin P (2000): Does the definition of ADHD affect heritability? J Am Acad Child Adolesc Psychiatry 39:1–12. Todd RD (2000): Genetics of attention deficit/hyperactivity disorder: Are we ready for molecular genetic studies? Am J Med Genet 96:241–243. www.sobp.org/journal