PERRLA Version 6 For APA - NIU College of Education
advertisement

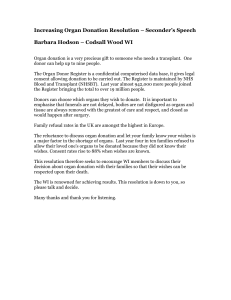
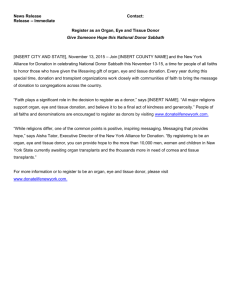
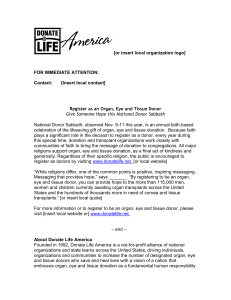
Running head: ORGAN DONATION OCCURRENCE BY ETHNICITY Organ Donation Occurrence by Ethnicity 1 ORGAN DONATION OCCURRENCE BY ETHNICITY 2 Organ Donation Occurrence by Ethnicity Introduction The research problem I will be exploring is the rate of organ donation among ethnicities based on the state population proportion, evaluating for any differences. This topic is important to me as a health care professional, especially in my role as a patient advocate. Organ donation is an important topic nationally, due to the fact that the organ recipient waiting list is growing significantly faster than the rate of organ transplants (Molzahn, Starzomski, & McCormick, 2003). There are currently 113,043 individuals waiting for an organ transplant and this number rises every minute (UNOS: United Network for Organ Sharing website, 2012). In comparison, there were 26,247 transplants, from 12,960 donors, from January to November of 2011 (UNOS: United Network for Organ Sharing website, 2012). Eighteen individuals die every day while waiting for an organ, while 79 individuals receive a life-saving organ each day (U.S. Department of Health & Human Services Organ Donor website, n.d.). These statistics illustrate the deficiency of suitable organs for the large number of possible transplant recipients. As well as those in need of life-saving transplants, numerous individuals receive skin grafts and corneal replacements from organ donors (U.S. Department of Health & Human Services Organ Donor website, n.d.) I am interested in the variation among deceased donor rates across ethnicities because it has been documented that transplants have better outcomes if the donor and recipient are from the same ethnicity (Park, Smith, & Yun, 2009). However, the number of minority donors is smaller than the number of ethnic minorities waiting for a transplant (Park et al., 2009). Compatibility among a donor and a recipient of the same ethnicity is more likely due to blood types and tissue markers that are present within ethnicities (U.S. Department of Health & Human ORGAN DONATION OCCURENCE BY ETHNICITY 3 Services Organ Donor website, n.d.). At this moment, 55.48% of those on the waiting list are from minority populations (U.S. Department of Health & Human Services: Organ Procurement and Transplantation Network website, 2012). In 2011, approximately 34% of donors were minorities (U.S. Department of Health & Human Services: Organ Procurement and Transplantation Network website, 2012). Variation in donation rates due to ethnic differences is important because it may help health care providers and family service coordinators better understand how to enlarge the donor pool. With each new donor, eight lives can be saved (U.S. Department of Health & Human Services Organ Donor website, n.d.). This information could also highlight areas of public education needed. Literature Review In order for a patient to be considered an eligible donor, they must meet the donor criteria. In order to determine if the patient meets donor criteria, health care professionals must contact the organ procurement agency to notify them of an imminent death. The agency will then determine whether a procurement coordinator will be sent to evaluate the patient and discuss donation with the family, or whether the patient does not meet the criteria. According to the Organ Procurement and Transplant Network of the U.S. Department Health and Human Services (2012), an eligible donor is a person age 70 years old or younger who has been legally declared brain dead, but is being maintained on life support. The patient’s heart must still be beating (Delmonico et al., 2005). Also, the patient must not be a medical examiner or coroner case (Delmonico et al., 2005). In addition to this, the patient must be free of active infections, including but not limited to tuberculosis, sepsis, HIV/AIDS, rabies, pneumonia, and Epstein Barr Virus (U.S. Department of Health & Human Services: Organ Procurement and Transplantation Network website, 2012). Certain chronic conditions would also prevent organ donation, ORGAN DONATION OCCURENCE BY ETHNICITY 4 including but not limited to: aplastic anemia, cancer, meningitis, and organ failure. As well as meeting these criteria, the organ procurement agency must obtain consent from the next of kin for organ donation. This illustrates the lengthy process involved in enrolling organ donors. As the number of individuals on the recipient waiting list continues to increase, it is important to educate the public on organ donation, including the process and the outcomes, in order to increase consent rates. In general, it has been documented that next of kin for white patients, younger patients, and male patients were more likely to give consent for organ donation (Siminoff, Gordon, Hewlett, & Arnold, 2001, p. 73). However, data from a 2005 review of donations and transplantations in the U.S. states that minority populations appear to be donating at a rate that is similar to their population proportion (Delmonico et al., 2005). For example, in 2004 African Americans accounted for approximately 13% of the national population and they represented 14% of all donors (Delmonico et al., 2005). However, with more research, it was found that African Americans provided consent for organ donation only 34% of the time, whereas the white population provided consent 61% of the time donation was requested (Delmonico et al., 2005). The same study found that the next of kin for Asian donors provided consent for donation only 30% of the time it was requested (Delmonico et al., 2005). Due to the stringent criteria, only 49% of potential white donors actually became organ donors, which is significantly higher than the compared minority populations (Delmonico et al., 2005). Only 25% of potential African American donors and 23% of the potential Asian donors actually donated at least one organ for transplant (Delmonico et al., 2005). With the limited number of eligible donors, it becomes even more important to increase consent rates. ORGAN DONATION OCCURENCE BY ETHNICITY 5 While researching this topic I discovered that certain ethnicities have a higher demand for organs due to the prevalence of certain conditions within their population (U.S. Department of Health & Human Services Organ Donor website, n.d.). For instance, African Americans tend to have high rates of hypertension and diabetes, both of which can lead to chronic renal failure necessitating a kidney transplant (U.S. Department of Health & Human Services Organ Donor website, n.d.). Hispanic individuals are more likely to suffer from obesity, diabetes, and hypertension, increasing their risk of organ failure (U.S. Department of Health and Human Services: The Office of Minority Health, 2012). Hispanic men and women are more likely than their non-Hispanic counterparts to have chronic liver disease and to die from chronic liver disease (U.S. Department of Health and Human Services: The Office of Minority Health, 2012). There may be other factors contributing to differences within and between ethnicities. It is important to understand these related factors. It has been found that individuals with higher levels of education are more likely to support organ donation than those with less education (Park et al., 2009). Also, life experiences can have an effect on an individual’s perception of organ donation and their willingness to register as a donor. Cultural differences may account for some discrepancy between ethnicities, such as a misunderstanding of their religious beliefs and obligations (Delmonico et al., 2005). It should be noted however, that the majority of organized religions have issued statements in support of organ donation (Molzahn et al., 2003). Nevertheless, it has been documented that some cultures view cremation and organ donation as damaging a body that should remain intact, while other cultures do not accept brain death which prevents them from consenting to donate a loved one’s organs (Molzahn et al., 2003). Another reason that could contribute to the discrepancy of organ donation rates is a fear or mistrust of the medical system (Delmonico et al., 2005). It has been found that some ORGAN DONATION OCCURENCE BY ETHNICITY 6 individuals fear that they or a loved one will be pronounced dead prematurely if they have consented to organ donation or have filled out a donor registration card (Delmonico et al., 2005). In support of this finding, those with higher education levels have been found to sign the donor registration card more frequently than those with less education, as well as whites signing their donor cards more frequently than their African American and Hispanic counterparts (Rubens, 1996). These misconceptions may play a large role in the differences among donation and consent rates. It has also been found that many individuals do not understand the process of organ donation and transplantation, specifically what it means for their loved one (Delmonico et al., 2005). This lack of knowledge prevents consents for donation and causes unease among the public (Delmonico et al., 2005). Methodology The ethnic populations identified are: White, Black, Hispanic, Asian, American Indian/ Alaska Native, Pacific Islander, and Multiracial. I collected Asian, American Indian/Alaska Native, Pacific Islander, and Multiracial into one category due to the limited number of donors from these ethnicities. Unfortunately, this will limit the specificity in regard to these populations. I gathered data from 2010, which provides me with the most recent, published data available from the U.S. Department of Health and Human Services as well as the United States Census Bureau. The data was reported by state and within state by ethnicity. Unfortunately, not every state in the United States of America is represented. The Organ Procurement and Transplantation Network did not include data for Alaska, Delaware, Idaho, Maine, Montana, New Hampshire, Rhode Island, South Dakota, Vermont, West Virginia, and Wyoming. It should be noted that each of these states does have an organ donor program. Puerto Rico and the District of Columbia are included in the sample. There are in total 40 states and territories ORGAN DONATION OCCURENCE BY ETHNICITY 7 accounted for. I found my data from the U.S. Department of Health and Human Services: Organ Procurement and Transplantation Network (OPTN) website. I have also gathered the most recent census data for the states involved in the data from the OPTN (United States Census Bureau website, n.d.). The census data provided me with the ethnic group populations within states. Initially I was evaluating a difference in the number of donors from each ethnicity. This did show a significant difference in the number of donors from each ethnicity and a power level of 1.000. A power of 1.000 means we have completely controlled for Type II error and that 100% of the time we will correctly reject a false null hypothesis and identify a true relationship. The effect size of this test was .38, which shorts a large effect size. This means that 38% of the variance in the dependent variable can be accounted for by having ethnicity as the independent variable. Also, 62% of the variance cannot be accounted for by having ethnicity as the independent variable, meaning there are other influencing factors. Our power and effect size are consistent, indicating that we are correct in rejecting the null hypothesis and stating that the compared means are not all equal. Since, this shows statistical significance and the Levene’s Test shows that we cannot assume that the population variances are equal (p < .05 at < .001), I ran the Tamhane and Games-Howell post-hoc tests. These post-hoc tests showed significant differences in the donor means between all four groups, except between Black and Hispanic populations. However, this is not an accurate portrayal of the donation rates due to variations in ethnic populations. As you can see from the error bar charts, the donation rates appear to correspond to the population size. ORGAN DONATION OCCURENCE BY ETHNICITY 8 Levene's Test of Equality of Error Variancesa Dependent Variable: Donors F 25.016 df1 df2 3 Sig. 156 .000 Tests of Between-Subjects Effects Dependent Variable Donors Source Corrected Model Intercept Ethnicity Error Total Corrected Total Partial Eta Squared .391 .390 .391 Type III Sum of Squares 1324367.075a 1315150.225 1324367.075 2058882.700 4698400.000 3383249.775 Noncent. Parameter 100.346 99.648 100.346 Sig. df 3 1 3 156 160 159 Mean Square 441455.692 1315150.225 441455.692 13197.966 Observed Powerb 1.000 1.000 1.000 R Squared = .391 (Adjusted R Squared = .380)a Computed using alpha = b F 33.449 99.648 33.449 .000 .000 .000 ORGAN DONATION OCCURENCE BY ETHNICITY 9 ORGAN DONATION OCCURENCE BY ETHNICITY 10 Due to the inaccuracy of those findings in regard to the United States population, I am now using the collected data to evaluate the relationship between ethnicity and organ donation occurrence, in proportion to the population size within each state. I will use each state’s data to compare each ethnicity as a whole. In order to determine the proportion of organ donors to the ethnic group’s population, I divided the number of organ donors by that population for each state. This will provide me with more accurate and less biased results. By using data from each state represented, I was able to get descriptive statistics of each ethnicity for an overall perspective. The dependent variable in my study is the number of donations in proportion to population representation. My dependent variable is interval level data. The independent variable in my study is the ethnic groups, which is nominal data. For a deceased to be counted as a donor, they had to have donated at least one solid organ (U.S. Department of Health & Human Services: Organ Procurement and Transplantation Network website, 2012). There was no sampling used for this study. Organ donation and transplantations records are complete and all relevant data was used. Therefore, I am studying the population of donors. Analysis To analyze my data, I will run a one-way analysis of variance (ANOVA). The ANOVA test uses sample data to generate assumptions about the population of interest (Gravetter & Wallnau, 2011). I have chosen to run an ANOVA because I am going to be evaluating the differences in the means for more than two groups of independent variables. I will be discussing the mean differences of four independent variables and the ANOVA is the test that allows me to do this. The result of the ANOVA test will indicate whether or not there is a significant ORGAN DONATION OCCURENCE BY ETHNICITY 11 difference in the mean donation rates among the ethnicities specified (Gravetter & Wallnau, 2011). In other words, the null and alternative hypotheses for an ANOVA test are as follows: Ho: All of the means are equal (μ1 = μ2 = μ3 = μ4) For my model Ho is: All ethnicities have the same rate of donation per population proportion. H1: At least one of the means varies from the others. For my model H1 is: All ethnicities do not have the same rate of donation per population proportion. The independent variable, or factor, is ethnicity, which is broken down into four levels: 1 = White 2 = Black 3 = Hispanic 4 = Asian, American Indian/Alaska Native, Pacific Islander, and Multiracial, which have been grouped together. Each ethnic group’s data is provided for each of the forty territories (n), providing a balanced design with a total of 160 samples (N). However, the population and donor statistics within these states vary greatly, accounting for a poor skewness and kurtosis. When running an ANOVA test, it is important to remember the assumptions for this test. The assumptions are: 1. The population you are study should be normally distributed. a. However, my data does not meet this assumption. The skewness and kurtosis are outside of the -2.00 to 2.00 range for each population. The data for each ethnic grouping is positively skewed and leptokurtic. I was able to determine this by the descriptive statistics output as well as by assessing the graphs. Also, in three out of the four groups, the standard deviation exceeds the mean; this highlights the large variation in donation rates within ethnicities and within territories. When analyzing the results from the ANOVA test, I will have to take into consideration the violation of this assumption. Between-Subjects Factors Value Label N 1 White 40 2 Black 40 Ethnicity 3 Hispanic 40 Asian/American Indian/Alaska Native/Pacific 4 40 Islander/Multiracial ORGAN DONATION OCCURENCE BY ETHNICITY 12 This boxplot shows that there are many outliers present within this population. Due to the number of outliers and the consistency among the groups, I have decided to leave the outliers in the data. The outliers highlight the variation in ethnic representation within states as well as donation rates. I believe that removing the outliers would corrupt the data. The overall donation rate in proportion to population is fairly consistent among the four ethnic groupings, evidenced by the boxplot size and shape. Lastly, all of the boxplots overlap, indicating nearly equal donation rates. ORGAN DONATION OCCURENCE BY ETHNICITY 13 Statistics Ethnicity Ethnicity N White Valid Missing Mean Std. Deviation Std. Error of Skewness Std. Error of Kurtosis Skewness 40 0 1.00 .000 .374 .733 Kurtosis N Black Hispanic Asian/American Indian/Alaska Native/Pacific Islander/Multiracial Valid Missing Mean Std. Deviation Std. Error of Skewness Std. Error of Kurtosis Skewness Kurtosis Valid N Missing Mean Std. Deviation Std. Error of Skewness Std. Error of Kurtosis Skewness Kurtosis Valid N Missing Mean Std. Deviation Std. Error of Skewness Std. Error of Kurtosis Skewness Kurtosis Donors Population Proportion 40 0 .0000669177 .00009868177 .374 .733 4.151 40 0 17.184 40 0 .0000549873 .00004991292 .374 .733 4.076 21.332 40 0 .0000491567 .00008107096 .374 .733 3.941 15.281 40 0 4.00 .000 .374 .733 .0000337544 .00007718150 .374 .733 40 0 2.00 .000 .374 .733 40 0 3.00 .000 .374 .733 4.732 23.465 ORGAN DONATION OCCURENCE BY ETHNICITY 14 2. The samples being used were selected randomly. a. In the instance of my test, all available data is being analyzed. In other words, I am analyzing the population of interest. The limited number of deaths that are eligible for donation and that receive consent make this a small population. 3. The data for the dependent variable should be interval level data. a. The dependent variable in my study is the proportion of donors per state population for each ethnicity; this is interval level data. 4. Assumption of Homogeneity of Variances: the population variances are unknown but assumed equal. a. Ho: The population variances are assumed equal. (σ1 = σ2 = σ3 = σ4) b. H1: The population variances are not assumed equal. (σ1 ≠ σ2 ≠ σ3 ≠ σ4) c. This was checked through SPSS for my data. The observed p-value for the Homogeneity of Variances test for my data was .612, which is greater than .05. Therefore, we would fail to reject the null hypothesis and would assume that the variances of the populations are assumed equal. Levene's Test of Equality of Error Variancesa Dependent Variable: DonorsPopulationProportion F df1 df2 .606 3 156 Sig. .612 In the ANOVA test, we use the test statistic F-ratio. The F-ratio is essentially a comparison of the variation among the group means and the variation among the participants within the groups. The F-ratio formula is: F= variance (differences) between sample means . variance (differences) expected with no treatment effect Based on this equation, if the F-value is ≤ 1.0, you would expect not to have statistical significance because there is no difference between your group means. However, if there is a difference between your group means, you would expect your F-value to be > 1.0, indicating that you will have statistical significance (Gravetter & Wallnau, 2011). In other words, if my observed F-value is > 1.0, I would assume that a person’s ethnicity contributes to their decision to consent or not to organ donation. ORGAN DONATION OCCURENCE BY ETHNICITY 15 In order to determine the F-critical value for my model, I need to determine the degrees of freedom. The equation for determining the degrees of freedom used on the F-critical value table is as follows: For the degrees of freedom (df) numerator: df = k (number of groups) – 1 For my study, I have 4 groups (k). df = 4 -1, therefore the numerator df = 3. Degrees of freedom (df) denominator: df = N (sum of sample sizes from all populations) – k (number of groups) For my study, I have a total of 160 samples (N). df = 160 – 4, therefore the denominator df = 156. I then use these finding and the F Distribution table (Gravetter & Wallnau, 2011) to determine my F-critical value for a p-value of .05. Based on the table, the F-critical value for my ANOVA is 2.66. When I ran my ANOVA, I found that my observed test statistic (F-ratio) was 1.228 and my observed p-value was .302. Based on these findings, we would retain the null hypothesis. This means that there is not a difference among the donation rates per population proportion of the identified ethnicities. Our decision to retain the null hypothesis is supported by graphs printed previously and below. The boxplots and error bars show overlapping values, indicating similar donation rates. The observed F-ratio of 1.228, is very close to 1.0, which is predictive of retaining the null hypothesis. The power of my model was found to be .324, which is very small. This indicates that only 32.4% of the time, we will correctly reject a false null hypothesis. In other words, only 32.4% of the time will we correctly identify a true relationship between the variables. Also, the probability of committing a Type II error in this test is large at 67.6%. The “bad error” or the error of the dependent variable in this model is 6.190-9 (.000000006) donors per population proportion. Due to the lack of statistical significance in this test, post-hoc tests are not necessary. ORGAN DONATION OCCURENCE BY ETHNICITY 16 Tests of Between-Subjects Effects Dependent Variable Type III Sum of Source Squares df Mean Square F Sig. a 3 7.599E-009 1.228 .302 Intercept 4.195E-007 1 4.195E-007 67.773 .000 Ethnicity 2.280E-008 3 7.599E-009 1.228 .302 Error 9.656E-007 156 6.190E-009 Total 1.408E-006 160 Corrected Total 9.884E-007 159 Corrected Model 2.280E-008 Partial Eta Noncent. Squared Parameter Observed Power b .023 3.683 .324 .303 67.773 1.000 .023 3.683 .324 R Squared = .023 (Adjusted R Squared = .004)a Computed using alpha =b ORGAN DONATION OCCURENCE BY ETHNICITY 17 Conclusion The lack of statistical significance within this model could be due to many factors. For example, the standard deviations for three out of the four populations exceeded the corresponding means. The one group in which this did not occur, still had a standard deviation that was very close to the mean. This highlights the variability of donation rates within states and the variation of population sizes within states. Also, the power of this model is very poor at .324. Therefore, it did not adequately control for Type II error. The large variation in the ethnic populations makes it more difficult to compare them. This is also true for the vast differences in the number of donors for each ethnicity within and between states. There were many states in which there were zero donors for at least one ethnic group. These aspects of the data are highlighted in the skewness and kurtosis. I combined the following populations due to their limited numbers even though it would compromise the specificity of my study: Asian, American Indian, Alaska Native, Pacific Islander, and Multiracial. I had hoped this would help improve the skewness and kurtosis within my study. The skewness and kurtosis for each group was outside of the acceptable ranges of -2.00 to 2.00. This means that the data values are not normally distributed on both sides of the mean, which was confirmed by our histograms for each population. Therefore, even though the population size was large, at 160 total, our data did not meet all of the assumptions for an ANOVA. Another limitation to note at this point is that we do not have data regarding the number of eligible donor deaths and the ethnicity of those potential donors. I requested this data from the Organ Procurement and Transplantation Network, but received a reply that they do not have this information. If we were able to compare the actual donor rates to the number of eligible donors, we would have a more complete and more accurate portrayal in regards to any discrepancy ORGAN DONATION OCCURENCE BY ETHNICITY 18 between organ donation rates among ethnicities. It is also important to note that the interaction between the donor coordinator, healthcare professionals, and the family members may play a role in the family’s decision on organ donation, among other unknown factors. This is something we cannot control for at this time. Lastly, the target population includes all states in the U.S. The information I was able to find does not include all states; therefore, I will be making an assumption on the entire United States with information from only forty territories. While I expected to find statistically significant findings, I am reassured to see that donation rates are similar across ethnicities. This shows an improvement in the understanding and acceptance of organ donation by all ethnicities. Although the increase in multicultural donation is considerable, it is still significantly less than the number of individuals on the waiting list from the same ethnicities (Tuttle-Newhall et al., 2009). As the number of those on the waiting list for organs continues to grow at a faster rate than the number of consenting donors (U.S. Department of Health & Human Services Organ Donor website, n.d.), we as healthcare professionals and patient advocates need to work with state agencies to continue educating the nation as a whole to increase the number of overall donors. In addition, I would recommend reeducating healthcare professional about the importance of notifying organ procurement agencies of imminent deaths and the importance of this process. Hopefully with these changes we can reduce the number of individuals who die while waiting for organ transplantations. ORGAN DONATION OCCURENCE BY ETHNICITY 19 References Delmonico, F. L., Sheehy, E., Marks, W. H., Baliga, P., McGowan, J. J., & Magee, J. C. (2005, March 10). Organ donation and utilization in the United States, 2004. American Journal of Transplantation, 5, 862-873. doi:10.1111/j.1600-6135.2005.00832.x Gravetter, F. J., & Wallnau, L. B. (2011). Essentials of statistics for the behavioral sciences (7th ed.). Belmont, CA: Wadsworth, Cengage Learning. Molzahn, A. E., Starzomski, R., & McCormick, J. (2003, February). The supply of organs for transplantation: Issues and challenges. Nephrology Nursing Journal, 30(1), 17-28. Park, H. S., Smith, S. W., & Yun, D. (2009). Ethnic differences in intention to enroll in a state organ donor registry and intention to talk with family about organ donation. Health Communication, 24, 647-659. doi:10.1080/10410230903242259 Rubens, A. J. (1996, July). Racial and ethnic differences in students’ attitudes and behavior toward organ donation. Journal of the National Medical Association, 88, 417-421. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2608007/ Siminoff, L. A., Gordon, N., Hewlett, J., & Arnold, R. M. (2001). Factors influencing families’ consent for donation of solid organs for transplantation. Journal of the American Medical Association, 286, 71-77. Retrieved from http://jama.ama-assn.org Tuttle-Newhall, J. E., Krishnan, S. M., Levy, M. F., McBride, V., Orlowski, J. P., & Sung, R. S. (2009). Organ donation and utilization in the United States: 1998-2007. American Journal of Transplantation, 9, 879-893. doi:10.1111/j.1600-6143.2009.02565.x UNOS: United Network for Organ Sharing website. (2012). www.unos.org U.S. Department of Health & Human Services Organ Donor website. (n.d.). www.organdonor.gov ORGAN DONATION OCCURENCE BY ETHNICITY 20 U.S. Department of Health & Human Services: Organ Procurement and Transplantation Network website. (2012). http://optn.transplant.hrsa.gov U.S. Department of Health and Human Services: The Office of Minority Health. (2012). http://minorityhealth.hhs.gov/templates/content.aspx?lvl=3&lvlID=12&ID=7989 United States Census Bureau website. (n.d.). http://2010.census.gov