Ventilatory limitations in chronic obstructive pulmonary disease
advertisement

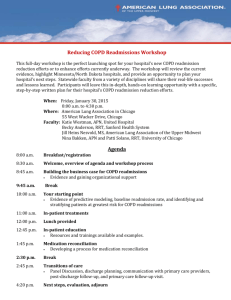
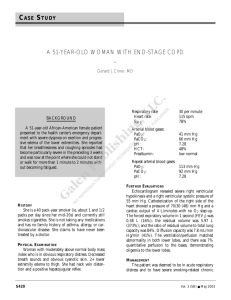
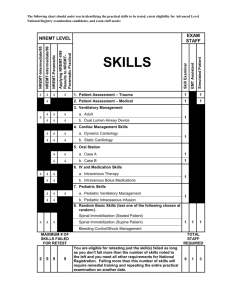
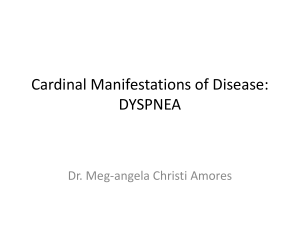
Ventilatory limitations in chronic obstructive pulmonary disease DENIS E. O’DONNELL Departments of Medicine and Physiology, Division of Respiratory and Critical Care Medicine, Queen’s University, Kingston, Ontario, CANADA ABSTRACT O’DONNELL, E. D. Ventilatory limitations in chronic obstructive pulmonary disease. Med. Sci. Sports Exerc., Vol. 33, No. 7, Suppl., pp. S647–S655, 2001. Chronic obstructive pulmonary disease (COPD) is a heterogeneous disorder characterized by dysfunction of the small and large airways, as well as by destruction of the lung parenchyma and vasculature, in highly variable combinations. Breathlessness and exercise intolerance are the most common symptoms in COPD and progress relentlessly as the disease advances. Exercise intolerance is multifactorial, but in more severe disease, ventilatory limitation is often the proximate exercise-limiting event. Multiple factors determine ventilatory limitation and include integrated abnormalities in ventilatory mechanics and ventilatory muscle function as well as increased ventilatory demands (as a result of gas exchange abnormalities) and alterations in the neuroregulatory control of breathing. Despite its heterogeneity, the pathophysiological hallmark of COPD is expiratory flow limitation. When ventilation increases in flow-limited patients during exercise, air trapping is inevitable and causes further dynamic lung hyperinflation (DH) above the already increased resting volumes. DH causes elastic and inspiratory threshold loading of inspiratory muscles already burdened with increased resistive work. It seriously constrains tidal volume expansion during exercise. DH compromises the ability of the inspiratory muscles to generate pressure, and the positive intrathoracic pressures likely contribute to cardiac impairment during exercise. Progressive DH hastens the development of critical ventilatory constraints that limit exercise and, by causing serious neuromechanical uncoupling, contributes importantly to the quality and intensity of breathlessness. The corollary of this is that therapeutic interventions that reduce operational lung volumes during exercise, by improving lung emptying or by reducing ventilatory demand (which delays the rate of DH), result in clinically meaningful improvement of exercise endurance and symptoms in disabled COPD patients. Key Words: DYSPNEA, DYNAMIC HYPERINFLATION, MECHANICS, FLOW–VOLUME LOOPS V entilatory limitation and the associated respiratory discomfort contribute importantly to exercise curtailment in chronic obstructive pulmonary disease (COPD). Our knowledge of the complex interface between ventilatory impairment and exercise intolerance has increased considerably in recent years and is the primary focus of this review. Advances in our ability to evaluate the prevailing ventilatory constraints during exercise, together with the development of reliable methods to assess symptom intensity, have increased our understanding of this impairment– disability interface. These new insights into the nature of ventilatory limitation to exercise will be reviewed, and their implications for the management of the disabled COPD patient will be discussed. abnormalities, 3) peripheral muscle dysfunction, 4) cardiac impairment, 5) exertional symptoms, and 6) any combination of these interdependent factors. The predominant contributory factors to exercise limitation vary among patients with COPD, or indeed, in a given patient over time. The more advanced the disease, the more of these factors come into play in a complex integrative manner. In patients with severe COPD, ventilatory limitation is often the predominant contributor to exercise limitation—that is, exercise is terminated because of the inability to further increase ventilation in the face of increasing metabolic demands. The patient is deemed to have ventilatory limitation if, at the breakpoint of exercise, he or she has reached estimated maximal ventilatory capacity (MVC), while at the same time cardiac and other physiological functions are operating below maximal capacity. In practice, it is difficult to precisely determine if ventilatory limitation is the proximate boundary to exercise performance in a given individual. Attendant respiratory discomfort may limit exercise before “physiological limitation” occurs, and the relative importance of other nonventilatory factors is impossible to quantify with precision. Our assessment of MVC, as estimated from resting spirometry or from brief bursts of voluntary hyperventilation, is inaccurate (1). Prediction of the peak ventilation actually achieved during exercise from maximal voluntary ventilation at rest is problematic because the pattern of ventilatory muscle recruitment, the changes in intrathoracic pressures and respired flows and volumes, and the DETECTION OF VENTILATORY LIMITATION IN COPD Exercise limitation is multifactorial in COPD. Recognized contributory factors include 1) ventilatory limitation because of impaired respiratory system mechanics and ventilatory muscle dysfunction, 2) metabolic and gas exchange 0195-9131/01/3307-0647/$3.00/0 MEDICINE & SCIENCE IN SPORTS & EXERCISE® Copyright © 2001 by the American College of Sports Medicine Received for publication October 2000. Accepted for publication April 2001. S647 extent of dynamic lung hyperinflation are often vastly different under the two conditions (21). Although an increased ratio (0.9) of peak ventilation (VE) to the estimated MVC strongly suggests serious ventilatory constraints, a lower peak VE/MVC ratio (i.e., ⬍0.75) by no means excludes the possibility of significant ventilatory impairment during exercise. Thus, simultaneous analysis of exercise flow–volume loops at the symptom-limited peak of exercise may show marked constraints on flow and volume generation in the presence of an apparent adequate ventilatory reserve, as estimated from the peak VE/MVC ratio (17,21). An alternative approach to the evaluation of the role of ventilatory factors in exercise limitation is to determine the effects of interventions that selectively increase or decrease ventilatory demand or capacity on exercise performance. For example, the addition of hypercapnic stimulation or external dead space to the breathing circuit will increase ventilatory demand (3,18). In this regard, the inability to increase ventilation with earlier attainment of peak VE and premature termination of exercise when an external dead space is added indicates that ventilatory factors likely contributed importantly to poor exercise capacity in the unloaded condition (3). Similarly, we can conclude that ventilatory limitation contributed importantly to exercise intolerance in chronic pulmonary disease; by using an intervention that decreases ventilatory demand and delays peak ventilation (i.e., such as oxygen therapy), we can improve exercise tolerance (36). Studies of how exercise capacity can be increased in patients with COPD that have used therapeutic manipulation of the ventilatory demand– capacity relationship allow us to explore, in a novel manner, the nature of the existing ventilatory constraints to exercise (see below). VENTILATORY MECHANICS IN COPD COPD is a heterogeneous disorder characterized by dysfunction of the small and large airways and by parenchymal and vascular destruction, in highly variable combinations. Although the most obvious physiological defect in COPD is expiratory flow limitation caused by combined reduced lung recoil and airway tethering, as well as intrinsic airway narrowing, the most important mechanical consequence of this is a “restrictive” ventilatory deficit attributable to lung hyperinflation (54,61) (Fig. 1). When expiratory flow limitation reaches a critical level, lung emptying becomes incomplete during resting tidal breathing, and lung volume fails to decline to its natural equilibrium point (i.e., passive functional residual capacity [FRC]). End-expiratory lung volume (EELV), therefore, becomes dynamically and not statically determined and represents a higher resting lung volume than in health (54). In COPD, EELV is a continuous variable that fluctuates widely with rest and activity. When VE increases in flow-limited patients (e.g., during exercise), dynamic EELV (EELVdyn) increases even further above resting values: this is termed dynamic lung hyperinflation (DH) (Fig. 1). By contrast, in healthy, non–flow-limited subjects, EELVdyn may actually decline during the inS648 Official Journal of the American College of Sports Medicine FIGURE 1—In a normal healthy subject and a typical patient with COPD, tidal flow–volume loops at rest and during exercise (peak exercise in COPD compared with exercise at a comparable metabolic load in the age-matched healthy person) are shown in relation to their respective maximal flow–volume loops. creased VE of exercise, particularly in younger individuals (14,19,29) (Fig. 1). This allows tidal volume (VT) expansion within the linear portion of the respiratory system’s pressure–volume relationship where “high end” elastic loading is avoided. Expiratory muscle recruitment and reduced EELVdyn also favorably affect diaphragmatic function in health (14,19,29). Many of these important advantages are lost in COPD patients because of DH. The extent and pattern of DH development in COPD patients is highly variable: the average range of increase in EELVdyn in published series is 0.3 to 0.6 L (53,11,37). However, some patients do not increase EELVdyn during exercise, whereas others show dramatic increases (i.e., ⬎1 L). Patients with a predominant “chronic bronchitis” clinical profile show comparable levels of dynamic hyperinflation during exercise to those with a more “emphysematous” profile. Important determinants of DH include 1) the level of baseline lung hyperinflation, 2) the extent of expiratory flow limitation, 3) ventilatory demand, and 4) breathing pattern for a given ventilation. Although DH serves to maximize tidal expiratory flow rates during exercise, it has serious consequences with respect to dynamic ventilatory mechanics, inspiratory muscle function, respiratory sensation, and probably cardiac function (37) (Table 1). An important mechanical consequence of DH is severe mechanical constraints on VT expansion during exercise: VT is truncated from below by the increasing EELVdyn and constrained from above by the relatively reduced inspiratory reserve volume (IRV) and the total lung capacity (TLC) envelope (61) (Figs. 1 and 2). Thus, at comparable low work rates in COPD patients, dynamic end-inspiratory lung TABLE 1. Negative effects of dynamic hyperinflation during exercise. Restricted tidal volume response to exercise, with tachypnea Increased elastic/threshold loading of the inspiratory muscles Functional inspiratory muscle weakness “Neuromechanical uncoupling” of the respiratory system Increased exertional dyspnea Cardiac impairment Early exercise termination http://www.acsm-msse.org FIGURE 2—Behavior of (A) operational lung volumes, (B) respiratory effort (Pes/PImax), and (D) exertional dyspnea as ventilation increases throughout exercise in normals and COPD. In COPD, tidal volume (VT) takes up a larger proportion of the reduced inspiratory capacity (IC), and the inspiratory reserve volume (IRV) is decreased at any given ventilation—these mechanical constraints on tidal volume expansion are further compounded because of dynamic hyperinflation during exercise. (C) Because of a truncated VT response to exercise, patients with COPD must rely more on increasing breathing frequency (F) to generate increases in ventilation. Adapted from O’Donnell et al. (38) with permission. volume (EILVdyn) and VT/inspiratory capacity (IC) ratios are greatly increased, and the IRV is diminished compared with healthy subjects (Figs. 1 and 2). To increase VE during exercise, such patients must rely on increasing breathing frequency; but this tachypnea, in turn, causes further DH in a vicious cycle (Fig. 2). The behavior of EELV during exercise is usually tracked by serial IC maneuvers (11,37,53). This is a reasonable approach since, to our knowledge, TLC does not change appreciably during exercise in COPD (59). Repeated IC measurements during constant load exercise have recently been shown to be both reproducible and responsive (39). In contrast to health, where IC remains unchanged or actually increases (14,19,29), IC progressively diminishes with increasing levels of exercise in COPD patients (Figs. 1 and 2). The smaller the IC during exercise, the closer VT is positioned to TLC and the upper alinear extreme of the respiratory system’s (combined chest wall and lung) pressure– volume relationships, where there is increased elastic loading of muscles already burdened by increased resistive work. The combined elastic and resistive loads on the ventilatory muscles substantially increase the mechanical work VENTILATORY LIMITATIONS and the oxygen cost of breathing at a given ventilation in COPD compared with health. At a peak exercise VE of approximately 20 L·min⫺1, ventilatory work may approach over 200 J·min⫺1 and respiratory muscle V̇O2 exceeds 300 mL·min⫺1 in COPD (27). Another more recently recognized mechanical consequence of DH is inspiratory threshold loading (ITL) (54). Since in flow-limited patients, inspiration begins before tidal lung emptying is complete, the inspiratory muscles must first counterbalance the combined inward (expiratory) recoil of the lung and chest wall before inspiratory flow is initiated. This phenomenon (i.e., reduced lung emptying) is associated with positive intrapulmonary pressures at the end of quiet expiration (autoPEEP or intrinsic PEEP). The ITL, which may be present at rest in some flow-limited patients with COPD, further increases with exercise and can be substantial (e.g., ⫺6 to ⫺14 cm H2O) and may have important implications for dyspnea causation (30,38). DH alters the length–tension relationship of the inspiratory muscles, particularly the diaphragm, and compromises their ability to generate pressure (20,55–57). Attendant tachypnea and increased velocity of muscle shortening during exercise results in further functional inspiratory muscle weakness (20). Because of weakened inspiratory muscles and the intrinsic mechanical loads already described, tidal inspiratory pressures represent a much higher fraction of their maximal force-generating capacity than in health at a similar work rate or ventilation (20,55–57) (Fig. 2). DH may alter the pattern of ventilatory muscle recruitment to a more inefficient pattern with negative implications for muscle energetics (34). The net effect of DH in COPD is, therefore, that the VT response to increasing exercise is progressively constrained despite inspiratory efforts that approach the maximum: the ratio of effort (i.e., tidal esophageal pressures relative to maximum [Pes/PImax]) to tidal volume response (VT/VC) are thus significantly higher at any given work rate or ventilation in COPD compared with health (38) (Fig. 2). Accelerated dynamic hyperinflation during exercise hastens the onset of critical ventilatory limitation, which in turn leads to premature termination of exercise (Figs. 1 and 2). In flow-limited patients, the degree of resting lung hyperinflation, as reflected by reduced inspiratory capacity, is a powerful predictor of exercise capacity (9,33). In a recent study, the resting IC in conjunction with the FEV1.0/FVC ratio together accounted for 72% of the variance in exercise capacity in a group (n ⫽ 52) of patients with COPD (9). Moreover, it has recently been shown that improvement in resting IC after bronchodilator therapy was the strongest correlate of improved exercise endurance in patients with severe COPD (43). DYNAMIC HYPERINFLATION AND DYSPNEA Dyspnea intensity during exercise has been shown to correlate strongly with measures of dynamic lung hyperinflation (37) (Fig. 3). In a multiple regression analysis with Borg ratings of dyspnea intensity as the dependent variable versus a number of relevant independent physiological Medicine & Science in Sports & Exercise姞 S649 FIGURE 3—The relationship between respiratory effort (Pes/PImax) and the tidal volume response (VT standardized as a % of predicted VC) increases during exercise in patients with COPD (i.e., neuromechanical dissociation). Increasing ventilation and the mechanical load on the respiratory muscles (i.e., dynamic hyperinflation) results in increased elastic recoil and an inspiratory threshold load (ITL). (left panel). Significant interrelationships have been found between dyspnea intensity, neuromechanical dissociation (Pes/VT ratio), and the extent of dynamic lung hyperinflation (EELV) at a standardized level of exercise in COPD (right panel). Adapted from O’Donnell et al. (38) with permission. variables, the change in EILVdyn (expressed as % TLC) during exercise emerged as the strongest independent correlate (r ⫽ 0.63, P ⬍ 0.001) in 23 patients with advanced COPD (average FEV1.0 ⫽ 36% predicted) (37). Change in EELVdyn and change in VT (the components of EILVdyn) emerged as significant contributors to exertional breathlessness and, together with increased breathing frequency, accounted for 61% of the variance in change in exercise dyspnea by Borg ratings (37). A second study showed equally strong correlations between intensity of inspiratory difficulty during exercise and EILVdyn/TLC (r ⫽ 0.69, P ⬍ 0.001) (38). DH gives rise to restrictive ventilatory mechanics and an increased ratio of inspiratory effort to VT response (Figs. 2 and 3). It is not surprising, therefore, that Borg ratings of dyspnea intensity also correlate strongly with this increased effort/displacement ratio (38) (Fig. 3). This increased ratio ultimately reflects increased neuromechanical uncoupling of the respiratory system and may provide a neurophysiological basis for perceived respiratory distress. These studies collectively attest to the importance of DH and its adverse mechanical consequences on dyspnea causation during exercise in COPD patients. Further evidence of the importance of DH in contributing to exertional dyspnea in COPD has come from a number of studies that have shown that dyspnea was effectively ameliorated by interventions that reduced operational lung volumes, either pharmacologically (2,7,39) or surgically (13,32), or that counterbalanced the negative effects of DH on the respiratory muscle (i.e., continuous positive airway pressure (CPAP)) (40,51). GAS EXCHANGE ABNORMALITIES IN COPD Arterial hypoxemia during exercise commonly occurs in patients with severe COPD as a result of the effects of a fall in mixed venous oxygen tension (PvO2) on low ventilation– perfusion lung units and shunting (1). In severe COPD, both the ability to increase lung perfusion and to distribute inS650 Official Journal of the American College of Sports Medicine FIGURE 4 —(A) Tidal flow–volume loops at rest (solid lines) and at isotime during a given load of exercise (dotted lines) are shown while breathing room air and oxygen. The maximal flow–volume envelope measured on room air is also shown (solid line on left, dashed line on right). In response to a drop in ventilation (VE) of approximately 3 L·minⴚ1, inspiratory capacity (IC) is improved and dynamic hyperinflation (DH) is reduced. (B) Exertional dyspnea fell significantly (*P < 0.05) in response to oxygen therapy. spired ventilation during exercise is compromised (1,8). Resting physiological dead space is often increased, reflecting ventilation–perfusion abnormalities, and may fail to decline further during exercise, as is the case in health (1,8). To maintain appropriate alveolar ventilation and blood gas homeostasis in the face of an increased physiological dead space, minute ventilation must increase. High physiological dead space in the setting of a blunted VT response to exercise in hyperinflated COPD patients will compromise CO2 elimination. Thus, exercise-induced hypercapnia, as a result of alveolar hypoventilation, can occur in severely mechanically compromised patients with COPD. Derangements of blood gases beyond a critical level will excessively stimulate ventilation, aggravate dynamic hyperinflation, and cause early ventilatory limitation to exercise (Fig. 4). It must be emphasized that the effects of hypoxemia are multifactorial and involve many integrated mechanisms that culminate in reduced exercise performance in COPD. In addition to the stress on the ventilatory system caused by hypoxia, reduced oxygen delivery to the active peripheral muscles may increase reliance on anaerobic glycolysis and also contribute to muscle fatigue. Other deleterious effects of acute exercise hypoxemia include 1) impaired cardiovascular function, 2) impaired central nervous system function, http://www.acsm-msse.org 3) alteration of afferent inputs from peripheral chemoreceptors, and 4) altered perception of dyspnea and leg discomfort. The relative importance of these factors likely varies between individuals. Although gas exchange abnormalities, such as severe hypoxemia, are inextricably linked to ventilatory limitation in COPD, the effects of correction of arterial hypoxemia on exercise performance are quite variable and unpredictable in a given subject (6,24,60). However, in general, patients with the most severe mechanical and gas exchange abnormalities benefit most in terms of improved dyspnea and exercise endurance (36,45). INCREASED VENTILATORY DEMAND The effects of the above-outlined mechanical derangements in COPD are often compounded by concomitantly increased ventilatory demand. Many studies have shown that VE at a given submaximal work rate is significantly increased compared with normal (10,16,41). Factors contributing to increased ventilation include high physiological dead space, earlier lactate acidosis, hypoxemia, high metabolic demands, low arterial CO2 set point, and other nonmetabolic sources of ventilatory stimulation (e.g., anxiety, hyperventilation). For a given level of expiratory flow limitation, the extent of dynamic hyperinflation and its consequent negative sensory consequences will vary with ventilatory demand. Those with the highest ventilation will develop limiting ventilatory constraints on flow and volume generation, and greater dyspnea early in exercise (41). There is abundant evidence that increased ventilatory demand contributes to dyspnea causation in COPD, and dyspnea intensity during exercise has been shown in several studies to correlate strongly with the change in VE or with VE expressed as a fraction of maximal breathing capacity (26,41,42). For a given FEV1.0, patients who have greater ventilatory demands will have more severe chronic activityrelated dyspnea (41). Moreover, exertional dyspnea relief after interventions such as exercise training (42), oxygen therapy (45), and opiates (28) has been shown to result, in part, from the reduced submaximal ventilation (see below). DELAYING VENTILATORY LIMITATION Quantitative flow–volume loop analysis during constantload exercise testing (at approximately 75% of the achievable peak work rate or V̇O2), allows a noninvasive assessment of ventilatory mechanics in COPD: changes in dynamic IC correlate strongly with the elastic load (2,38). Furthermore, comparison of exercise flow–volume loops before and after therapeutic interventions at a standardized time using this protocol provide valuable insights into the mechanisms of improved exercise performance and symptoms, vis-à-vis their effects on ventilatory limitation (39). To improve exercise capacity in symptomatic COPD patients, therapeutic interventions must either increase ventilatory capacity (i.e., the maximal flow–volume envelope), delay the rate of DH (i.e., the shift of exercise tidal flow– VENTILATORY LIMITATIONS volume loops toward TLC during exercise), or a combination of both. Bronchodilator therapy. Combination bronchodilator therapy with inhaled anticholinergic and 2 sympathomimetic agents represents the first step in the management of symptomatic COPD. These agents have each been shown to successfully alleviate dyspnea and improve exercise performance, even in advanced COPD (2,39). Bronchodilator therapy has been shown to increase maximal (and tidal) expiratory flow rates over the operating volume range, consequently providing more effective lung emptying with a reduction in dynamic lung volumes throughout exercise (2,39) (Fig. 5). Bronchodilators, therefore, delay the attainment of critical ventilatory limitation and significantly improve exercise endurance and reduce dyspnea (43). For example, after high-dose anticholinergic therapy in advanced COPD, we have shown that the inspiratory reserve volume was significantly increased at any given work rate or ventilation compared with placebo, in conjunction with an increase in exercise endurance time by 32% of the control value (43) (Fig. 5). Because of this delay in ventilatory limitation, dyspnea was displaced by leg discomfort in many patients as the primary exercise-limiting symptom (43). It is noteworthy that important improvements in exercise operational lung volumes and endurance times often occur after bronchodilators in the presence of minimal or no change in the resting postbronchodilator FEV1.0 (2,7,39). This likely reflects the fact that the FEV1.0 provides only a crude estimation of dynamic small airway dysfunction and the extent of prevailing expiratory flow limitation. The change in resting IC, which indicates greater capacity for VT expansion during exercise, correlates better with improved exercise endurance than the FEV1.0 (43). Lung volume reduction surgery. Surgical reduction of lung volume by resection of targeted areas of emphysematous lung destruction has also been shown to delay ventilatory limitation. This is achieved by increasing the maximal and tidal flow–volume loops chiefly by increasing static lung recoil and airway tethering effects (12,32). Improved airway conductance in turn promotes more effective lung emptying and reduces resting and exercise operational lung volumes (12,32). Reduced operational lung volumes after lung volume reduction surgery (LVRS) correlated closely with the extent of symptom relief (32). Additional improvements in dynamic ventilatory mechanics occur after LVRS as a result of reduced ventilatory demand. Reduced submaximal VE after surgery may reflect improved oxygenation in some cases, but more importantly, often reflects the response to ancillary perioperative exercise training (43). Oxygen therapy. Since the extent of DH during exercise in flow-limited COPD patients depends on the ventilation and the breathing pattern for a given ventilation, it follows that therapeutic interventions that reduce submaximal ventilation during exercise, such as supplemental oxygen therapy, exercise training, and opiates, should delay the rate of DH and the onset of critical ventilatory constraints that limit exercise (45) (Fig. 4). These interventions do not typically affect the maximal flow–volume loop envelope (as Medicine & Science in Sports & Exercise姞 S651 FIGURE 5—Responses to bronchodilator therapy (nebulized ipratropium bromide, 500 g) are shown. As maximal expiratory flow– volume relationships improved after dose, tidal flow–volume curves at rest can shift to the right, i.e., lung hyperinflation is reduced as reflected by an increased IC (top panel). Exertional dyspnea decreases significantly (*P < 0.05) in response to bronchodilator therapy (middle panel). Operational lung volumes improve in response to bronchodilator therapy, i.e., mechanical constraints on VT expansion are reduced as IC and IRV are increased significantly (*P < 0.05) (lower panel). Adapted from O’Donnell et al. (38) with permission. in the case of bronchodilators), but merely alter the time course for the development of restrictive ventilatory mechanics (45) (Fig. 4). In a placebo-controlled, crossover study, where patients with advanced COPD received either 60% oxygen or room air, we have recently shown that hyperoxia more than doubled the time to reach ventilatory S652 Official Journal of the American College of Sports Medicine limitation (45) (Fig. 4). In this study, the improvements in dyspnea and exercise endurance during hyperoxia were explained, in large measure, by the effects of reduced ventilatory demand (i.e., by reducing hypoxic drive and the metabolic load) on operational lung volumes (45). At a standardized submaximal work rate, VE was decreased by approximately 3 L·min⫺1 and the inspiratory reserve volume increased by 0.3 L during 60% oxygen compared with room air (45) (Fig. 5). The effects of oxygen therapy on exercise performance are complex: in addition to delaying ventilatory limitation, oxygen also improves the metabolic load, peripheral muscle function, and cardiac function. The relative importance of these various factors in contributing to improved exercise endurance in a given individual is difficult to evaluate, but in patients with unequivocal ventilatory limitation on room air, O2-induced changes in operational lung volumes and dyspnea appear to be most important (30,45). Exercise training. Exercise training, which has been shown repeatedly to reduce submaximal ventilation in advanced COPD (by improving efficiency and/or reducing the metabolic acidemia) should also, theoretically, alter ventilatory limitation in a manner similar to hyperoxia (5,44). Clearly, improved exercise endurance after exercise training is multifactorial, but improved dyspnea and/or leg discomfort are important contributory factors. Improved dyspnea is likely related to improved ventilatory muscle strength and endurance and reduced ventilatory demand. Reduced submaximal ventilation after training mainly reflects reduced breathing frequency responses to exercise. In some patients, this is accompanied by increased VT expansion. This more efficient breathing pattern is associated with more effective CO2 elimination, and both factors may combine to ameliorate respiratory discomfort. Dyspnea relief after exercise training is also undoubtedly linked to “nonphysiological” factors such as reduced fear and anxiety, increased tolerance, or systemic desensitization to respiratory discomfort as a result of participation in a comprehensive pulmonary rehabilitation program. These subjective changes alone may improve exercise endurance in some patients in the absence of measurable physiological training effects. Evidence is accumulating that small reductions in ventilation and operational lung volumes have clinically important effects in people with hyperinflated COPD who are ventilatory limited during exercise (31,45). Moreover, a comprehensive multimodality approach to management with combined bronchodilator therapy, oxygen, and exercise training generally results in additive or synergistic effects on exercise performance (Fig. 6). VENTILATORY MUSCLE DYSFUNCTION IN COPD Inspiratory muscle function. The degree to which ventilatory pump failure contributes to ventilatory limitation in COPD is uncertain and has been the subject of intense study (4,13,22,23,52). Theoretically, reduced ventilatory http://www.acsm-msse.org FIGURE 6 —(A) Exercise endurance increases significantly (*P < 0.05, **P < 0.01) in response to various interventions in COPD: nebulized ipratropium bromide (IB) 500 g, 60% O2 (shown for both hypoxic (open bar) and nonhypoxic (solid bar) patients), exercise training (EXT), inhaled morphine (opiates), optimized low-level continuous positive airway pressure (CPAP), and volume reduction surgery (VRS). From references 39, 36, 45, 44, 40, and 49, respectively. (B) Exertional dyspnea improves cumulatively with a stepwise approach to therapy. Adapted from O’Donnell (48) with permission. capacity caused by reduced ventilatory muscle strength or fatigue in the setting of increased ventilatory muscle loading should contribute to ventilatory limitation in many patients with advanced COPD (4,13,22,52). However, the evidence that a weakened ventilatory pump contributes to exercise intolerance is not conclusive (22,23,35,38). The prevalence of inspiratory muscle weakness in the COPD population has not been established and may not be as pervasive as previously thought. In fact, there is evidence that functional muscle strength is remarkably preserved in some patients with advanced chronic ventilatory insufficiency (57). Patients with acute-on-chronic hypercapnia during exercise have been shown to have no acute deterioration in maximal force-generating capacity, and do not exhibit alteration in the pattern of ventilatory muscle recruitment compared with nonhypercapnic individuals matched for FEV1.0 (35). The results of studies on the effects of specific inspiratory muscle training on exercise performance in COPD have been inconsistent (58). Similarly, the effects of long-term, noninvasive ventilatory assistance (designed to reduce chronic fatigue) on dyspnea and exercise performance in a large COPD population have been negative. Role of assisted ventilation. Indirect evidence that acute inspiratory muscle weakness contributes to ventilatory VENTILATORY LIMITATIONS limitation in some individuals with COPD comes from studies of acute ventilatory assistance during exercise in COPD using CPAP or pressure support, alone or in combination (50 –52). Such studies have shown an improvement in exercise endurance by 30 – 40%, on average, with impressive relief of dyspnea in individual COPD patients (40,51). Optimized CPAP counterbalances the negative effects of the inspiratory threshold load on the inspiratory muscles, and pressure support provides variable resistive and elastic unloading of these muscles. In general, the effects of ventilatory assistance on exercise capacity have been quite variable and the magnitude of the response is either comparable to, or less than, the effects of ambulatory oxygen (36,45). Ventilatory assistance often does not affect ventilatory limitation per se but, by assisting the weakened, overburdened muscles, may delay the point of intolerable dyspnea and the breakpoint of exercise. Expiratory muscle recruitment. In the presence of expiratory flow limitation, tidal expiratory flow rates are independent of expiratory transpulmonary pressures beyond a critical level (15). In fact, increasing expiratory effort beyond this level not only fails to increase expiratory flow, but results in dynamic airway compression of the airways downstream from the flow-limiting segment (15). Expiratory muscle recruitment appears to be highly variable in COPD during exercise (11,34,53). During constant-load exercise, some patients allow expiratory transpulmonary pressures to reach, but not exceed, the critical flow-limiting pressure, thus attenuating dynamic airway compression (25). Expiratory muscle recruitment may assist the inspiratory muscles by favorably altering diaphragmatic configuration or by the release of stored elastic energy at the onset of inspiration. Several studies have shown marked expiratory muscle activity at high work rates in COPD (11,34,53). This possibly maladaptive behavior will not improve alveolar ventilation and will aggravate dynamic airway compression, which in turn likely contributes to increased exertional dyspnea (46,47). Excessive expiratory intrathoracic and abdominal pressures, with reduced velocity of shortening of the expiratory muscles, may also significantly impair cardiac function in exercising COPD patients (53). The net effect of intense expiratory muscle recruitment on exercise performance will vary among COPD patients. In many patients, the deleterious effects of vigorous expiratory muscle contraction on symptoms and cardiac performance may outweigh potential beneficial effects on inspiratory muscle function. SUMMARY On the basis of extensive studies in COPD patients, we can conclude that ventilatory limitation contributes importantly, and often predominantly, to exercise limitation. Expiratory flow limitation is the hallmark of this heterogeneous condition, and its most important consequence during exercise is dynamic lung hyperinflation, which accelerates ventilatory limitation and exercise termination. The recognition that dynamic hyperinflation is one factor contributing Medicine & Science in Sports & Exercise姞 S653 to reduced ventilatory capacity is potentially clinically important, since lung hyperinflation is at least partially reversible and can, therefore, be manipulated for the patient’s benefit. Interventions that improve airway function and lung emptying will reduce operational lung volumes during exercise, and delay the occurrence of critical ventilatory constraints, thus improving exercise endurance and symptoms. An integrative approach that maximizes lung emptying (combined bronchodilators) and further reduces the rate of gas accumulation by reducing ventilatory demand during exercise (i.e., oxygen therapy and exercise training) can result in clinically meaningful benefits for the patient with advanced symptomatic COPD. Although much of the scientific evidence currently available refers to COPD patients, certain of the principles of exercise limitation described above also apply to patients with other types of chronic pulmonary disease. The reduced ventilatory capacity in chronic restrictive pulmonary disease would imply that measures to reduce exercise ventilation, such as supplemental oxygen and exercise training, would have similar applicability as in COPD. Furthermore, patients with neuromuscular diseases have important mechanical abnormalities, including respiratory muscle dysfunction and altered respiratory system compliance, that likely impact exercise ability. Investigation of the ventilatory limitation needs to be extended to these other forms of chronic pulmonary disease. In the future, better understanding of the pathophysiology of all types of chronic pulmonary disease will, perhaps, lead to more specific treatment strategies depending on the type of patient. Address for correspondence: Dr. Denis E. O’Donnell, 102 Stuart Street, Kingston, Ontario K7L 2V6, Canada; E-mail: odonnell@post. queensu.ca. REFERENCES 1. BARBARA, J. A., J. ROCA, J. RAMIREZ, et al. Gas exchange during exercise in mild chronic obstructive pulmonary disease. Am. Rev. Respir. Dis. 144:520 –525, 1991. 2. BELMAN, M. J., W. C. BOTNICK, and J. W. SHIN. Inhaled bronchodilators reduce dynamic hyperinflation during exercise in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 153:967–975, 1996. 3. BROWN, S. E., R. R. KING, S. M. TEMERLIN, et al. Exercise performance with added deadspace in chronic airway obstruction. J. Appl. Physiol. 56:1020 –1026, 1984. 4. BYE, P. T., S. A. ESAU, R. D. LEVY, et al. Ventilatory muscle function during exercise in air and oxygen in patients with chronic airflow limitation. Am. Rev. Respir. Dis. 132:236 –240, 1985. 5. CASABURI, R., A. PATESSIO, F. IOLI, S. ZANABONI, C. F. DONNER, and K. WASSERMAN. Reductions in exercise lactic acidosis and ventilation as a result of exercise training in patients with obstructive lung disease. Am. Rev. Respir. Dis. 143:9 –18, 1991. 6. CHRONOS, N., L. ADAMS, and A. GUZ. Effect of hyperoxia and hypoxia on exercise-induced breathlessness in normal subjects. Clin. Sci. 74:531–537, 1988. 7. CHRYSTYN, H., B. A. MULLEY, and M. D. PEAKE. Dose response relation to oral theophylline in severe chronic obstructive airways disease. BMJ. 297:1506 –1510, 1988. 8. DANTZKER, D. R., and G. E. D’ALONZO. The effect of exercise on pulmonary gas exchange in patients with severe chronic obstructive pulmonary disease. Am. Rev. Respir. Dis. 134:1135–1139, 1986. 9. DIAZ, O., C. VILLAFRANCO, H. GHEZZO, et al. Exercise tolerance in COPD patients with and without tidal expiratory flow limitation at rest. Eur. Respir. J. 16:269 –275, 2000. 10. DILLARD, T. A., S. PIANTADOSI, and K. R. RAJAGOPAL. Prediction of ventilation at maximal exercise in chronic airflow obstruction. Am. Rev. Respir. Dis. 132:230 –235, 1985. 11. DODD, D. S., T. BRANCATISANO, and L. A. ENGEL. Chest wall mechanics during exercise in patients with severe chronic airflow obstruction. Am. Rev. Respir. Dis. 129:33–38, 1984. 12. GELB, A., N. ZAMEL, R. MCKENNA, and M. BRENNER. Mechanism of short-term improvement in lung function after emphysema resection. Am. J. Respir. Crit. Care Med. 154:945–951, 1996. 13. GRASSINO, A., D. GROSS, P. T. MACKLEM, C. ROUSSOS, and G. ZAGELBAUM. Inspiratory muscle fatigue as a factor limiting exercise. Bull. Eur. Pathophysiol. Respir. 15:105–111, 1979. 14. HENKE, K. G., M. SHARRATT, D. F. PEGELOW, J. A. DEMPSEY. Regulation of end-expiratory lung volume during exercise. J. Appl. Physiol. 64:135–146, 1988. 15. HYATT, R. E. Expiratory flow limitation. J. Appl. Physiol. 55:1– 8, 1983. S654 Official Journal of the American College of Sports Medicine 16. JOHNSON, B. D., I. M. WERSMAN, R. J. ZEFALLOS, and K. C. BECK. Emerging concepts in the evolution of ventilatory limitation during exercise. Chest 116:488 –503, 1999. 17. JOHNSON, B. D., K. W. SAUPE, and J. A. DEMPSEY. Mechanical constraints on exercise hypercapnia in endurance athletes. J. Appl. Physiol. 73:874 – 886, 1992. 18. JOHNSON, D. B., W. G. REDDAN, K. C. SEOW, and J. DEMPSEY. Mechanical constraints on exercise hypercapnea in an aging population. Am. Rev. Respir. Dis. 143:968 –977, 1991. 19. JONES, N. L., G. JONES, and R. H. T. EDWARDS. Exercise tolerance in chronic airway obstruction. Am. Rev. Respir. Dis. 103:477– 491, 1971. 20. KILLIAN, K. J., and N. J. JONES. Respiratory muscles and dyspnea. Clin. Chest Med. 9:237–248, 1988. 21. KLAS, J. V., and J. A. DEMPSEY. Voluntary versus reflex regulation of maximal exercise flow-volume loops. Am. Rev. Respir. Dis. 139:150 –156, 1989. 22. KYROUSSIS, D., M. I. POLKEY, S. E. J. KEILTY, et al. Exhaustive exercise shows inspiratory muscle relaxation rate in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 153: 787–793, 1996. 23. KRYOUSSIS, D., M. I. POLEY, G.-H. HAMMEGARD, G. H. MILLS, M. GREEN, and J. MOXHAM. Respiratory muscle activity in patients with COPD walking to exhaustion with and without pressure support. Eur. Respir. J. 15:649 – 655, 2000. 24. LANE, R., A. A. COCKROFT, L. ADAMS, and A. GUZ. Arterial oxygen saturation and breathlessness in patients with chronic obstructive airways disease. Clin. Sci. 72:693– 698, 1987. 25. LEAVER, D. G., and N. B. PRIDE. Flow volume curves and expiratory pressures during exercise in patients with chronic airflow obstruction. Scand. J. Respir. Dis. 42(Suppl.):23–27, 1971. 26. LEBLANC, P., D. M. BOWIE, E. SUMMERS, N. L. JONES, and K. J. KILLIAN. Breathlessness and exercise in patients with cardio-respiratory disease. Am. Rev. Respir. Dis. 133:21–25, 1986. 27. LEVISON, H., and R. M. CHERNIACK. Ventilatory cost of exercise in chronic obstructive pulmonary disease. J. Appl. Physiol. 25:21– 27, 1968. 28. LIGHT, R. W., J. R. MURO, R. I. SATO, D. W. STANSBURY, C. E. FISCHER, and S. E. BROWN. Effects of oral morphine on breathlessness and exercise tolerance in patients with chronic obstructive pulmonary disease. Am. Rev. Respir. Dis. 139:126 –133, 1989. 29. LIND, F., and C. M. HESSER. Breathing pattern and lung volumes during exercise. Acta Physiol. Scand. 120:123–129, 1984. 30. LOUGHEED, M. D., K. A. WEBB, and D. E. O’DONNELL. Breathlessness during induced lung hyperinflation in asthma: the role of the inspiratory threshold load. Am. J. Respir. Crit. Care Med. 152: 911–920, 1995. http://www.acsm-msse.org 31. MALTAIS, F., P. LEBLANC, C. SIMARD, et al. Skeletal muscle adaptation to endurance training in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 154:442– 447, 1996. 32. MARTINEZ, F. J., M. MONTES DE OCA, R. I. WHYTE, J. STETZ, S. E. GAY, and B. R. CELLI. Lung-volume reduction improves dyspnea, dynamic hyperinflation and respiratory muscle function. Am. J. Respir. Crit. Care Med. 155:1984 –1990, 1997. 33. MILIC-EMILI, J. Inspiratory capacity and exercise tolerance in chronic obstructive pulmonary disease. Can. Respir. J. 7:282–285, 2000. 34. MONTES DE OCA, M., J. RASSULO, and B. R. CELLI. Respiratory muscle and cardiopulmonary function during exercise in very severe COPD. Am. Rev. Respir. Crit. Care Med. 154:1284 –1289, 1996. 35. MONTES DE OCA, M., and B. R. CELLI. Respiratory muscle recruitment and exercise performance in eucapnic and hypercapnic severe chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 161:880 – 885, 2000. 36. O’DONNELL, D. E., D. J. BAIN, and K. A. WEBB. Factors contributing to relief of exertional breathlessness during hyperoxia in chronic airflow limitation. Am. J. Respir. Crit. Care Med. 155: 530 –535, 1997. 37. O’DONNELL, D. E., and K. A. WEBB. Exertional breathlessness in patients with chronic airflow limitation: the role of hyperinflation. Am. Rev. Respir. Dis. 148:1351–1357, 1993. 38. O’DONNELL, D. E., J. C. BERTLEY, L. K. CHAU, and K. A. WEBB. Qualitative aspects of exertional breathlessness in chronic airflow limitation: pathophysiologic mechanisms. Am. J. Respir. Crit. Care Med. 155:109 –115, 1997. 39. O’DONNELL, D. E., M. LAM, and K. A. WEBB. Measurement of symptoms, lung hyperinflation and endurance during exercise in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 158:1557–1565, 1998. 40. O’DONNELL, D. E., R. SANII, G. GIESBRECHT, and M. YOUNES. Effect of continuous positive airway pressure on respiratory sensation in patients with chronic obstructive pulmonary disease during submaximal exercise. Am. Rev. Respir. Dis. 138:1185–1191, 1988. 41. O’DONNELL, D. E., and K. A. WEBB. Breathlessness in patients with severe chronic airflow limitation: physiologic correlates. Chest 102:824 – 831, 1992. 42. O’DONNELL, D. E., M. MCGUIRE, L. SAMIS, and K. A. WEBB. The impact of exercise reconditioning on breathlessness in severe chronic airflow limitation. Am. J. Respir. Crit. Care Med. 152: 2005–2013, 1995. 43. O’DONNELL, D. E., M. LAM, and K. A. WEBB. Spirometric correlates of improvement in exercise performance after anticholinergic therapy in COPD. Am. J. Respir. Crit. Care Med. 160:524 –549, 1999. 44. O’DONNELL, D. E., M. MCGUIRE, L. SAMIS, and K. A. WEBB. Effects of general exercise training on ventilatory and peripheral muscle strength and endurance in chronic airflow limitation. Am. J. Respir. Crit. Care Med. 157:1489 –1497, 1998. 45. O’DONNELL, D. E., C. D’ARSIGNY, E. N. HOLLINGWORTH, and K. A. WEBB. Oxygen reduces dynamic hyperinflation and improves ex- VENTILATORY LIMITATIONS 46. 47. 48. 49. 50. 51. 52. 53. 54. 55. 56. 57. 58. 59. 60. 61. ercise performance in hypoxic patients with COPD. Am. J. Respir. Crit. Care Med. 161:A753, 2000. O’DONNELL, D. E., R. SANII, N. R. ANTONISEN, and M. YOUNES. Effect of dynamic airway compression on breathing pattern and respiratory sensation in severe chronic obstructive pulmonary disease. Am. Rev. Respir. Dis. 135:912–918, 1987. O’DONNELL, D. E., R. SANII, N. R. ANTONISEN, and M. YOUNES. Expiratory resistive loading in patients with severe chronic airflow limitation: an evaluation of ventilatory mechanics and compensatory responses. Am. Rev. Respir. Dis. 136:102–107, 1987. O’DONNELL, D. E. Dyspnea in advanced COPD. J. Heart Lung Transplant. 17:544 –559, 1998. O’DONNELL, D. E., J. BERTLEY, K. A. WEBB, and A. A. CONLAN. Mechanisms of relief of exertional breathlessness following unilateral bullectomy and lung volume reduction surgery in advanced chronic airflow limitation. Chest 110:18 –27, 1996. O’DONNELL, D. E., R. SANII, and M. YOUNES. Improvement in exercise endurance in patients with chronic airflow limitation using CPAP. Am. Rev. Respir. Dis. 138:1510 –1514, 1988. PETROF, B. J., E. CALDERINI, and S. B. GOTTFRIED. Effect of CPAP on respiratory effort and dyspnea during exercise in severe COPD. J. Appl. Physiol. 69:178 –188, 1990. POLKEY, M. I., D. KYROUSSIS, G. H. MILLS, et al. Inspiratory pressure support reduces slowing of inspiratory muscle relaxation rate during exhaustive treadmill walking in severe COPD. Am. J. Respir. Crit. Care Med. 154:1146 –1150, 1996. POTTER, W. A., S. OLAFSSON, R. E. HYATT. Ventilatory mechanics and expiratory flow limitation during exercise in patients with obstructive lung disease. J. Clin. Invest. 50:910 –919, 1971. PRIDE, N. B., and P. T. MACKLEM. Lung mechanics in disease. In: Handbook of Physiology, Section 3, Vol. III, Part 2. The Respiratory System. A. P. Fishman (Ed.). Bethesda, MD: American Physiological Society, 1986, pp. 659, 692. ROCHESTER, D. F. The diaphragm in COPD: better than expected, but not good enough. N. Engl. J. Med. 325:961–962, 1991. ROCHESTER, D. F., and N. M. T. BRAUN. Determinants of maximal inspiratory pressure in chronic obstructive pulmonary disease. Am. Rev. Respir. Dis. 132:42– 47, 1970. SIMILOWSKI, T., S. YAN, A. P. GAUTHIER, P. T. MACKLEM, and F. BELLEMERE. Contractile properties of the human diaphragm during chronic hyperinflation. N. Engl. J. Med. 325:917–923, 1991. SMITH, K., D. COOK, G. H. GUYATT, J. MADHOVEN, and A. D. OXMAN. Respiratory muscle training in chronic airflow obstruction. Am. Rev. Respir. Dis. 145:533–539, 1992. STUBBING, D. G., L. D. PENGELLY, J. L. C. MORSE, and N. L. JONES. Pulmonary mechanics during exercise in subjects with chronic airflow limitation. J. Appl. Physiol. 49:511–515, 1980. SWINBURN, C. R., J. M. WAKEFIELD, P. W. JONES. Relationship between ventilation and breathlessness during exercise in chronic obstructive airways disease is not altered by prevention of hypoxemia. Clin. Sci. 67:515–519, 1984. YOUNES, M. Determinants of thoracic excursions during exercise. In: Lung Biology in Health and Disease, Vol. 42: Exercise, Pulmonary Physiology and Pathophysiology. B. J. Whipp and K. Wasserman (Eds.). New York: Marcel Dekker, 1991, pp. 1– 65. Medicine & Science in Sports & Exercise姞 S655