Scapular Taping in the Treatment of Anterior Shoulder
advertisement

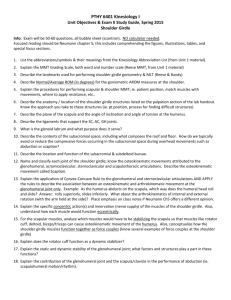
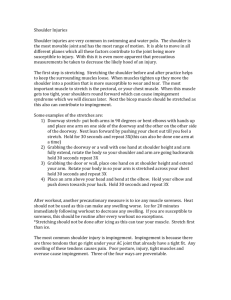
Case Report Scapular Taping in the Treatment of Anterior Shoulder Impingement The puqose of this case report is to describe how taping designed to promote proximal scapular stability was used in conjunction with other physical therapy interventions to manage a patient with anterior shoulder impingement. The taping technique is described in detail. The eualuation and treatment of a patient with an 8-month histo7y of shoulder pain are described as an example of when this type of taping procedure may be indicated. nis case report demonstrates that a patient was able to return to all of his regular overhead sports activities without pain following scapular taping used in combination with a home exercise program. Presumably, the improved resting position of the scapula corrected faulty scapulothoracic joint movements. [Host HH. Scapular taping in the treatment of anterior shoulder impingement. Phys Ther. 1995; 75:80+ 812.1 Key Wonls: Comernative treatment, Scapula, Shoulder impingement. Athletes who participate in sports that require repeated overhead motions, such as those involved in swimming, tennis, or throwing sports (eg, baseball), and who have faulty shoulder or scapular movement patterns appear to be most at risk for developing shoulder pain.lx2 "Overhead or "overhand movements can be defined as glenohumeral movements in the range of 90 degrees, or greater, of flexion, abduction, or a combination of the two motions. Sports that require these motions subject the shoulder to a large range of motion, repetitively, which can result in anterior shoulder instability and eventually microtrauma of the soft tissue surrounding the glenohumeral joint.l.3 This injury can lead to impingement of the rotator cuff tendons, which, over time, can cause a rotator cuff tear.3 This problem is most often treated with physical therapy and physician-prescribed nonsteroidal anti-inflammatory medications.l.+5 If no improvement is seen in the patient's condition within 3 months, surgery is often performed.3~4 The purpose of this case report is to illustrate the use of scapular taping in a patient with impingement of his right rotator cuff tendons. Taping was used only after the patient's symptoms were not relieved by attempting to correct his faulty overhead movements through exercise and education in the use of proper scapular positioning. Scapular taping and exercises appeared to be effective in relieving symptoms, and the patient was able to return to all of his overhead recre- ational and sports activities without pain. The taping, I believe, promotes proximal stability of the scapula, allowing humeral motion without the subsequent pain that can result from impingement of the rotator cuff tendons. The taping technique is thought to affect the resting position of the scapula and assist in maintaining the proximal shoulder-girdle stability necessary to perform elevating motions of the arm. With the tape holding the scapula in a more proper alignment, the patient can then use the shoulder without further stressing the impinged tendons. Additionally, the tape provides a feedback mechanism allowing the patient to feel "normal" alignment and positioning of the shoulder complex. l n t d e w Data HH Host, PT, is a doctoral student in the Program in Movement Science, Washington University School of Medicine, Box 8502, 660 S Euclid Ave, St Louis, MO 63110 (USA) (hhhost@ansci.wustl.edu). A right-handed, 40-year-old, Caucasian man with a diagnosis of right shoulder pain was referred to physical therapy by his orthopedic surgeon. At the time 7his article was submitted July ZG,1994, and was accepted May 8, 1995. Physical Therapy / Volume 75, Number 9 / September 1995 803/ 27 (NaprosynBt), without noticeable benefit. Physical Examination Dafa During the patient's initial physical therapy visit, an ordinal self-report rating scale was used to assess the intensity of his pain at rest and during shoulder movements. He rated his pain intensity by assigning a number from a 0 to 10, where 0 represented no pain and 10 represented the worst imaginable pain.6 The patient reported a 0 pain rating for both (right and left) shoulders while at rest. . Figure 1 Dotted outline illustrates the position of the patient's scapula, and the solid outline shows where the scapula should "normally"be positioned. His right scapula is in aposition of downward rotation (inferior-medial border of the scapula closer to spinous processes than superior-medial border). Taping technique can help improue the resting position of the scapula and make it more like the "nom1"position. of the initial visit, he reported an %month history of progressively worsening symptoms. His primary complaint was of intermittent pain in the anterior-superior glenohumerdl joint with activities requiring the use of his right arm for overhead motions. He was employed as a laboratory research technician and was recreationally very active, participating in some type of sports activity daily. He stated he had been regularly weight training (on Nautilus equipment,' performing the entire circuit of upper- and lowerextremity exercises) three times per week and played racquetball and tennis 1 to 2 days per week, on a year-round basis and had been doing so for at least 10 yean. The only modification made by the patient, secondary to onset of his right shoulder pain, was that 2 months after the symptoms first developed, he stopped playing tennis because he could not serve without severe pain. When the patient first came to physical therapy, he reported slight pain in his right shoulder during each weight-training session, but a great increase in pain the morning following each session. He also reported having pain when trying to throw a baseball. He described the pain as being in his anterior-superior right glenohumeral joint and reported a "popping" sensation when he lifted hls right arm overhead. The patient had been seen by two different physicians, and he said they told him that radiographs were negative for evidence of fracture or moderate to severe ligamentous disruption. He repolted taking prescribed nonsteroidal anti-inflammatory medication *Sports/Medical Industries, PO Box 1783, Depart PT, DeLand, FL 32721. ??yntex Laboratories Inc, 3401 Hillview Ave, P O Box 10850, Palo Alto, CA 94303. The patient reported pain (pain rating=5) during right shoulder flexion (in the 150°-180° range) and abduction (in the 140°-170' range) while standing. He had full, pain-free motion of the left shoulder. Additionally, when the patient was positioned supine with his shoulder abducted approximately 30 degrees, it was noted he had medial (internal) (0'-BO) and lateral (external) (00-1000) rotation of his right shoulder that exceeded normal values.' His left shoulder medial rotation was 0 to 80 degrees, which is also greater than the normal range, but he had normal lateral rotation on that side. Although intratester rehbility of these measures was not assessed, measurements of shoulder range of motion have been shown to be reliable when repeated by the same physical therapist.*,9The intrarater intraclass correlation coefficients for shoulder rotation ranged from .93 to Additionally, high intratester reliability of goniometric measurement of both upper- and lowerextremity joints has been established by several researchers.8-11 While the patient was standing, a visual inspection of his posture revealed he had bilateral forward shoulders, with the right shoulder more forward than the left shoulder ("forward was defined as the shoulder, from a lateral view, appearing anterior from the mid-coronal plane). From a posterior view, the right scapula appeared to be more abducted fmm the vertebral spinal processes than the left scapula. The right humeral head ap- Physical Therapy / Volume 75, Number 9 / September 1995 - Table 1. Manual Muscle Test Results for Initial and Final Visits Initial Visit Muscle Group Right Final Visit Left Right Left Shoulder flexors Shoulder abductors Shoulder medial (internal) rotations 4-/5 5/5 5/5 5/5 Shoulder lateral (external) rotations 4-/5 415 5/5 5/5 Biceps 5/5 5/5 5/5 5/5 Triceps 5/5 5/5 5/5 5/5 Supraspinatus opinion of several authors and is not based on data or research findings. Additionally, at rest, the left scapula's medial border remained parallel to the thoracic spinous processes along the entire extent, whereas the right scapula was in a position of downward rotation (ie, the inferior, medial border of the scapula was closer to the thoracic spinous processes than the superior, medial border of the same scap ula) (Fig. 1). Intratester reliability of measuring these scapular positions has not been assessed by this examiner or others. Lower trapezius Serratus anterior Middle trapezius Upper trapezius a Painful. peared, based on palpation, to be slightly anterior to the anterior border of the acromion, whereas on the left the humeral head was centered under the acrornion. Winging of both scapulae was evident along the entire length of the vertebral borders of the scapula; however, winging of the right scapula was greater than that observed of the left scapula. 'Winging" of the scapula occurs around the vertical axis and is almost universally used to describe a posterior displacement of the vertebral border of the scapula.12 Faulty scapulohumeral rhythm was thought to occur when the patient flexed and abducted his right humerus. The observed fault was an immediate and excessive scapular abduction and elevation during the initiation of either humeral motion and what appeared to be excessive (greater than 60") scapular abduction at the end range (180") of abduction and flexion. Scapular abduction was a p proximated based on visual estimates during the movements and measured once the patient achieved full flexion or abduction. The measurement was made with a goniometer with the stationary arm parallel to the thoracic spinous processes and the movable arm following the medial border of the scapula. Some authors '+I7 state that during complete (180" or full) humeral flexion or abduction, the range of scapular movement does not normally exceed 60 degrees, whereas the range of glenohumeral movement is approximately 120 degrees of motion. The excessive scapular abduction and elevation were not observed with flexion and abduction of the left shoulder. The patient was given verbal directions to keep his scapula "down" (depressed) and "back (adducted) while repeating right humeral flexion and abduction. At first, tactile cues were provided by the therapist, but after one to two attempts the patient was able to do this independently. While attempting to maintain his scap ula in a depressed and adducted position, he was able to perform right shoulder flexion and abduction without pain. The resting scapular positions were compared while the patient was standing. The medial border of the right scapula was abducted 9 cm away from the fourth thoracic spinous process, whereas the medial border of the left scapula was abducted 5 cm away from the same spinal landmark. The normal distance from the medial scapular border to the thoracic spinous processes is believed to be 5.08 cm (2 in).12J8J9This value, however, is the Physical Therapy /Volume 75, Number 9 / September 1995 There was notable tenderness to palpation over the right bicipital and rotator cuff tendons. There was no tenderness to palpation on the left side. Palpation of these tendons was performed in positions as described by several Differentiation of the rotator cuff tendons was not made, as it has been shown that the four rotator cuff tendons blend intimately together to form a continuous rotator ~uff.l7,~l Weakness (as determined with manual muscle testing) with pain was found when testing the right shoulder flexors and abductors and during testing of the supraspinatus muscle (Tab. All of the manual muscle tests were performed as previously described by Ker~dall,~ except for a test attempting to isolate the supraspinatus muscle, which was done as described by Jobe and Bradley 3 and Townsend et a1.Z Manual muscle testing grades can be reliable within examiners, under special conditions, according to several resear~hers.~3,~* Intertester reliability is not high.23.25 When performing tests that were used to assess muscle length, the patient exhibited shortness in the latissimus dorsi muscle (lacked 40" on the right and 30" on the left) and the pectoralis minor muscle (right posterior acromion approximately 5 cm [2 in] up from table and left posterior acromion approximately 2.5 crn [I in] up from the table), bilaterally. These tests were performed as described by Kendall? and neither test provoked pain in the 805 / 29 - ing other overhead activities with resistance (eg, lifting weights)' are both strong indicators of anterior shoulder impingement. Table 2. Stretching and Strengthening Exercises Exercise 1. Pectoralis minor muscle stretch-supine Description Patient positioned supine, hook-lying7with another person pressing, with the heel of hand over the patient's coracoid process, down and out at approximately a 45" angle away from the body. 2. Latissimus dorsi muscle stretch-supine Patient positioned supine, hook-lying in same position in which "tightness" is assessed7;care is taken to ensure that the patient does not arch the lower back. 3. Wall push-up with scapular adduction-standing Starting position-patient positioned standing, facing the wall with forearms resting on wall (thumbs facing away from wall) and shoulders flexed to approximately 90". Patient slides arms up wall making shape of letter "V" (similar position as strength test position of lower trapezius muscle7),until end range is reached or to just before pain starts. If able to go through full motion without pain, patient lifts arms away from the wall while retracting scapulae. Position is held 2-3 s; patient then returns arms to wall and slides them back to starting position. Maintenance of proper bacWtrunk posture is very important with this exercise. 4.Shoulder medial/lateral (intemal/external) rotation-prone ~ . ~towels used anterior to Patient positioned p r ~ n ewith humeral head to maintain proper glenohumeral alignment and shoulder abducted 90". Patient laterally rotates (0"-90") and medially rotates (0"-70"), concentrating on pure glenohumeral movement. This exercise was started with just the weight of the patient's arm and quickly progressed to using small dumbbells (1-5 lb). 5. Shoulder medial/lateral rotation with Thera-Band@,b-standing Patient positioned standing as illustrated in Kisner and Colby text" and using ~hera-Bandm to perform IateraVmedial rotation of the shoulder. Patient with shoulder in neutral, adducted starting position with the Thera-band" attached opposite from the direction in which he or she will pull. Patient started with yellow and moved up to blue Thera-bandmthroughout the treatment. 6. Lower trapezius muscle strengthening-prone This exercise is performed in same position in which the strength is assessed7,except secondary to this patient's weakness he started with just lifting his arm into the test position but with his elbow flexed and he eventually progressed to lifting a straightened arm with maintenance of proper scapular position (depression, lateral rotation of inferior angle, and adduction of the scapula). Last, he did the exercise with lightweight dumbbells. Assessment The patient's history and data from the physical examination support the diagnosis of anterior impingement of the right shoulder. The patient's history was the first indicator of an impingement syndrome. His inability to perform the maneuver that caused the impingement (his tennis serve)X4and his pain and discomfort after perform- The patient reported decreasing right shoulder pain until his fourth visit. During his fourth visit, he reported that after helping a friend move some heavy furniture he hurt h s right shoulder and had pain, even at rest, with an intensity rated at 4. He complained that he was again having pain during flexion and abduction and that he was Davis Co; 1985:258-259, 6 2 0 . bThe Hygenic Corp, 1245 Home Ave, Akron, OH 44310-2575. 30 / 806 Treatment Because the patient was able to resolve his pain with verbal and tactile cues on the first visit, I directed my initial treatment toward teaching him to flex and abduct his right humerus while attempting to maintain proper scapulohumeral position throughout the range of motion. He was also given exercises (Tab. 2) to stretch the short muscle groups and strengthen those muscle groups that were weak. He wanted to continue with his recreational activities, but it was emphasized to him that he should avoid any activities that caused his pain. He was able to continue llfting weights, but decreased the resistance during all of his arm exercises by 4.5 to 9.1 kg (10-20 lb). The patient was encouraged to correct his scapular position during performance of these exercises. If he experienced pain on any of the resistance exercises, he was instructed not to elevate his arms higher than the point of pain. " Kisner C, Colby LA. merapeutic Exercise: Foundations and Techniques. Philadelphia, Pa: FA right shoulder. It should be noted that although goniometric measures are reported to express an existence of a specdic muscle's shortness, this relationship has not been exanlined by research. As a rule, limitations in joint range of motion measurements may be due to a variety of causes and cannot be said to be only due to muscle tightness.26 Subjective measures such as the patient's postural faults, both in a standing, resting position and with elevation of his right humerus into flexion and abduction (faulty scapulohumeral positioning); his painful arcs of motion; his tenderness to palpation of the rotator cuff tendons and biceps tendon; his strength deficits; and his muscle shortness in specific muscle groups all suggested the patient had an anterior impingement of his right shoulder. This finding is based on several authors' classification of a stage I1 anterior shoulder impingement.+5.13.14 Physical Therapy / Volume 75, Number 9 / September 1995 Scapular Taping Technique Figure 2a. scapular taping technique: First strip of Cover-Rolf" in place. unable to reduce his pain with his own attempts at proper scapular positioning. I was able to decrease his pain by holding his right scapula in a more correct position during humeral flexion and abduction (this was accomplished by manually holding the scapula back into a more adducted position, assisting with upward rota- tion and preventing it from elevating excessively). This suggested that scapular taping might be helpful. The patient's scapula was taped to decrease the excessive abduction and winging and also to promote upward rotation, as opposed to the downwardly rotated position that was his resting position. *Distributed by Beiersdorf Inc, Norwalk, CT 06856-5529. Physical Therapy / Volume 75, Number 9 / September 1995 Cover-roll@stretch*was used to protect the patient's skin, and the taping was done using Leukosport@(Leukotape@P) tape.*The taping was initiated by first applying two 10.2cmwide (4-in-wide) Cover-Roll@strips to protect the skin. The first strip was applied pulling proximally from the right upper trapezius muscle belly region distally to approximately 5 to 7.6 cm (2-3 in) below the inferior angle of the right scapula (Fig. 2a). Another protective Cover-Roll@strip was then applied from the posteriorlateral right acrornion diagonally across the back and ended just lateral to the thoracic spinous processes (Fig. 2b). Several 3.8-cm-wide (1.5-in-wide) Leukosport@strips of tape were then applied, with the first two strips of tape starting at the mid-muscle belly region of the right upper trapezius muscle and pulling downward and in toward the spinous processes attaching the tape just medial and inferior to the inferior angle of the scapula (Fig. 2c). Additional strips of tape were then applied by starting with each piece from the mid-muscle belly region of the upper tmpezius muscle and continuing outward to the posterior-lateral acromial process. Each strip of tape was applied in order to pull the scapula back into adduction and slightly downward (from its starting, elevated position) (Fig. 2d). The strips of tape followed the line of pull of the lower and middle trapezius muscles. The tape was applied with the patient in a sitting position while an assistant or the therapist supported the patient's shoulder under the axillary region to relax the scapular muscles (especially the upper trapezius muscle). The tape was applied tightly, but loose enough to allow movement of the scapula with flexion or abduction of the humerus. A total of 8 to 10 strips of Leukospofl tape were used with this patient. After the tape was applied (Fig. 2e), the patient had pain-free full flexion and abduction of the right humerus. Assessment of the patient's motion with the tape in place allowed for immediate assessment of the tape's these four visits, the patient reported that his pain was progressively decreasing. On the patient's ninth visit, he was able to abduct and flex the right humerus through a complete 180-degree range of motion and perform his home exercise program without pain and without the tape, so the scapular taping was discontinued. The patient stated he continued to have occasional, brief periods of pain, but with consciously making an effort to hold his scapula "down and back," he could relieve the pain entirely. The patient was not seen for the following 3 weeks because he was out of town. His next visit was his 10th and final visit. He reported no pain with any of his work or recreational activities, although he would have an occasional "twinge" of pain (whlch he rated as 1-2) in the anterior right shoulder the day after a weight-lifting session, but he stated the pain was not as severe as before. The patient reported he had not yet resumed playing tennis. Figure 2b. Scapular taping technique: Second strip of Cover-Roll@in place. effectiveness, and it could be decided based on whether the patient had pain whether additional pieces of tape were required for further support. The patient's scapula was retaped on visits 5 through 8, with no more than 4 days between visits. The tape seemed to hold tightly for 2 to 3 days, at which time the patient reported he could feel it loosening and his painful symptoms would return. At that time, 32 / 808 the patient was instructed to remove the tape and return for another visit to have the scapula retaped. During each visit, immediately prior to taping, the patient would flex and abduct his right humerus to determine whether these motions were stdl causing pain. With each of these visits (visits 58), the patient continued to have complaints of pain (ratings equal to 3-5) without the tape during motions of right humeral flexion and abduction. Over Final impairment measurements were taken on this date to determine whether the patient had changed from the initial visit. In a standing, resting position, the right scapula's medial border was now 5 cm from the spinous process of T 4 . A slight winging was still evident in the right scapula, but the winging was not as great as during his initial visit. The muscle test attempting to isolate the right supraspinatus muscle was now 4+/5 (pain-free), and all other muscle tests revealed bilateral upper-extremity strengths of 5/5 with no pain Gab. 1). The diference between ratings of 4+ and 5 is that with a rating of 5 the patient can hold the test position against gravity and maximal pressure, whereas with a rating of 4+ the patient can hold against gravity and moderate pressure.' The patient's muscle shortness had improved in both his latissimus dorsi and pectoralis minor muscles, bilaterally, although he still did not have normal length. With assessment of his pectoralis minor muscle length, while positioned su- Physical Therapy /Volume 75, Number 9 / September 1995 the past 3 weeks. He stated he was playing racquetball without pain, along with practicing his tennis serve. It was recommended that he continue with his home exercise program. A second follow-up phone call was made, 3 months after his last visit and the patient reported that he was no longer having any pain and had resumed playing tennis a few times a week, along with his other recreational activities. Several factors will determine successful treatment of a patient with shoulder impingement syndrome. One of the most impomnt criteria must be reduction of the patient's complaints of pain. Second, the return of the patient to his or her prior activity level provides a measure of successful outcome. Impingement of the rotator cuff is presumably the result of poor shoulder-girdle mechanics and may be due to hypomobility (shortening of soft tissue), hypermobility (lengthening of soft tissue that can eventually lead to damage to the labrum), or strength imbalances of one or more muscles about the shoulder girdle.*' AU of these factors may have contributed to the anterior shoulder impingement of the patient described in thii case report. Figure 2 ~ .Scapular taping technique: Application of Leukosport@tape, with support given under patient's axilla. pine, the patient's posterior acromion was about 2.5 cm (1 in) above the table surface on the right and about 1.3 cm (0.5 in) above the table surface on the left. With measurement of the latissimus dorsi muscle length, the patient was now lacking 15 degrees (from 180') on the right and 10 degrees on the left. The patient was encouraged to start practicing his tennis serve, and to progress with this activity over the next 4 to 6 weeks. Additionally, he was also instructed to continue with his stretching exercises and rotator cuff strengthening, at least three times a week. Phone Follow-up I spoke with the patient 1 month after his last visit, and he reported that he had not had right shoulder pain for Physical Therapy / Volume 75, Number 9 / September 1995 I believe scapular taping is indicated when a patient is unable to alleviate his or her symptoms, even after education in proper positioning and an appropriate home exercise program. The effectiveness of scapular taping alone has not been demonstrated. I believe, however, that scapular taping should be used in conjunction with other interventions, specifically selected exercises and patient education about modification of performing overhead activities. Scapular taping can be used as an adjunctive therapy to attempt to attain a more favorable scapular alignment and alleviate p i n . The tape should never restrict a patient's range of motion. Additionally, it should allow the patient to perform motions that would have been painful without the tape in place, thus providing an immediate assessment of the Improving the biomechanics of the scapulohumeral and scapulothoracic joints is what ultimately relieves the patient's symptoms. Scapular taping may be one way to improve scapular alignment. Holding the scapula in better alignment with tape may provide a prolonged stretch to the tight structures around the shoulder. Additionally, I believe that this improvement in position helps to increase the subacromial space. Thus, the taping may relieve any excessive tension placed on the involved structures of the impingement. Muscle and collagenous tissue are both very adaptable, and studies16,29-31 have shown that low-load, longduration stretching is more effective than short-term, vigorous stretching. Taping may be one way to achieve this low-load, prolonged-duration stretching. The patient in this case report was seen for 3 months for a total of 10 visits. It is felt that through the use of scapular taping, his treatment was of shorter duration than it would have been without the taping technique. There are several outcome r e p o r t ~ ~ ~ 5 ~ 3 ~ that have documented the time course and results of surgical interventions in patients with rotator cuff injury and bicipital tendinitis, but very few provide the results of those patients treated conservatively. Pink and Jobe33 report a 95% "success" rate for returning an athlete to his or her prior level of competition within 3 months without surgery. Unfortunately, this reporl contained no data to support this claim. Figure 2d. Scapular taping technique: Application of Leukosport" with supporr given under patient's axilla. tape's effectiveness. A thorough examination of the scapula's position at rest and during movements is most important before using taping as a treatment technique.28One difference with scapular taping as compared with patellar taping is that the patients must return to the clinic every 2 to 4 days to be retaped, as they cannot tape themselves. This is also not an easy procedure to teach a family member or 34 / 810 friend unless that person is very familiar with the anatomy and kinesiology of the scapula and shoulder. I believe that paramount to the success of this treatment program is a thorough understanding by the patient of the underlying mechanical cause of his or her pain and the importance of changing faulty movements to prevent the pain from returning.28 There have been few studies of therapeutic outcomes and expected durations of treatment regarding conservative management of shoulder impingement syndromes. Several auth0rs3.~imply that if the patient with shoulder impingement was not better after 3 months of conservative treatment, surgery was indicated. Although taping may have been of benefit in treating this patient, and has been used by this author and other therapists in our clinic with good success, this was not a controlled experimental study but rather a report Physical Therapy / Volume 75, Number 9 / September 1995 tension on the involved structures of the impingement. Poor scapulohumeral rhythm from faulty shoulder and scapular movements presumably contributed to this patient's impingement, but it cannot be said with certainty that the taping and exercise addressed these faults. I can only surmise that the resting position of this patient's right scapula was changed and his pain was relieved as a result of the treatment. Scapular taping may be a useful adjunctive technique for promoting proper scapular position and should be used in conjunction with other conservative methods of treating patients with impingement syndromes of the shoulder. !p --,I: .( 30,'. . Special thanks are given to David R Sinacore, PhD, PT, for his critical review of this manuscript. His assistance and time are both greatly appreciated. I also thank Shirley A Sahrmann, PhD, PT, FAPTA, and Susan S Deusinger, PhD, PT, for their helpful comments and recommendations in regard to this manuscript. Figure 2e. scapular taping technique: Patient with tape in place. He is able topex and abduct his right arm withoutpain. of a single patient. Further studies are necessary before any substantive claims can be made about the efficacy of scapular taping. Conclusion This case report describes the treatment of a patient with anterior impingement of his right shoulder with a taping procedure designed to promote proximal stability of the scapula and therapeutic exercises. The improvements seen in his resting scapular position after this treatment regimen indicate that the taping procedure may have provided a prolonged stretch to short structures and possibly enabled other muscles to function in a more proper manner. Another possible result of the taping procedure is that it could have relieved the excessive Physical Therapy / Volume 75, Number 9 1September 1995 1 Penny JN, Welsh MB. Shoulder impingement syndromes in athletes and their surgical management. Am JSports Med. 1981;9:11-15. 2 Percy EC, Birbrager D, Pin MJ. Snapping scapula: a review of the literature and presentation of 14 patients. Can JSurg. 1988;31:248250. 3 Jobe FW, Bradley JP. The diagnosis and nonoperative treatment of shoulder injuries in athletes. Clin Sports Med. 1989;8:419-438. 4 Hawkins RF, Kennedy JC. Impingement syndromes in athletes. Am J Sports Med. 1980; 8:151-158. 5 Neer CS. Impingement lesions. Clin Ortbop. 1982;73:70-77. 6 Duncan GH, Bushnell MC lavigne GJ. Comparison of verbal and visual analogue scales for measuring the intensity and unpleasantness of experimental pain. Pain. 1989;37:295303. 7 Kendall FP. Muscle Testing and Function. 3rd ed. Baltimore, Md: Williams & Wilkins; 198394-120, 8 Riddle DL, Rothstein JM, Lamb RL. G o n i c ~ metric reliability in a clinical setting. Pbys l%er.1987;67:668-673. 9 Pandya S, Florence JM, King WM, et al. Reliability of goniometric measurements in patients with Duchenne muscular dystrophy. Pbys 7her. 1985;65:1339-1342. 10 Gogia PP, Braatz JH, Rose SJ, Norton BJ Reliability and validity of goniometric measurements at the knee. Pb.vs Ther. 1987;67: 192-195. 11 Clapper MP, Wolf SL. Comparison of the reliability of the Orthoranger and the standard goniometer for assessing active lowerextremity range of motion. Pbys Iher. 1988;68: 214-218. 12 Norkin CC, Levangie PK. Joint Structure and Function: A Comprehensive Analysis. 2nd ed. Philadclphia, Pa: FA Davis Co; 1992:209. 13 Malone TR.Shoulder Injuries. Baltimore, Md: Williams & Wilkins; 1988;1:6-86. 14 Gould JA. Orthopedic and Sports Pbysical Therapy. 2nd ed. St Louis, Mo: CV Mosby Co; 1990:484-521. 15 Inman W, Saunders JB, Abbott LC. Observations on the function of the shoulder joint. JBone Joint Surg. 1944;26:1-30. I6 Donatelli R. Greenfield B. Case study: rehabilitation of a stiff and painful shoulder-a biomechanical approach. J Ortbop Sports Pbys .fier. 1987;9:118-126, 17 Lucas DB. Biomechanics of the shoulder joint. Arch Szrrg. 1973;107:425-432. 18 Hoppenfeld S. Physical fiaminarion of the Spine and Extremities. East Nowalk, Conn: Appleton-Century-Crofts; 1976:ll. 19 Kapandji IA. The Physiology of the,foints. 5th ed. New York, NY: Churchill Livingstone Inc; 1982;1:34-69. 20 Magee DJ. Orthopedic Pbysical Assessment. Philadelphia, Pa: WB Saunders Co; 1987:8687. 21 Clark JM, Harryman DT. Tendons, ligaments, and capsule of the rotator cuff. J Bone Joint Surg /Am/. 1992;74:71%725. 22 Townsend H, Jobe FW, Pink M, Perry J. EMG analysis of the glenohumeral positioning muscles during a baseball rehabilitation program. Am J Sports Med. 1991;19:264-272. 23 Wadsworth CT, Krishnan R, Sear M, et al. Intrarater reliability of manual testing and hand-held dynametric muscle testing. Pbys Ther. 1987;67:1342-1347. 24 Bohannon RW. Manual muscle test scores and dynamometer test scores of knee extension strength. Arch Pbys Med Rebabil. 1986; 67:390-392. 25 Frese E, Brown M, Norton BJ. Clinical reliability of manual muscle testing: middle u-apezius and gluteus medius muscles. Pbys n e r . 1987;67:1072-1076. 26 Gajdosik RL, Bohannon RW. Clinical measurement of range of motion. Pbys n e r . 1987; 67~1867-1872. 27 Donatelli R, Wooden MJ. Ortbopaedic Physical Therapy. New York, NY: Churchill Livingstone Inc; 198949, 165. 28 McConnell J. The management of chondromalacia patellae: a long-term solution. Australian Journal of Physical Therapy. 1986;32: 215-223. 29 Williams PE, Goldspink G. Changes in sarcomere length and physiological properties in immobilized muscle. J A m t . 1978;127:459- 468. 30 Warren CG, Lehmann JF, Koblanski JN. Heat and stretch procedures: an evaluation using rat tail tendon. Arch Pbys Med Rebabil. 1976;57:122-126, 31 Kottke FJ, Pauley DL, Ptak RA. The rationale for prolonged stretching for correction of shortening of connective tissue. A n b Pbys Med Rebabil. 1966;47:345352. 32 Neer CS. Anterior acromioplasty for the chronic impingement syndrome in the shoulder. J Bone Joint S u p /Am/. 1972;54:41-50. 3 3 Pink M, Jobe FW.Shoulder injuries in athletes. CIin Management. 1991;11:39-47. PHARMACOLOGY For an in-depth understanding of how medications influence your patient's 1 2231 4-1 488. This collection of 1 3 articles, from a two-part special series published in Physical Therapy, insightfully explores the relationship between specific clinical conditions, such as cardiovascular and pulmonary disease, diabetes mellitus, Parkinson's disease, and rheumatoid arthritis; pro- 36 / 812 hi , NAME APTA MFMHEK # Physical Therapy / Volume 75, Number 9 / September 199j