Form SS-4 (Rev. January 2009)
advertisement
")
Consumer Agreement for PCA Fiscal Intermediary Services Q Q Q Q Q Q Q Acuerdo del consumidor para servicios de intermediario fiscal de PCA I am a consumer of MassHealth-approved Personal Care Attendant Services (“PCA Services”). As a consumer of PCA Services, I employ my own Personal Care Attendants (“PCAs”). I understand that the wages paid to my PCA(s) are established through a collective bargaining agreement between the PCA Quality Homecare Workforce Council (the Council) and the Union (SEIU Local 1199). As the employer of my PCAs, I must perform certain tasks (“Employer-Required Tasks”) such as paying federal and state taxes and buying workers’ compensation insurance. I understand that MassHealth has hired companies called fiscal intermediaries (“FIs”) who can help consumers like me perform the Employer-Required Tasks. I understand that the fiscal intermediary that my personal care agency has chosen will be my FI. I understand that I must let my FI know, by filling out this form and returning it to my FI, whether I want the FI to help me with my Employer-Required Tasks. Q Q Q Q Q Q If I want the FI to help me with my Employer-Required Tasks, I should choose Option One (Consumer-Delegated Employer Option). Q If I do not want the FI to help me with my EmployerRequired Tasks, I should choose Option Two (ConsumerDirected Employer Option). Q Q Si quisiera que el FI me ayude con las Tareas requeridas del empleador, debo escoger la Opción uno (Opción de empleador: Opción delegada por el consumidor). I understand that I must read the explanations of Option One and Option Two below, and then choose an option by checking one of the boxes at the end of this Agreement. I understand that my personal care agency or my fiscal intermediary can answer any questions I have about Option One or Option Two, give me more information, and help me choose which option is best for me. Si no quisiera que el FI me ayude con las Tareas requeridas del empleador, debo escoger la Opción dos (Opción de empleador: Opción dirigida por el consumidor). Q Q Entiendo que debo leer las explicaciones de la Opción uno y la Opción dos al final de este acuerdo, y luego escoger una opción marcando una de las casillas al final de este Acuerdo. Entiendo que mi agencia de atención individual o mi intermediario fiscal puede responder cualquier pregunta que yo tenga sobre la Opción uno u Opción dos, darme más información y ayudarme a escoger la opción que más me convenga. Q Q Q Q Q Q Q 1 Acuerdo del consumidor para servicios de intermediario fiscal de PCA I am a consumer of MassHealth-approved Personal Care Attendant Services (“PCA Services”). As a consumer of PCA Services, I employ my own Personal Care Attendants (“PCAs”). I understand that the wages paid to my PCA(s) are established through a collective bargaining agreement between the PCA Quality Homecare Workforce Council (the Council) and the Union (SEIU Local 1199). As the employer of my PCAs, I must perform certain tasks (“Employer-Required Tasks”) such as paying federal and state taxes and buying workers’ compensation insurance. I understand that MassHealth has hired companies called fiscal intermediaries (“FIs”) who can help consumers like me perform the Employer-Required Tasks. I understand that the fiscal intermediary that my personal care agency has chosen will be my FI. I understand that I must let my FI know, by filling out this form and returning it to my FI, whether I want the FI to help me with my Employer-Required Tasks. Q Q Q Q Q Q If I want the FI to help me with my Employer-Required Tasks, I should choose Option One (Consumer-Delegated Employer Option). Q If I do not want the FI to help me with my EmployerRequired Tasks, I should choose Option Two (ConsumerDirected Employer Option). Q Q Si no quisiera que el FI me ayude con las Tareas requeridas del empleador, debo escoger la Opción dos (Opción de empleador: Opción dirigida por el consumidor). Q Q Entiendo que debo leer las explicaciones de la Opción uno y la Opción dos al final de este acuerdo, y luego escoger una opción marcando una de las casillas al final de este Acuerdo. Entiendo que mi agencia de atención individual o mi intermediario fiscal puede responder cualquier pregunta que yo tenga sobre la Opción uno u Opción dos, darme más información y ayudarme a escoger la opción que más me convenga. (continúa en la sección de la derecha de la página 2) (continued on left half of page 2) PCA-3 (REV 06/09) Soy consumidor del programa autorizado de MassHealth, Personal Care Attendant Services [Servicios de ayudantes de atención individual (“Servicios PCA”)]. Como consumidor de los Servicios PCA, contrato a mis propios Ayudantes de atención individual (“PCAs“). Entiendo que los salarios pagados a mi(s) PCA(s) se han establecido por medio de un acuerdo de negociación colectiva entre el PCA Quality Homecare Workforce Council (el Concejo) y el Sindicato (SEIU Local 1199). Como empleador de mis PCAs, debo realizar ciertas funciones (“Tareas requeridas del empleador”) tales como pagar los impuestos federales y estatales, y adquirir seguro de accidentes de trabajo. Tengo entendido que MassHealth ha contratado a unas compañías conocidas como intermediarios fiscales (“FIs“), los cuales pueden ayudar a usuarios como yo, a realizar las Tareas requeridas del empleador. Entiendo que el intermediario fiscal que mi agencia de atención individual seleccionó será mi FI. Entiendo que al completar y entregar este formulario a mi FI, le debo informar si deseo sus servicios para asistirme a realizar mis Tareas requeridas del empleador. Si quisiera que el FI me ayude con las Tareas requeridas del empleador, debo escoger la Opción uno (Opción de empleador: Opción delegada por el consumidor). I understand that I must read the explanations of Option One and Option Two below, and then choose an option by checking one of the boxes at the end of this Agreement. I understand that my personal care agency or my fiscal intermediary can answer any questions I have about Option One or Option Two, give me more information, and help me choose which option is best for me. (continúa en la sección de la derecha de la página 2) (continued on left half of page 2) PCA-3 (REV 06/09) Soy consumidor del programa autorizado de MassHealth, Personal Care Attendant Services [Servicios de ayudantes de atención individual (“Servicios PCA”)]. Como consumidor de los Servicios PCA, contrato a mis propios Ayudantes de atención individual (“PCAs“). Entiendo que los salarios pagados a mi(s) PCA(s) se han establecido por medio de un acuerdo de negociación colectiva entre el PCA Quality Homecare Workforce Council (el Concejo) y el Sindicato (SEIU Local 1199). Como empleador de mis PCAs, debo realizar ciertas funciones (“Tareas requeridas del empleador”) tales como pagar los impuestos federales y estatales, y adquirir seguro de accidentes de trabajo. Tengo entendido que MassHealth ha contratado a unas compañías conocidas como intermediarios fiscales (“FIs“), los cuales pueden ayudar a usuarios como yo, a realizar las Tareas requeridas del empleador. Entiendo que el intermediario fiscal que mi agencia de atención individual seleccionó será mi FI. Entiendo que al completar y entregar este formulario a mi FI, le debo informar si deseo sus servicios para asistirme a realizar mis Tareas requeridas del empleador. Consumer Agreement for PCA Fiscal Intermediary Services 1 (continued from left half of page 1) Q (proviene de la sección de la derecha de la página 1) I understand that if I have a surrogate, I must choose Option One, unless I have a legal guardian and my legal guardian chooses Option Two. Q Q Q Q Q Q Q Opción uno, a no ser que tenga un tutor legal y mi tutor legal elija la Opción dos. I understand that no matter which option I choose, I must: Q Entiendo que si tengo un sustituto, debo escoger la (continued from left half of page 1) notify my FI any time I hire or fire a PCA, any time that I move, and any time one of my PCAs moves; notify my FI and my personal care agency when I am admitted to a nursing facility or other inpatient facility. I understand that MassHealth and the FI cannot pay for activity time performed by my PCA when I am in a nursing facility or other inpatient facility, and that any payments made while I am in a nursing facility or inpatient facility are considered fraud and will be reported to the state Bureau of Special Investigations for investigation, and may result in termination of my PCA services as well as other potential penalties; make sure that each week my PCAs sign their time sheets (“Activity Forms”), and fill them out correctly; make sure my PCA activity forms accurately reflect the days and hours my PCA worked for me; send my PCAs’ completed Activity Forms to my FI, following my FI’s instructions, that accurately represent the hours my PCA(s) worked for me; and follow the MassHealth regulations for the Personal Care Attendant Program. My personal care agency can provide me with a copy of these regulations; and I understand that MassHealth and the FI cannot pay my PCA if my PCA is on the List of Excluded Individuals/ Entities (LEIE) maintained by the U.S. Department of Health and Human Services Office of Inspector General (OIG). My FI or my personal care agency can provide me with more information about this. I must have prior authorization for PCA services from MassHealth before my PCAs start working for me. I understand that I may lose my eligibility for PCA services if I do not complete and return this form to my FI as instructed. I understand that no matter which option I choose, I must: notificar a mi FI siempre que contrate o despida a un PCA, siempre que cambie de dirección y siempre que cualquiera de mis PCAs cambie de dirección; Q notificar a mi FI y a mi agencia de atención individual cuando sea internado en una institución de atención especializada u otra institución para pacientes internos. Entiendo que MassHealth y el FI no pueden pagar por el tiempo de las actividades realizadas por mi PCA cuando yo esté en una institución de atención especializada u otra institución para pacientes internos, y que cualquier pago que se haga mientras esté en una institución de atención especializada u otra institución para pacientes internos se considera fraude y será reportado al Departamento de investigaciones especiales para su respectiva investigación, pudiendo dar como resultado la terminación de los servicios de mi PCA al igual que otras multas posibles; Q comprobar que mis PCAs firmen semanalmente su hoja de asistencia (“Formularios de actividades”), y que las llenen correctamente; Q comprobar que los formularios de actividades de mi PCA reflejan con precisión los dias y horas en que mi PCA trabajó para mí; Q enviar los Formularios de actividades de mis PCAs completados a mi FI, de acuerdo a las instrucciones de mi FI, que representan las horas exactas que mi(s) PCA(s) trabajó (trabajaron) para mí; y Q cumplir con las normas de MassHealth sobre el Programa de ayudantes de atención individual. Mi agencia de atención individual me puede dar una copia de dichas normas; y Entiendo que MassHealth y el FI no pueden pagarle al PCA si dicha persona está en la Lista de individuos/ entidades excluidas (LEIE, por sus siglas en inglés) que mantiene la Oficina del Inspector general (OIG, por sus siglas en inglés) del Departamento de salud y servicios humanos de los E.E.U.U. Mi FI o mi agencia de atención individual puede proporcionarme más información sobre esto. Debo tener autorización previa de MassHealth para los servicios PCA antes de que mis PCAs comiencen a trabajar para mí. Entiendo que puedo perder mi eligibilidad para los servicios PCA si no completo y devuelvo este formulario a mi FI tal como aquí se indica. Q (continúa en la sección de la derecha de la página 3) (continued on left half of page 3) 2 I understand that if I have a surrogate, I must choose Option One, unless I have a legal guardian and my legal guardian chooses Option Two. Entiendo que no importa cuál opción escoja, tengo la obligación de: Q Q Q Q Q Q (proviene de la sección de la derecha de la página 1) Q Entiendo que si tengo un sustituto, debo escoger la Opción uno, a no ser que tenga un tutor legal y mi tutor legal elija la Opción dos. Entiendo que no importa cuál opción escoja, tengo la obligación de: notify my FI any time I hire or fire a PCA, any time that I move, and any time one of my PCAs moves; notify my FI and my personal care agency when I am admitted to a nursing facility or other inpatient facility. I understand that MassHealth and the FI cannot pay for activity time performed by my PCA when I am in a nursing facility or other inpatient facility, and that any payments made while I am in a nursing facility or inpatient facility are considered fraud and will be reported to the state Bureau of Special Investigations for investigation, and may result in termination of my PCA services as well as other potential penalties; make sure that each week my PCAs sign their time sheets (“Activity Forms”), and fill them out correctly; make sure my PCA activity forms accurately reflect the days and hours my PCA worked for me; send my PCAs’ completed Activity Forms to my FI, following my FI’s instructions, that accurately represent the hours my PCA(s) worked for me; and notificar a mi FI siempre que contrate o despida a un PCA, siempre que cambie de dirección y siempre que cualquiera de mis PCAs cambie de dirección; Q notificar a mi FI y a mi agencia de atención individual cuando sea internado en una institución de atención especializada u otra institución para pacientes internos. Entiendo que MassHealth y el FI no pueden pagar por el tiempo de las actividades realizadas por mi PCA cuando yo esté en una institución de atención especializada u otra institución para pacientes internos, y que cualquier pago que se haga mientras esté en una institución de atención especializada u otra institución para pacientes internos se considera fraude y será reportado al Departamento de investigaciones especiales para su respectiva investigación, pudiendo dar como resultado la terminación de los servicios de mi PCA al igual que otras multas posibles; Q comprobar que mis PCAs firmen semanalmente su hoja de asistencia (“Formularios de actividades”), y que las llenen correctamente; Q comprobar que los formularios de actividades de mi PCA reflejan con precisión los dias y horas en que mi PCA trabajó para mí; Q enviar los Formularios de actividades de mis PCAs completados a mi FI, de acuerdo a las instrucciones de mi FI, que representan las horas exactas que mi(s) PCA(s) trabajó (trabajaron) para mí; y Q cumplir con las normas de MassHealth sobre el Programa de ayudantes de atención individual. Mi agencia de atención individual me puede dar una copia de dichas normas; y Entiendo que MassHealth y el FI no pueden pagarle al PCA si dicha persona está en la Lista de individuos/ entidades excluidas (LEIE, por sus siglas en inglés) que mantiene la Oficina del Inspector general (OIG, por sus siglas en inglés) del Departamento de salud y servicios humanos de los E.E.U.U. Mi FI o mi agencia de atención individual puede proporcionarme más información sobre esto. Debo tener autorización previa de MassHealth para los servicios PCA antes de que mis PCAs comiencen a trabajar para mí. Entiendo que puedo perder mi eligibilidad para los servicios PCA si no completo y devuelvo este formulario a mi FI tal como aquí se indica. Q follow the MassHealth regulations for the Personal Care Attendant Program. My personal care agency can provide me with a copy of these regulations; and I understand that MassHealth and the FI cannot pay my PCA if my PCA is on the List of Excluded Individuals/ Entities (LEIE) maintained by the U.S. Department of Health and Human Services Office of Inspector General (OIG). My FI or my personal care agency can provide me with more information about this. I must have prior authorization for PCA services from MassHealth before my PCAs start working for me. I understand that I may lose my eligibility for PCA services if I do not complete and return this form to my FI as instructed. (continúa en la sección de la derecha de la página 3) (continued on left half of page 3) 2 (continued from left half of page 2) EXPLANATION OF Option One ( CONSUMER - DELEGATED Q Q (proviene de la sección de la derecha de la página 2) EXPLICACIÓN DE LA EMPLOYER OPTION ) ( OPCIÓN Under Option One, I choose to have my FI perform my Employer-Required Tasks. Under Option One, my FI will: s WRITEOUTMYPAYROLLCHECKSFORMEINTHENAMEOF each PCA that worked for me; s MAKECORRECTWITHHOLDINGSFROMMY0#!S paychecks; s MAKEDEDUCTIONSFOR0#!UNIONDUESANDFEES in accordance with the collective bargaining agreement between the PCA Quality Homecare Workforce Council and the Union (SEIU Local 1199); s SENDALLMONEYWITHHELDFROMMY0#!SPAYCHECKS to the proper agencies; s PAYMYFEDERALSTATEANDLOCALEMPLOYMENTTAXES for me; s PAYMYUNEMPLOYMENTINSURANCETAXESFORME s PURCHASEWORKERSCOMPENSATIONINSURANCEINMY name to cover my PCAs; s send me the completed paychecks every two weeks for me to distribute to my PCAs — OR — Q Q s DEPOSITMY0#!SPAYCHECKSDIRECTLYINTOMY PCAs’ bank accounts if I tell the FI to do this. (I understand that MassHealth regulations require me to inform my PCAs of the option to have my PCA payments direct-deposited into the PCA’s bank account.); s PERFORMOTHER%MPLOYER2EQUIRED4ASKSSUCHAS getting Employer Identification Numbers (EINs) and filling out, filing, and saving copies of other required employment forms; s SENDMESUMMARIESOFMYPAYROLLSANDMYTAX filings; and s SENDMESUMMARIESOFMYREMAININGHOURSOF0#! services when I request this from my FI. If I choose Option One, I understand that I must sign certain forms that will allow the FI to act on my behalf. I understand my PCAs cannot be paid until these forms are completed and returned to my FI. My FI will send me these forms. My FI will also do other Employer-Required Tasks such as getting EINs and filling out, filing, and saving copies of other required employment forms. Opción uno DEL EMPLEADOR : DELEGADA POR EL CONSUMIDOR ) Bajo la Opción uno, opto por solicitar los servicios de un FI para que realice mis Tareas requeridas del empleador. Bajo la Opción uno, mi FI: s ESCRIBIRÉPORMÓLOSCHEQUESDENØMINAANOMBREDE cada uno de los PCA que hayan trabajado para mí; s EFECTUARÉLASRETENCIONESCORRESPONDIENTESDELOS cheques de sueldo de mis PCAs; s hará deducciones para las cuotas y aranceles del sindicato de PCA de acuerdo con la negociación colectiva entre el PCA Quality Homecare Workforce Council y el Sindicato (SEIU Local 1199); s ENVIARÉTODODINERORETENIDODELOSCHEQUES de sueldo de mis PCAs a las agencias correspondientes; s PAGARÉPORMÓMISIMPUESTOSDEEMPLEOFEDERALES estatales y locales; s PAGARÉMISIMPUESTOSDESEGURODEDESEMPLEO por mí; s ADQUIRIRÉELSEGURODEACCIDENTESDETRABAJOENMI nombre para cubrir a mis PCAs; s MEENVIARÉCADADOSSEMANASLOSCHEQUESDE sueldo llenados para que yo los entregue a mis PCAs — O — s DEPOSITARÉLOSCHEQUESDESUELDODIRECTAMENTE en las cuentas bancarias de mis PCAs, si así se lo pido. (Entiendo que las normas de MassHealth requieren que yo informe a mis PCAs de su opción de recibir mis cheques directamente en su cuenta bancaria.); s REALIZARÉOTRAS4AREASPROPIASDEUNEMPLEADOR tales como obtener un Número de identificación del empleador (EINs, por sus siglas en inglés) y completar, presentar y guardar las copias de los demás formularios de empleo obligatorios; s MEENVIARÉRESÞMENESDEMINØMINAY presentaciones de impuestos; y s MEENVIARÉRESÞMENESDELASHORASRESTANTESDEMIS servicios de PCA cuando yo lo solicite de mi FI. Si opto por la Opción uno, entiendo que debo firmar ciertos formularios que le permitirán al FI actuar en mi nombre. Entiendo que mis PCAs no pueden recibir su paga hasta que estos formularios sean llenados y devueltos a mi FI. Mi FI me enviará dichos formularios. Mi Fi también hará otras Tareas requeridas del empleador tales como obtener los EINs y completar, presentar y guardar copias de otros formularios de empleo obligatorios. (continued on left half of page 4) (continúa en la sección de la derecha de la página 4) 3 (continued from left half of page 2) EXPLANATION OF Option One ( CONSUMER - DELEGATED Q Q (proviene de la sección de la derecha de la página 2) EXPLICACIÓN DE LA EMPLOYER OPTION ) ( OPCIÓN Under Option One, I choose to have my FI perform my Employer-Required Tasks. Under Option One, my FI will: s WRITEOUTMYPAYROLLCHECKSFORMEINTHENAMEOF each PCA that worked for me; s MAKECORRECTWITHHOLDINGSFROMMY0#!S paychecks; s MAKEDEDUCTIONSFOR0#!UNIONDUESANDFEES in accordance with the collective bargaining agreement between the PCA Quality Homecare Workforce Council and the Union (SEIU Local 1199); s SENDALLMONEYWITHHELDFROMMY0#!SPAYCHECKS to the proper agencies; s PAYMYFEDERALSTATEANDLOCALEMPLOYMENTTAXES for me; s PAYMYUNEMPLOYMENTINSURANCETAXESFORME s PURCHASEWORKERSCOMPENSATIONINSURANCEINMY name to cover my PCAs; s send me the completed paychecks every two weeks for me to distribute to my PCAs — OR — Q Q s DEPOSITMY0#!SPAYCHECKSDIRECTLYINTOMY PCAs’ bank accounts if I tell the FI to do this. (I understand that MassHealth regulations require me to inform my PCAs of the option to have my PCA payments direct-deposited into the PCA’s bank account.); s PERFORMOTHER%MPLOYER2EQUIRED4ASKSSUCHAS getting Employer Identification Numbers (EINs) and filling out, filing, and saving copies of other required employment forms; s SENDMESUMMARIESOFMYPAYROLLSANDMYTAX filings; and s SENDMESUMMARIESOFMYREMAININGHOURSOF0#! services when I request this from my FI. If I choose Option One, I understand that I must sign certain forms that will allow the FI to act on my behalf. I understand my PCAs cannot be paid until these forms are completed and returned to my FI. My FI will send me these forms. My FI will also do other Employer-Required Tasks such as getting EINs and filling out, filing, and saving copies of other required employment forms. Opción uno DEL EMPLEADOR : DELEGADA POR EL CONSUMIDOR ) Bajo la Opción uno, opto por solicitar los servicios de un FI para que realice mis Tareas requeridas del empleador. Bajo la Opción uno, mi FI: s ESCRIBIRÉPORMÓLOSCHEQUESDENØMINAANOMBREDE cada uno de los PCA que hayan trabajado para mí; s EFECTUARÉLASRETENCIONESCORRESPONDIENTESDELOS cheques de sueldo de mis PCAs; s hará deducciones para las cuotas y aranceles del sindicato de PCA de acuerdo con la negociación colectiva entre el PCA Quality Homecare Workforce Council y el Sindicato (SEIU Local 1199); s ENVIARÉTODODINERORETENIDODELOSCHEQUES de sueldo de mis PCAs a las agencias correspondientes; s PAGARÉPORMÓMISIMPUESTOSDEEMPLEOFEDERALES estatales y locales; s PAGARÉMISIMPUESTOSDESEGURODEDESEMPLEO por mí; s ADQUIRIRÉELSEGURODEACCIDENTESDETRABAJOENMI nombre para cubrir a mis PCAs; s MEENVIARÉCADADOSSEMANASLOSCHEQUESDE sueldo llenados para que yo los entregue a mis PCAs — O — s DEPOSITARÉLOSCHEQUESDESUELDODIRECTAMENTE en las cuentas bancarias de mis PCAs, si así se lo pido. (Entiendo que las normas de MassHealth requieren que yo informe a mis PCAs de su opción de recibir mis cheques directamente en su cuenta bancaria.); s REALIZARÉOTRAS4AREASPROPIASDEUNEMPLEADOR tales como obtener un Número de identificación del empleador (EINs, por sus siglas en inglés) y completar, presentar y guardar las copias de los demás formularios de empleo obligatorios; s MEENVIARÉRESÞMENESDEMINØMINAY presentaciones de impuestos; y s MEENVIARÉRESÞMENESDELASHORASRESTANTESDEMIS servicios de PCA cuando yo lo solicite de mi FI. Si opto por la Opción uno, entiendo que debo firmar ciertos formularios que le permitirán al FI actuar en mi nombre. Entiendo que mis PCAs no pueden recibir su paga hasta que estos formularios sean llenados y devueltos a mi FI. Mi FI me enviará dichos formularios. Mi Fi también hará otras Tareas requeridas del empleador tales como obtener los EINs y completar, presentar y guardar copias de otros formularios de empleo obligatorios. (continued on left half of page 4) (continúa en la sección de la derecha de la página 4) 3 (continued from left half of page 3) EXPLANATION OF (proviene de la sección de la derecha de la página 3) Option Two ( CONSUMER - DIRECTED EXPLICACIÓN DE LA EMPLOYER OPTION ) ( OPCIÓN Opción dos DEL EMPLEADOR : DIRIGIDA POR EL CONSUMIDOR ) Under Option Two, I choose to perform the EmployerRequired Tasks myself. Bajo la Opción dos, opto por realizar por mí mismo las tareas requeridas del empleador. Under Option Two, I will s SUBMITMY0#!SACTIVITYFORMSTOTHE&) as instructed; s ENSURETHATMY0#!ACTIVITYFORMSACCURATELY reflect the day and hours my PCA worked; s PROCESSMYPAYROLLFORALLOFMY0#!S s PAYMY0#!SCORRECTLYANDONTIME s SENDALLMONEYWITHHELDFROMMY0#!SPAYCHECKS to the proper agencies; s PURCHASEWORKERSCOMPENSATIONINSURANCEFOR my PCAs; s PAYMY0#!STHEHOURLYWAGEESTABLISHEDTHROUGH the collective bargaining agreement between the PCA Quality Homecare Workforce Council and the Union (SEIU Local 1199). (The FI can tell me what these rates are.); s file and pay my own federal, state, and local employment taxes; s file and pay my own unemployment insurance taxes; s not hire a PCA whose name appears on the List of Excluded Individuals/Entities (LEIE) maintained by the U.S. Office of Inspector General (OIG). MassHealth and the FI cannot pay a PCA who is on the LEIE. My FI or my personal care agency can provide me with information about this; s make correct withholdings from my PCAs’ paychecks; s make deductions for PCA union dues and fees in accordance with the collective bargaining agreement between the PCA Quality Homecare Workforce Council and the Union (SEIU Local 1199) and forward the dues and fees collected to the Union. I understand I can contact my FI to obtain the phone number for SEIU if I have any questions about this; and s GIVEPROOFTOTHE&)WHENREQUESTEDTHAT)HAVE done all these tasks correctly. Under Option Two, the FI will send me one check every two weeks. I will use this money solely to pay for my Employer-Required Tasks as described above. Q Q (continued on left half of page 5) Bajo la Opción dos: s ENVIARÏLOSFORMULARIOSDEACTIVIDADESDEMIS0#!S al FI tal como se indica; s MEASEGURARÏQUELOSFORMULARIOSDEACTIVIDADES de mis PCAs reflejan con precisión los días y las horas en que mi PCA trabajó; s PROCESARÏMINØMINAPARATODOSMIS0#!S s PAGARÏAMIS0#!SCORRECTAMENTEYATIEMPO s ENVIARÏELDINERORETENIDODELOSCHEQUESDESUELDO de mis PCAs a las agencias correspondientes; s OBTENDRÏELSEGURODEACCIDENTESDETRABAJOPARA mis PCAs; s PAGARÏAMIS0#!ELSALARIOPORHORAESTABLECIDO a través de la negociación colectiva entre el PCA Quality Homecare Workforce Council y el Sindicato (SEIU Local 1199). (El FI puede informarme cuáles son estos salarios.); s PRESENTARÏYPAGARÏPORCUENTAPROPIAMIS impuestos de empleo federales, estatales y locales; s PRESENTARÏYPAGARÏPORCUENTAPROPIAMIS impuestos de seguro de desempleo; s NOCONTRATARÏAUN0#!CUYONOMBREAPARECEEN la Lista de individuos/entidades excluidas (LEIE, por sus siglas en inglés) que mantiene la Oficina del inspector general de los E.E.U.U. (OIG, por sus siglas en inglés). Ni MassHealth ni el FI pueden pagarle a un PCA que no esté en la LEIE. Mi FI o mi agencia de atención personal puede proporcionarme información sobre esto; s HARé las retenciones apropiadas de los cheques de mi(s) PCAs; s HARé deducciones para las cuotas y aranceles del sindicato de PCA de acuerdo con la negociación colectiva entre el PCA Quality Homecare Workforce Council y el Sindicato (SEIU Local 1199) y enviaré las cuotas y aranceles recaudados al Sindicato. Entiendo que puedo comunicarme con mi FI para obtener el número telefónico del SEIU si deseo hacer preguntas al respecto; y 4 s PRESENTARÏLAPRUEBAAMI&)CUANDOASÓLOPIDA de que he realizado todas esas tareas correctamente. Bajo la Opción dos, el FI me enviará un cheque cada dos semanas. Usaré ese dinero, sólo para pagar por mis Tareas requeridas del empleador tal como se describen anteriormente. (continúa en la sección de la derecha de la página 5) (continued from left half of page 3) EXPLANATION OF (proviene de la sección de la derecha de la página 3) Option Two ( CONSUMER - DIRECTED EXPLICACIÓN DE LA EMPLOYER OPTION ) ( OPCIÓN Opción dos DEL EMPLEADOR : DIRIGIDA POR EL CONSUMIDOR ) Under Option Two, I choose to perform the EmployerRequired Tasks myself. Bajo la Opción dos, opto por realizar por mí mismo las tareas requeridas del empleador. Under Option Two, I will s SUBMITMY0#!SACTIVITYFORMSTOTHE&) as instructed; s ENSURETHATMY0#!ACTIVITYFORMSACCURATELY reflect the day and hours my PCA worked; s PROCESSMYPAYROLLFORALLOFMY0#!S s PAYMY0#!SCORRECTLYANDONTIME s SENDALLMONEYWITHHELDFROMMY0#!SPAYCHECKS to the proper agencies; s PURCHASEWORKERSCOMPENSATIONINSURANCEFOR my PCAs; s PAYMY0#!STHEHOURLYWAGEESTABLISHEDTHROUGH the collective bargaining agreement between the PCA Quality Homecare Workforce Council and the Union (SEIU Local 1199). (The FI can tell me what these rates are.); s file and pay my own federal, state, and local employment taxes; s file and pay my own unemployment insurance taxes; s not hire a PCA whose name appears on the List of Excluded Individuals/Entities (LEIE) maintained by the U.S. Office of Inspector General (OIG). MassHealth and the FI cannot pay a PCA who is on the LEIE. My FI or my personal care agency can provide me with information about this; s make correct withholdings from my PCAs’ paychecks; s make deductions for PCA union dues and fees in accordance with the collective bargaining agreement between the PCA Quality Homecare Workforce Council and the Union (SEIU Local 1199) and forward the dues and fees collected to the Union. I understand I can contact my FI to obtain the phone number for SEIU if I have any questions about this; and s GIVEPROOFTOTHE&)WHENREQUESTEDTHAT)HAVE done all these tasks correctly. Under Option Two, the FI will send me one check every two weeks. I will use this money solely to pay for my Employer-Required Tasks as described above. Q Q (continued on left half of page 5) Bajo la Opción dos: s ENVIARÏLOSFORMULARIOSDEACTIVIDADESDEMIS0#!S al FI tal como se indica; s MEASEGURARÏQUELOSFORMULARIOSDEACTIVIDADES de mis PCAs reflejan con precisión los días y las horas en que mi PCA trabajó; s PROCESARÏMINØMINAPARATODOSMIS0#!S s PAGARÏAMIS0#!SCORRECTAMENTEYATIEMPO s ENVIARÏELDINERORETENIDODELOSCHEQUESDESUELDO de mis PCAs a las agencias correspondientes; s OBTENDRÏELSEGURODEACCIDENTESDETRABAJOPARA mis PCAs; s PAGARÏAMIS0#!ELSALARIOPORHORAESTABLECIDO a través de la negociación colectiva entre el PCA Quality Homecare Workforce Council y el Sindicato (SEIU Local 1199). (El FI puede informarme cuáles son estos salarios.); s PRESENTARÏYPAGARÏPORCUENTAPROPIAMIS impuestos de empleo federales, estatales y locales; s PRESENTARÏYPAGARÏPORCUENTAPROPIAMIS impuestos de seguro de desempleo; s NOCONTRATARÏAUN0#!CUYONOMBREAPARECEEN la Lista de individuos/entidades excluidas (LEIE, por sus siglas en inglés) que mantiene la Oficina del inspector general de los E.E.U.U. (OIG, por sus siglas en inglés). Ni MassHealth ni el FI pueden pagarle a un PCA que no esté en la LEIE. Mi FI o mi agencia de atención personal puede proporcionarme información sobre esto; s HARé las retenciones apropiadas de los cheques de mi(s) PCAs; s HARé deducciones para las cuotas y aranceles del sindicato de PCA de acuerdo con la negociación colectiva entre el PCA Quality Homecare Workforce Council y el Sindicato (SEIU Local 1199) y enviaré las cuotas y aranceles recaudados al Sindicato. Entiendo que puedo comunicarme con mi FI para obtener el número telefónico del SEIU si deseo hacer preguntas al respecto; y 4 s PRESENTARÏLAPRUEBAAMI&)CUANDOASÓLOPIDA de que he realizado todas esas tareas correctamente. Bajo la Opción dos, el FI me enviará un cheque cada dos semanas. Usaré ese dinero, sólo para pagar por mis Tareas requeridas del empleador tal como se describen anteriormente. (continúa en la sección de la derecha de la página 5) (proviene de la sección de la derecha de la página 4) (continued from left half of page 4) Here Is My Choice: (proviene de la sección de la derecha de la página 4) (continued from left half of page 4) Here Is My Choice: I choose Option One (Consumer-Delegated option) because I want to have the FI perform my Employer-Required Tasks for me. I choose Option Two (Consumer-Directed option) because I want to perform my Employer-Required Tasks myself. I understand that I can change my option, but that I have to tell the FI at least 10 days before I want to make the change. I choose Option One (Consumer-Delegated option) because I want to have the FI perform my Employer-Required Tasks for me. I choose Option Two (Consumer-Directed option) because I want to perform my Employer-Required Tasks myself. I understand that I can change my option, but that I have to tell the FI at least 10 days before I want to make the change. Esta es mi elección: Elijo la Opción uno (Opción delegada por el consumidor) porque deseo obtener los servicios de un FI para que realice por mí las Tareas requeridas del empleador. Elijo la Opción dos (Opción dirigida por el consumidor) porque deseo realizar por mí mismo las Tareas requeridas del empleador. Entiendo que puedo cambiar mi opción, pero debo informar al FI por lo menos 10 días antes de realizar el cambio. Esta es mi elección: Elijo la Opción uno (Opción delegada por el consumidor) porque deseo obtener los servicios de un FI para que realice por mí las Tareas requeridas del empleador. Elijo la Opción dos (Opción dirigida por el consumidor) porque deseo realizar por mí mismo las Tareas requeridas del empleador. Entiendo que puedo cambiar mi opción, pero debo informar al FI por lo menos 10 días antes de realizar el cambio. Here is my printed name Mi nombre en letra de molde Here is my printed name Mi nombre en letra de molde ________________________________________________ _________________________________________________ ________________________________________________ _________________________________________________ Here is my signature Mi firma Here is my signature Mi firma ________________________________________________ _________________________________________________ ________________________________________________ _________________________________________________ OR O OR O Here is my legal guardian’s signature La firma de mi Tutor legal Here is my legal guardian’s signature La firma de mi Tutor legal ________________________________________________ _________________________________________________ ________________________________________________ _________________________________________________ Today’s date Fecha de hoy Today’s date Fecha de hoy ________________________________________________ _________________________________________________ ________________________________________________ _________________________________________________ Commonwealth of Massachusetts MassHealth Commonwealth of Massachusetts MassHealth Commonwealth of Massachusetts MassHealth Commonwealth of Massachusetts MassHealth 5 5 Form 8821 (Rev. October 2011) Department of the Treasury Internal Revenue Service OMB No. 1545-1165 Tax Information Authorization For IRS Use Only Form Received by: Name a Do not sign this form unless all applicable lines have been completed. a Do not use this form to request a copy or transcript of your tax return. Instead, use Form 4506 or Form 4506-T. Telephone Department of the Treasury Internal Revenue Service Function Date 1 Taxpayer information. Taxpayer(s) must sign and date this form on line 7. Taxpayer name(s) and address (type or print) Taxpayer identification number INCOME TAX WITHHOLDING SS-4, 940, 940R, 940EZ, 941, INCOME TAX WITHHOLDING 941R, 941X, 941C AND EMPLOYMENT TAXES Received by: Name a Do not sign this form unless all applicable lines have been completed. a Do not use this form to request a copy or transcript of your tax return. Instead, use Form 4506 or Form 4506-T. Taxpayer name(s) and address (type or print) Telephone Function Date (c) Year(s) or Period(s) (see the instructions for line 3) Taxpayer identification number Daytime telephone number Plan number (if applicable) 2 Appointee. If you wish to name more than one appointee, attach a list to this form. CAF No. Name and address 0302-31933R PTIN SEREN DERIN OR DESIGNATED REPRESENTATIVE FOR Telephone No. 413-256-6692 STAVROS CENTER FOR INDEPENDENT LIVING Fax No. 413-256-2630 P.O. BOX 2130, AMHERST, MA 01004 Check if new: Address Telephone No. Fax No. 3 Tax matters. The appointee is authorized to inspect and/or receive confidential tax information in any office of the IRS for the tax matters listed on this line. Do not use Form 8821 to request copies of tax returns. (b) Tax Form Number (1040, 941, 720, etc.) For IRS Use Only 1 Taxpayer information. Taxpayer(s) must sign and date this form on line 7. Daytime telephone number (a) Type of Tax (Income, Employment, Excise, etc.) or Civil Penalty 8821 (Rev. October 2011) OMB No. 1545-1165 Tax Information Authorization Plan number (if applicable) 2 Appointee. If you wish to name more than one appointee, attach a list to this form. CAF No. Name and address 0302-31933R PTIN SEREN DERIN OR DESIGNATED REPRESENTATIVE FOR Telephone No. 413-256-6692 STAVROS CENTER FOR INDEPENDENT LIVING Fax No. 413-256-2630 P.O. BOX 2130, AMHERST, MA 01004 Check if new: Address Telephone No. Fax No. 3 Tax matters. The appointee is authorized to inspect and/or receive confidential tax information in any office of the IRS for the tax matters listed on this line. Do not use Form 8821 to request copies of tax returns. (d) Specific Tax Matters (see instr.) TAX LIABILITY 843, W-2, W-2C, W-3, W-3C (a) Type of Tax (Income, Employment, Excise, etc.) or Civil Penalty (b) Tax Form Number (1040, 941, 720, etc.) INCOME TAX WITHHOLDING SS-4, 940, 940R, 940EZ, 941, INCOME TAX WITHHOLDING 941R, 941X, 941C AND EMPLOYMENT TAXES (c) Year(s) or Period(s) (see the instructions for line 3) (d) Specific Tax Matters (see instr.) TAX LIABILITY 843, W-2, W-2C, W-3, W-3C 4 Specific use not recorded on Centralized Authorization File (CAF). If the tax information authorization is for a specific use not recorded on CAF, check this box. See the instructions on page 4. If you check this box, skip lines 5 and 6 . . a 4 Specific use not recorded on Centralized Authorization File (CAF). If the tax information authorization is for a specific use not recorded on CAF, check this box. See the instructions on page 4. If you check this box, skip lines 5 and 6 . . a 5 Disclosure of tax information (you must check a box on line 5a or 5b unless the box on line 4 is checked): a If you want copies of tax information, notices, and other written communications sent to the appointee on an ongoing basis, check this box . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . a Note. Appointees will no longer receive forms, publications and other related materials with the notices. b If you do not want any copies of notices or communications sent to your appointee, check this box . . . . . . . a 5 Disclosure of tax information (you must check a box on line 5a or 5b unless the box on line 4 is checked): a If you want copies of tax information, notices, and other written communications sent to the appointee on an ongoing basis, check this box . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . a Note. Appointees will no longer receive forms, publications and other related materials with the notices. b If you do not want any copies of notices or communications sent to your appointee, check this box . . . . . . . a ✔ 6 Retention/revocation of tax information authorizations. This tax information authorization automatically revokes all prior authorizations for the same tax matters you listed on line 3 above unless you checked the box on line 4. If you do not want to revoke a prior tax information authorization, you must attach a copy of any authorizations you want to remain in effect and check this box . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . a To revoke this tax information authorization, see the instructions on page 4. 6 Retention/revocation of tax information authorizations. This tax information authorization automatically revokes all prior authorizations for the same tax matters you listed on line 3 above unless you checked the box on line 4. If you do not want to revoke a prior tax information authorization, you must attach a copy of any authorizations you want to remain in effect and check this box . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . a To revoke this tax information authorization, see the instructions on page 4. 7 Signature of taxpayer(s). If a tax matter applies to a joint return, either husband or wife must sign. If signed by a corporate officer, partner, guardian, executor, receiver, administrator, trustee, or party other than the taxpayer, I certify that I have the authority to execute this form with respect to the tax matters/periods on line 3 above. 7 Signature of taxpayer(s). If a tax matter applies to a joint return, either husband or wife must sign. If signed by a corporate officer, partner, guardian, executor, receiver, administrator, trustee, or party other than the taxpayer, I certify that I have the authority to execute this form with respect to the tax matters/periods on line 3 above. a IF a IF NOT SIGNED AND DATED, THIS TAX INFORMATION AUTHORIZATION WILL BE RETURNED. a DO Signature Print Name Date Title (if applicable) Signature Print Name PIN number for electronic signature For Privacy Act and Paperwork Reduction Act Notice, see page 4. NOT SIGNED AND DATED, THIS TAX INFORMATION AUTHORIZATION WILL BE RETURNED. a DO NOT SIGN THIS FORM IF IT IS BLANK OR INCOMPLETE. Date Title (if applicable) PIN number for electronic signature Cat. No. 11596P Form 8821 (Rev. 10-2011) ✔ NOT SIGN THIS FORM IF IT IS BLANK OR INCOMPLETE. Signature Print Name Date Title (if applicable) Signature Print Name PIN number for electronic signature For Privacy Act and Paperwork Reduction Act Notice, see page 4. Date Title (if applicable) PIN number for electronic signature Cat. No. 11596P Form 8821 (Rev. 10-2011) Page 2 Form 8821 (Rev. 10-2011) General Instructions Section references are to the Internal Revenue Code unless otherwise noted. What's New Appointees will no longer receive inserts, such as forms, publications, and other related materials, with notices. Purpose of Form Form 8821 authorizes any individual, corporation, firm, organization, or partnership you designate to inspect and/or receive your confidential information in any office of the IRS for the type of tax and the years or periods you list on Form 8821. You may file your own tax information authorization without using Form 8821, but it must include all the information that is requested on Form 8821. Form 8821 does not authorize your appointee to advocate your position with respect to the federal tax laws; to execute waivers, consents, or closing agreements; or to otherwise represent you before the IRS. If you want to authorize an individual to represent you, use Form 2848, Power of Attorney and Declaration of Representative. Use Form 4506, Request for Copy of Tax Return, to get a copy of your tax return. Use Form 4506-T, Request for Transcript of Tax Return, to order: (a) transcript of tax account information and (b) Form W-2 and Form 1099 series information. Use Form 56, Notice Concerning Fiduciary Relationship, to notify the IRS of the existence of a fiduciary relationship. A fiduciary (trustee, executor, administrator, receiver, or guardian) stands in the position of a taxpayer and acts as the taxpayer. Therefore, a fiduciary does not act as an appointee and should not file Form 8821. If a fiduciary wishes to authorize an appointee to inspect and/or receive confidential tax information on behalf of the fiduciary, Form 8821 must be filed and signed by the fiduciary acting in the position of the taxpayer. When To File Form 8821 must be received by the IRS within 120 days of the date it was signed and dated by the taxpayer. Where To File Chart IF you live in . . . Page 2 Form 8821 (Rev. 10-2011) General Instructions Section references are to the Internal Revenue Code unless otherwise noted. What's New Appointees will no longer receive inserts, such as forms, publications, and other related materials, with notices. Purpose of Form Form 8821 authorizes any individual, corporation, firm, organization, or partnership you designate to inspect and/or receive your confidential information in any office of the IRS for the type of tax and the years or periods you list on Form 8821. You may file your own tax information authorization without using Form 8821, but it must include all the information that is requested on Form 8821. Form 8821 does not authorize your appointee to advocate your position with respect to the federal tax laws; to execute waivers, consents, or closing agreements; or to otherwise represent you before the IRS. If you want to authorize an individual to represent you, use Form 2848, Power of Attorney and Declaration of Representative. Use Form 4506, Request for Copy of Tax Return, to get a copy of your tax return. Use Form 4506-T, Request for Transcript of Tax Return, to order: (a) transcript of tax account information and (b) Form W-2 and Form 1099 series information. Use Form 56, Notice Concerning Fiduciary Relationship, to notify the IRS of the existence of a fiduciary relationship. A fiduciary (trustee, executor, administrator, receiver, or guardian) stands in the position of a taxpayer and acts as the taxpayer. Therefore, a fiduciary does not act as an appointee and should not file Form 8821. If a fiduciary wishes to authorize an appointee to inspect and/or receive confidential tax information on behalf of the fiduciary, Form 8821 must be filed and signed by the fiduciary acting in the position of the taxpayer. When To File Form 8821 must be received by the IRS within 120 days of the date it was signed and dated by the taxpayer. Where To File Chart THEN use this address . . . Fax Number* IF you live in . . . THEN use this address . . . Fax Number* Alabama, Arkansas, Connecticut, Delaware, District of Columbia, Florida, Georgia, Illinois, Indiana, Kentucky, Louisiana, Maine, Maryland, Massachusetts, Michigan, Mississippi, New Hampshire, New Jersey, New York, North Carolina, Ohio, Pennsylvania, Rhode Island, South Carolina, Tennessee, Vermont, Virginia, or West Virginia Internal Revenue Service Memphis Accounts Management Center PO Box 268, Stop 8423 Memphis, TN 38101-0268 901-546-4115 Alabama, Arkansas, Connecticut, Delaware, District of Columbia, Florida, Georgia, Illinois, Indiana, Kentucky, Louisiana, Maine, Maryland, Massachusetts, Michigan, Mississippi, New Hampshire, New Jersey, New York, North Carolina, Ohio, Pennsylvania, Rhode Island, South Carolina, Tennessee, Vermont, Virginia, or West Virginia Internal Revenue Service Memphis Accounts Management Center PO Box 268, Stop 8423 Memphis, TN 38101-0268 901-546-4115 Alaska, Arizona, California, Colorado, Hawaii, Idaho, Iowa, Kansas, Minnesota, Missouri, Montana, Nebraska, Nevada, New Mexico, North Dakota, Oklahoma, Oregon, South Dakota, Texas, Utah, Washington, Wisconsin, or Wyoming Internal Revenue Service 1973 N. Rulon White Blvd. MS 6737 Ogden, UT 84404 801-620-4249 Alaska, Arizona, California, Colorado, Hawaii, Idaho, Iowa, Kansas, Minnesota, Missouri, Montana, Nebraska, Nevada, New Mexico, North Dakota, Oklahoma, Oregon, South Dakota, Texas, Utah, Washington, Wisconsin, or Wyoming Internal Revenue Service 1973 N. Rulon White Blvd. MS 6737 Ogden, UT 84404 801-620-4249 All APO and FPO addresses, American Samoa, nonpermanent residents of Guam or the Virgin Islands**, Puerto Rico (or if excluding income under section 933), a foreign country, U.S. citizens and those filing Form 2555, 2555-EZ, or 4563. Internal Revenue Service International CAF 2970 Market St. MS 3-E08.123 Philadelphia, PA 19104 267-941-1017 All APO and FPO addresses, American Samoa, nonpermanent residents of Guam or the Virgin Islands**, Puerto Rico (or if excluding income under section 933), a foreign country, U.S. citizens and those filing Form 2555, 2555-EZ, or 4563. Internal Revenue Service International CAF 2970 Market St. MS 3-E08.123 Philadelphia, PA 19104 267-941-1017 *These numbers may change without notice. **Permanent residents of Guam should use Department of Taxation, Government of Guam, P.O. Box 23607, GMF, GU 96921; permanent residents of the Virgin Islands should use: V.I. Bureau of Internal Revenue, 9601 Estate Thomas Charlotte Amalie, St. Thomas, V.I. 00802. *These numbers may change without notice. **Permanent residents of Guam should use Department of Taxation, Government of Guam, P.O. Box 23607, GMF, GU 96921; permanent residents of the Virgin Islands should use: V.I. Bureau of Internal Revenue, 9601 Estate Thomas Charlotte Amalie, St. Thomas, V.I. 00802. Page 3 Form 8821 (Rev. 10-2011) Where To File Generally, mail or fax Form 8821 directly to the IRS. See the Where To File Chart, above. Exceptions are listed below. If Form 8821 is for a specific tax matter, mail or fax it to the office handling that matter. For more information, see the instructions for line 4. Your appointee may be able to file Form 8821 electronically with the IRS from the IRS website. For more information, go to www.irs.gov. Under the Tax Professionals tab, click on e-services–Online Tools for Tax Professionals. If you complete Form 8821 for electronic signature authorization, do not file a Form 8821 with the IRS. Instead, give it to your appointee, who will retain the document. Revocation of an Existing Tax Information Authorization If you want to revoke an existing tax information authorization and do not want to name a new appointee, send a copy of the previously executed tax information authorization to the IRS, using the Where To File Chart, above. The copy of the tax information authorization must have a current signature and date of the taxpayer under the original signature on line 7. Write “REVOKE” across the top of Form 8821. Specific Instructions Where To File Specific Instructions Line 1. Taxpayer Information Generally, mail or fax Form 8821 directly to the IRS. See the Where To File Chart, above. Exceptions are listed below. If Form 8821 is for a specific tax matter, mail or fax it to the office handling that matter. For more information, see the instructions for line 4. Your appointee may be able to file Form 8821 electronically with the IRS from the IRS website. For more information, go to www.irs.gov. Under the Tax Professionals tab, click on e-services–Online Tools for Tax Professionals. If you complete Form 8821 for electronic signature authorization, do not file a Form 8821 with the IRS. Instead, give it to your appointee, who will retain the document. Line 1. Taxpayer Information Individuals. Enter your name, TIN, and your street address in the space provided. Do not enter your appointee’s address or post office box. If a joint return is used, also enter your spouse’s name and TIN. Also enter your EIN if applicable. Corporations, partnerships, or associations. Enter the name, EIN, and business address. Employee plan or exempt organization. Enter the name, address, and EIN of the plan sponsor or exempt organization, and the plan name and three-digit plan number. Trust. Enter the name, title, and address of the trustee, and the name and EIN of the trust. Estate. Enter the name, title, and address of the decedent’s executor/personal representative, and the name and identification number of the estate. The identification number for an estate includes both the EIN, if the estate has one, and the decedent’s TIN. Line 2. Appointee To revoke a specific use tax information authorization, send the tax information authorization or statement of revocation to the IRS office handling your case, using the above instructions. Enter your appointee’s full name. Use the identical full name on all submissions and correspondence. Enter the nine-digit CAF number for each appointee. If an appointee has a CAF number for any previously filed Form 8821 or power of attorney (Form 2848), use that number. If a CAF number has not been assigned, enter “NONE,” and the IRS will issue one directly to your appointee. The IRS does not assign CAF numbers to requests for employee plans and exempt organizations. If you want to name more than one appointee, indicate so on this line and attach a list of appointees to Form 8821. Check the appropriate box to indicate if either the address, telephone number, or fax number is new since a CAF number was assigned. Taxpayer Identification Numbers (TINs) If you do not have a copy of the tax information authorization you want to revoke, send a statement to the IRS. In the statement, indicate that the authority of the appointee is revoked, list the name and address of each recognized appointee whose authority is revoked, list the tax matters and periods, and sign and date the statement. If you are completely revoking the authority of the appointee, state “remove all years/periods” instead of listing the specific tax matters, years, or periods on the form. TINs are used to identify taxpayer information with corresponding tax returns. It is important that you furnish correct names, social security numbers (SSNs), individual taxpayer identification numbers (ITINs), or employer identification numbers (EINs) so that the IRS can respond to your request. Partnership Items Sections 6221-6234 authorize a Tax Matters Partner to perform certain acts on behalf of an affected partnership. Rules governing the use of Form 8821 do not replace any provisions of these sections. Appointee Address Change If the appointee's address has changed, a new Form 8821 is not required. The appointee can send a written notification that includes the new information and their signature to the location where the Form 8821 was filed. Page 3 Form 8821 (Rev. 10-2011) Revocation of an Existing Tax Information Authorization If you want to revoke an existing tax information authorization and do not want to name a new appointee, send a copy of the previously executed tax information authorization to the IRS, using the Where To File Chart, above. The copy of the tax information authorization must have a current signature and date of the taxpayer under the original signature on line 7. Write “REVOKE” across the top of Form 8821. Individuals. Enter your name, TIN, and your street address in the space provided. Do not enter your appointee’s address or post office box. If a joint return is used, also enter your spouse’s name and TIN. Also enter your EIN if applicable. Corporations, partnerships, or associations. Enter the name, EIN, and business address. Employee plan or exempt organization. Enter the name, address, and EIN of the plan sponsor or exempt organization, and the plan name and three-digit plan number. Trust. Enter the name, title, and address of the trustee, and the name and EIN of the trust. Estate. Enter the name, title, and address of the decedent’s executor/personal representative, and the name and identification number of the estate. The identification number for an estate includes both the EIN, if the estate has one, and the decedent’s TIN. Line 2. Appointee To revoke a specific use tax information authorization, send the tax information authorization or statement of revocation to the IRS office handling your case, using the above instructions. Enter your appointee’s full name. Use the identical full name on all submissions and correspondence. Enter the nine-digit CAF number for each appointee. If an appointee has a CAF number for any previously filed Form 8821 or power of attorney (Form 2848), use that number. If a CAF number has not been assigned, enter “NONE,” and the IRS will issue one directly to your appointee. The IRS does not assign CAF numbers to requests for employee plans and exempt organizations. If you want to name more than one appointee, indicate so on this line and attach a list of appointees to Form 8821. Check the appropriate box to indicate if either the address, telephone number, or fax number is new since a CAF number was assigned. Line 3. Matters Taxpayer Identification Numbers (TINs) Line 3. Matters Enter the type of tax, the tax form number, the years or periods, and the specific matter. Enter “Not applicable,” in any of the columns that do not apply. For example, you may list “Income, 1040” for calendar year “2006” and “Excise, 720” for “2006” (this covers all quarters in 2006). For multiple years or a series of inclusive periods, including quarterly periods, you may list 2004 through (thru or a hyphen) 2006. For example, “2004 thru 2006” or “2nd 2005-3rd 2006.” For fiscal years, enter the ending year and month, using the YYYYMM format. Do not use a general reference such as “All years,” “All periods,” or “All taxes.” Any tax information authorization with a general reference will be returned. You may list the current year or period and any tax years or periods that have already ended as of the date you sign the tax information authorization. However, you may include on a tax information authorization only future tax periods that end no later than 3 years after the date the tax information authorization is received by the IRS. The 3 future periods are determined starting after December 31 of the year the tax information authorization is received by the IRS. You must enter the type of tax, the tax form number, and the future year(s) or period(s). If the matter relates to estate tax, enter the date of the decedent’s death instead of the year or period. TINs are used to identify taxpayer information with corresponding tax returns. It is important that you furnish correct names, social security numbers (SSNs), individual taxpayer identification numbers (ITINs), or employer identification numbers (EINs) so that the IRS can respond to your request. Enter the type of tax, the tax form number, the years or periods, and the specific matter. Enter “Not applicable,” in any of the columns that do not apply. For example, you may list “Income, 1040” for calendar year “2006” and “Excise, 720” for “2006” (this covers all quarters in 2006). For multiple years or a series of inclusive periods, including quarterly periods, you may list 2004 through (thru or a hyphen) 2006. For example, “2004 thru 2006” or “2nd 2005-3rd 2006.” For fiscal years, enter the ending year and month, using the YYYYMM format. Do not use a general reference such as “All years,” “All periods,” or “All taxes.” Any tax information authorization with a general reference will be returned. You may list the current year or period and any tax years or periods that have already ended as of the date you sign the tax information authorization. However, you may include on a tax information authorization only future tax periods that end no later than 3 years after the date the tax information authorization is received by the IRS. The 3 future periods are determined starting after December 31 of the year the tax information authorization is received by the IRS. You must enter the type of tax, the tax form number, and the future year(s) or period(s). If the matter relates to estate tax, enter the date of the decedent’s death instead of the year or period. If you do not have a copy of the tax information authorization you want to revoke, send a statement to the IRS. In the statement, indicate that the authority of the appointee is revoked, list the name and address of each recognized appointee whose authority is revoked, list the tax matters and periods, and sign and date the statement. If you are completely revoking the authority of the appointee, state “remove all years/periods” instead of listing the specific tax matters, years, or periods on the form. Partnership Items Sections 6221-6234 authorize a Tax Matters Partner to perform certain acts on behalf of an affected partnership. Rules governing the use of Form 8821 do not replace any provisions of these sections. Appointee Address Change If the appointee's address has changed, a new Form 8821 is not required. The appointee can send a written notification that includes the new information and their signature to the location where the Form 8821 was filed. Form 8821 (Rev. 10-2011) In column (d), enter any specific information you want the IRS to provide. Examples of column (d) information are: lien information, a balance due amount, a specific tax schedule, or a tax liability. For requests regarding Form 8802, Application for United States Residency Certification, enter “Form 8802” in column (d) and check the specific use box on line 4. Also, enter the appointee’s information as instructed on Form 8802. Note. If the taxpayer is subject to penalties related to an individual retirement account (IRA) (for example, a penalty for excess contributions) enter, “IRA civil penalty” on line 3, column a. Line 4. Specific Use Not Recorded on CAF Generally, the IRS records all tax information authorizations on the CAF system. However, authorizations relating to a specific issue are not recorded. Check the box on line 4 if Form 8821 is filed for any of the following reasons: (a) requests to disclose information to loan companies or educational institutions, (b) requests to disclose information to federal or state agency investigators for background checks, (c) application for EIN, or (d) claims filed on Form 843, Claim for Refund and Request for Abatement. If you check the box on line 4, your appointee should mail or fax Form 8821 to the IRS office handling the matter. Otherwise, your appointee should bring a copy of Form 8821 to each appointment to inspect or receive information. A specific-use tax information authorization will not revoke any prior tax information authorizations. Line 6. Retention/Revocation of Tax Information Authorizations Check the box on this line and attach a copy of the tax information authorization you do not want to revoke. The filing of Form 8821 will not revoke any Form 2848 that is in effect. Line 7. Signature of Taxpayer(s) Individuals. You must sign and date the authorization. Either husband or wife must sign if Form 8821 applies to a joint return. Corporations. Generally, Form 8821 can be signed by: (a) an officer having legal authority to bind the corporation, (b) any person designated by the board of directors or other governing body, (c) any officer or employee on written request by any principal officer and attested to by the secretary or other officer, and (d) any other person authorized to access information under section 6103(e). Partnerships. Generally, Form 8821 can be signed by any person who was a member of the partnership during any part of the tax period covered by Form 8821. See Partnership Items, above. Page 4 All others. See section 6103(e) if the taxpayer has died, is insolvent, is a dissolved corporation, or if a trustee, guardian, executor, receiver, or administrator is acting for the taxpayer. Privacy Act and Paperwork Reduction Act Notice We ask for the information on this form to carry out the Internal Revenue laws of the United States. Form 8821 authorizes the IRS to disclose your confidential tax information to the person you appoint. This form is provided for your convenience and its use is voluntary. The information is used by the IRS to determine what confidential tax information your appointee can inspect and/or receive. Section 6103(c) and its regulations require you to provide this information if you want to designate an appointee to inspect and/or receive your confidential tax information. Under section 6109, you must disclose your identification number. If you do not provide all the information requested on this form, we may not be able to honor the authorization. Providing false or fraudulent information may subject you to penalties. We may disclose this information to the Department of Justice for civil or criminal litigation, and to cities, states, the District of Columbia, and U.S. commonwealths and possessions for use in administering their tax laws. We may also disclose this information to other countries under a tax treaty, to federal and state agencies to enforce federal nontax criminal laws, or to federal law enforcement and intelligence agencies to combat terrorism. You are not required to provide the information requested on a form that is subject to the Paperwork Reduction Act unless the form displays a valid OMB control number. Books or records relating to a form or its instructions must be retained as long as their contents may become material in the administration of any Internal Revenue law. The time needed to complete and file this form will vary depending on individual circumstances. The estimated average time is: Recordkeeping, 6 min.; Learning about the law or the form, 12 min.; Preparing the form, 24 min.; Copying and sending the form to the IRS, 20 min. If you have comments concerning the accuracy of these time estimates or suggestions for making Form 8821 simpler, we would be happy to hear from you. You can write to Internal Revenue Service, Tax Products Coordinating Committee, SE:W:CAR:MP:T:M:S, 1111 Constitution Ave. NW, IR-6526, Washington, DC 20224. Do not send Form 8821 to this address. Instead, see the Where To File Chart earlier. Form 8821 (Rev. 10-2011) In column (d), enter any specific information you want the IRS to provide. Examples of column (d) information are: lien information, a balance due amount, a specific tax schedule, or a tax liability. For requests regarding Form 8802, Application for United States Residency Certification, enter “Form 8802” in column (d) and check the specific use box on line 4. Also, enter the appointee’s information as instructed on Form 8802. Note. If the taxpayer is subject to penalties related to an individual retirement account (IRA) (for example, a penalty for excess contributions) enter, “IRA civil penalty” on line 3, column a. Line 4. Specific Use Not Recorded on CAF Generally, the IRS records all tax information authorizations on the CAF system. However, authorizations relating to a specific issue are not recorded. Check the box on line 4 if Form 8821 is filed for any of the following reasons: (a) requests to disclose information to loan companies or educational institutions, (b) requests to disclose information to federal or state agency investigators for background checks, (c) application for EIN, or (d) claims filed on Form 843, Claim for Refund and Request for Abatement. If you check the box on line 4, your appointee should mail or fax Form 8821 to the IRS office handling the matter. Otherwise, your appointee should bring a copy of Form 8821 to each appointment to inspect or receive information. A specific-use tax information authorization will not revoke any prior tax information authorizations. Line 6. Retention/Revocation of Tax Information Authorizations Check the box on this line and attach a copy of the tax information authorization you do not want to revoke. The filing of Form 8821 will not revoke any Form 2848 that is in effect. Line 7. Signature of Taxpayer(s) Individuals. You must sign and date the authorization. Either husband or wife must sign if Form 8821 applies to a joint return. Corporations. Generally, Form 8821 can be signed by: (a) an officer having legal authority to bind the corporation, (b) any person designated by the board of directors or other governing body, (c) any officer or employee on written request by any principal officer and attested to by the secretary or other officer, and (d) any other person authorized to access information under section 6103(e). Partnerships. Generally, Form 8821 can be signed by any person who was a member of the partnership during any part of the tax period covered by Form 8821. See Partnership Items, above. Page 4 All others. See section 6103(e) if the taxpayer has died, is insolvent, is a dissolved corporation, or if a trustee, guardian, executor, receiver, or administrator is acting for the taxpayer. Privacy Act and Paperwork Reduction Act Notice We ask for the information on this form to carry out the Internal Revenue laws of the United States. Form 8821 authorizes the IRS to disclose your confidential tax information to the person you appoint. This form is provided for your convenience and its use is voluntary. The information is used by the IRS to determine what confidential tax information your appointee can inspect and/or receive. Section 6103(c) and its regulations require you to provide this information if you want to designate an appointee to inspect and/or receive your confidential tax information. Under section 6109, you must disclose your identification number. If you do not provide all the information requested on this form, we may not be able to honor the authorization. Providing false or fraudulent information may subject you to penalties. We may disclose this information to the Department of Justice for civil or criminal litigation, and to cities, states, the District of Columbia, and U.S. commonwealths and possessions for use in administering their tax laws. We may also disclose this information to other countries under a tax treaty, to federal and state agencies to enforce federal nontax criminal laws, or to federal law enforcement and intelligence agencies to combat terrorism. You are not required to provide the information requested on a form that is subject to the Paperwork Reduction Act unless the form displays a valid OMB control number. Books or records relating to a form or its instructions must be retained as long as their contents may become material in the administration of any Internal Revenue law. The time needed to complete and file this form will vary depending on individual circumstances. The estimated average time is: Recordkeeping, 6 min.; Learning about the law or the form, 12 min.; Preparing the form, 24 min.; Copying and sending the form to the IRS, 20 min. If you have comments concerning the accuracy of these time estimates or suggestions for making Form 8821 simpler, we would be happy to hear from you. You can write to Internal Revenue Service, Tax Products Coordinating Committee, SE:W:CAR:MP:T:M:S, 1111 Constitution Ave. NW, IR-6526, Washington, DC 20224. Do not send Form 8821 to this address. Instead, see the Where To File Chart earlier. SS-4 Application for Employer Identification Number (Rev. January 2010) Type or print clearly. Department of the Treasury Internal Revenue Service 8a 8c 9a (For use by employers, corporations, partnerships, trusts, estates, churches, government agencies, Indian tribal entities, certain individuals, and others.) 10 Form Keep a copy for your records. 2 Trade name of business (if different from name on line 1) 3 Executor, administrator, trustee, “care of” name 4a Mailing address (room, apt., suite no. and street, or P.O. box) 5a Street address (if different) (Do not enter a P.O. box.) ,HHCSR P.O. Box 2130 City, state, and ZIP code (if foreign, see instructions) 5b City, state, and ZIP code (if foreign, see instructions) Amherst, MA 01004 6 County and state where principal business is located 7a Name of responsible party Is this application for a limited liability company (LLC) (or a foreign equivalent)? 7b SSN, ITIN, or EIN 8b If 8a is “Yes,” enter the number of LLC members ✔ No Yes Application for Employer Identification Number Department of the Treasury Internal Revenue Service Legal name of entity (or individual) for whom the EIN is being requested 4b SS-4 (Rev. January 2010) 1 8a ✔ No Yes If 8a is “Yes,” was the LLC organized in the United States? Type of entity (check only one box). Caution. If 8a is “Yes,” see the instructions for the correct box to check. 8c 9a (For use by employers, corporations, partnerships, trusts, estates, churches, government agencies, Indian tribal entities, certain individuals, and others.) 2 Trade name of business (if different from name on line 1) 3 Executor, administrator, trustee, “care of” name 4a Mailing address (room, apt., suite no. and street, or P.O. box) 5a Street address (if different) (Do not enter a P.O. box.) 5b City, state, and ZIP code (if foreign, see instructions) ,HHCSR P.O. Box 2130 4b City, state, and ZIP code (if foreign, see instructions) Amherst, MA 01004 6 County and state where principal business is located 7a Name of responsible party Is this application for a limited liability company (LLC) (or a foreign equivalent)? Sole proprietor (SSN) Plan administrator (TIN) Partnership Trust (TIN of grantor) Corporation (enter form number to be filed) Estate (SSN of decedent) Plan administrator (TIN) Trust (TIN of grantor) National Guard State/local government Church or church-controlled organization Farmers’ cooperative Federal government/military Church or church-controlled organization Farmers’ cooperative Federal government/military Other nonprofit organization (specify) ✔ Other (specify) HHCSR If a corporation, name the state or foreign country (if applicable) where incorporated Reason for applying (check only one box) State REMIC Indian tribal governments/enterprises Group Exemption Number (GEN) if any Foreign country Banking purpose (specify purpose) 9b 10 Changed type of organization (specify new type) Other nonprofit organization (specify) ✔ Other (specify) HHCSR If a corporation, name the state or foreign country (if applicable) where incorporated Reason for applying (check only one box) Started new business (specify type) Created a trust (specify type) Hired employees (Check the box and see line 13.) December If you expect your employment tax liability to be $1,000 Highest number of employees expected in the next 12 months (enter -0- if none). or less in a full calendar year and want to file Form 944 annually instead of Forms 941 quarterly, check here. If no employees expected, skip line 14. (Your employment tax liability generally will be $1,000 or less if you expect to pay $4,000 or less in total Agricultural Household Other wages.) If you do not check this box, you must file 0 0 0 Form 941 for every quarter. First date wages or annuities were paid (month, day, year). Note. If applicant is a withholding agent, enter date income will first be paid to nonresident alien (month, day, year) N/A Check one box that best describes the principal activity of your business. Rental & leasing Health care & social assistance Accommodation & food service Wholesale-agent/broker Retail Wholesale-other Transportation & warehousing Finance & insurance ✔ Other (specify) HHCSR Real estate Manufacturing Indicate principal line of merchandise sold, specific construction work done, products produced, or services provided. Banking purpose (specify purpose) Changed type of organization (specify new type) 11 Created a trust (specify type) Compliance with IRS withholding regulations Created a pension plan (specify type) ✔ Other (specify) HHCSR Date business started or acquired (month, day, year). See instructions. 12 Closing month of accounting year December If you expect your employment tax liability to be $1,000 Highest number of employees expected in the next 12 months (enter -0- if none). or less in a full calendar year and want to file Form 944 annually instead of Forms 941 quarterly, check here. If no employees expected, skip line 14. (Your employment tax liability generally will be $1,000 or less if you expect to pay $4,000 or less in total Agricultural Household Other wages.) If you do not check this box, you must file 0 0 0 Form 941 for every quarter. First date wages or annuities were paid (month, day, year). Note. If applicant is a withholding agent, enter date income will first be paid to nonresident alien (month, day, year) N/A 14 13 15 16 Check one box that best describes the principal activity of your business. Health care & social assistance Wholesale-agent/broker Accommodation & food service Retail Transportation & warehousing Wholesale-other Finance & insurance ✔ Real estate Manufacturing Other (specify) HHCSR Indicate principal line of merchandise sold, specific construction work done, products produced, or services provided. Construction 17 Yes ✔ No 18 Rental & leasing Has the applicant entity shown on line 1 ever applied for and received an EIN? If “Yes,” write previous EIN here Complete this section only if you want to authorize the named individual to receive the entity’s EIN and answer questions about the completion of this form. Designee’s name Designee’s telephone number (include area code) Seren Derin, Stavros Ctr For Ind Liv Inc. ( 413 ) Address and ZIP code P.O. Box 2130, Amherst, MA 01002 Name and title (type or print clearly) 256-6692 Designee’s fax number (include area code) ( 413 ) Under penalties of perjury, I declare that I have examined this application, and to the best of my knowledge and belief, it is true, correct, and complete. ( ) ✔ No Complete this section only if you want to authorize the named individual to receive the entity’s EIN and answer questions about the completion of this form. Third Party Designee 256-3516 Applicant’s telephone number (include area code) Yes Designee’s name Designee’s telephone number (include area code) Seren Derin, Stavros Ctr For Ind Liv Inc. ( 413 ) Address and ZIP code P.O. Box 2130, Amherst, MA 01002 ( 413 ) Under penalties of perjury, I declare that I have examined this application, and to the best of my knowledge and belief, it is true, correct, and complete. Name and title (type or print clearly) Date For Privacy Act and Paperwork Reduction Act Notice, see separate instructions. ( Cat. No. 16055N ) Form (Rev. 1-2010) 256-3516 Applicant’s telephone number (include area code) ( ) Applicant’s fax number (include area code) Signature SS-4 256-6692 Designee’s fax number (include area code) Applicant’s fax number (include area code) HHCSR Has the applicant entity shown on line 1 ever applied for and received an EIN? If “Yes,” write previous EIN here Third Party Designee State REMIC Indian tribal governments/enterprises Group Exemption Number (GEN) if any Foreign country Purchased going business Compliance with IRS withholding regulations Created a pension plan (specify type) ✔ Other (specify) HHCSR Date business started or acquired (month, day, year). See instructions. 12 Closing month of accounting year Signature ✔ No Yes Personal service corporation HHCSR 18 If 8a is “Yes,” enter the number of LLC members State/local government Construction 17 8b ✔ No Yes National Guard 14 16 SSN, ITIN, or EIN Personal service corporation Hired employees (Check the box and see line 13.) 15 7b If 8a is “Yes,” was the LLC organized in the United States? Type of entity (check only one box). Caution. If 8a is “Yes,” see the instructions for the correct box to check. Purchased going business 13 Keep a copy for your records. Legal name of entity (or individual) for whom the EIN is being requested Estate (SSN of decedent) Started new business (specify type) 11 OMB No. 1545-0003 EIN 1 Partnership See separate instructions for each line. Sole proprietor (SSN) Corporation (enter form number to be filed) 9b See separate instructions for each line. OMB No. 1545-0003 EIN Type or print clearly. Form Date For Privacy Act and Paperwork Reduction Act Notice, see separate instructions. ( Cat. No. 16055N ) Form SS-4 (Rev. 1-2010) Form SS-4 (Rev. 1-2010) Page 2 Form SS-4 (Rev. 1-2010) Page Do I Need an EIN? Do I Need an EIN? File Form SS-4 if the applicant entity does not already have an EIN but is required to show an EIN on any return, statement, or other document.1 See also the separate instructions for each line on Form SS-4. IF the applicant... Started a new business AND... Hired (or will hire) employees, including household employees File Form SS-4 if the applicant entity does not already have an EIN but is required to show an EIN on any return, statement, or other document.1 See also the separate instructions for each line on Form SS-4. THEN... Complete lines 1, 2, 4a–8a, 8b–c (if applicable), 9a, 9b (if applicable), and 10–14 and 16–18. IF the applicant... Started a new business AND... Does not already have an EIN Complete lines 1, 2, 4a–6, 7a–b (if applicable), 8a, 8b–c (if applicable), 9a, 9b (if applicable), 10–18. Hired (or will hire) employees, including household employees Does not already have an EIN Complete lines 1, 2, 4a–6, 7a–b (if applicable), 8a, 8b–c (if applicable), 9a, 9b (if applicable), 10–18. Opened a bank account Needs an EIN for banking purposes only Complete lines 1–5b, 7a–b (if applicable), 8a, 8b–c (if applicable), 9a, 9b (if applicable), 10, and 18. Opened a bank account Needs an EIN for banking purposes only Complete lines 1–5b, 7a–b (if applicable), 8a, 8b–c (if applicable), 9a, 9b (if applicable), 10, and 18. Changed type of organization Either the legal character of the organization or its ownership changed (for example, you incorporate a sole proprietorship or form a partnership) 2 Complete lines 1–18 (as applicable). Changed type of organization Either the legal character of the organization or its ownership changed (for example, you incorporate a sole proprietorship or form a partnership) 2 Complete lines 1–18 (as applicable). Purchased a going business 3 Created a trust Does not already have an EIN The trust is other than a grantor trust or an IRA trust 4 Complete lines 1–18 (as applicable). Complete lines 1–18 (as applicable). Purchased a going business 3 Created a trust Does not already have an EIN The trust is other than a grantor trust or an IRA trust 4 Complete lines 1–18 (as applicable). Complete lines 1–18 (as applicable). Created a pension plan as a plan administrator 5 Needs an EIN for reporting purposes Complete lines 1, 3, 4a–5b, 9a, 10, and 18. Created a pension plan as a plan administrator 5 Needs an EIN for reporting purposes Complete lines 1, 3, 4a–5b, 9a, 10, and 18. Is a foreign person needing an EIN to comply with IRS withholding regulations Needs an EIN to complete a Form W-8 (other than Form W-8ECI), avoid withholding on portfolio assets, or claim tax treaty benefits 6 Complete lines 1–5b, 7a–b (SSN or ITIN optional), 8a, 8b–c (if applicable), 9a, 9b (if applicable), 10, and 18. Is a foreign person needing an EIN to comply with IRS withholding regulations Needs an EIN to complete a Form W-8 (other than Form W-8ECI), avoid withholding on portfolio assets, or claim tax treaty benefits 6 Complete lines 1–5b, 7a–b (SSN or ITIN optional), 8a, 8b–c (if applicable), 9a, 9b (if applicable), 10, and 18. Is administering an estate Needs an EIN to report estate income on Form 1041 Complete lines 1–6, 9a, 10–12, 13–17 (if applicable), and 18. Is administering an estate Needs an EIN to report estate income on Form 1041 Complete lines 1–6, 9a, 10–12, 13–17 (if applicable), and 18. Is a withholding agent for taxes on non-wage income paid to an alien (i.e., individual, corporation, or partnership, etc.) Is a state or local agency Is an agent, broker, fiduciary, manager, tenant, or spouse who is required to file Form 1042, Annual Withholding Tax Return for U.S. Source Income of Foreign Persons Complete lines 1, 2, 3 (if applicable), 4a–5b, 7a–b (if applicable), 8a, 8b–c (if applicable), 9a, 9b (if applicable), 10, and 18. Is an agent, broker, fiduciary, manager, tenant, or spouse who is required to file Form 1042, Annual Withholding Tax Return for U.S. Source Income of Foreign Persons Complete lines 1, 2, 3 (if applicable), 4a–5b, 7a–b (if applicable), 8a, 8b–c (if applicable), 9a, 9b (if applicable), 10, and 18. Serves as a tax reporting agent for public assistance recipients under Rev. Proc. 80-4, 1980-1 C.B. 581 7 Complete lines 1, 2, 4a–5b, 9a, 10, and 18. Is a withholding agent for taxes on non-wage income paid to an alien (i.e., individual, corporation, or partnership, etc.) Is a state or local agency Serves as a tax reporting agent for public assistance recipients under Rev. Proc. 80-4, 1980-1 C.B. 581 7 Complete lines 1, 2, 4a–5b, 9a, 10, and 18. Is a single-member LLC Needs an EIN to file Form 8832, Classification Election, for filing employment tax returns and excise tax returns, or for state reporting purposes 8 Complete lines 1–18 (as applicable). Is a single-member LLC Needs an EIN to file Form 8832, Classification Election, for filing employment tax returns and excise tax returns, or for state reporting purposes 8 Complete lines 1–18 (as applicable). Is an S corporation Needs an EIN to file Form 2553, Election by a Small Business Corporation 9 Complete lines 1–18 (as applicable). Is an S corporation Needs an EIN to file Form 2553, Election by a Small Business Corporation 9 Complete lines 1–18 (as applicable). Does not currently have (nor expect to have) employees Does not currently have (nor expect to have) employees THEN... Complete lines 1, 2, 4a–8a, 8b–c (if applicable), 9a, 9b (if applicable), and 10–14 and 16–18. 1 For example, a sole proprietorship or self-employed farmer who establishes a qualified retirement plan, or is required to file excise, employment, alcohol, tobacco, or firearms returns, must have an EIN. A partnership, corporation, REMIC (real estate mortgage investment conduit), nonprofit organization (church, club, etc.), or farmers’ cooperative must use an EIN for any tax-related purpose even if the entity does not have employees. 1 For example, a sole proprietorship or self-employed farmer who establishes a qualified retirement plan, or is required to file excise, employment, alcohol, tobacco, or firearms returns, must have an EIN. A partnership, corporation, REMIC (real estate mortgage investment conduit), nonprofit organization (church, club, etc.), or farmers’ cooperative must use an EIN for any tax-related purpose even if the entity does not have employees. 2 However, do not apply for a new EIN if the existing entity only (a) changed its business name, (b) elected on Form 8832 to change the way it is taxed (or is covered by the default rules), or (c) terminated its partnership status because at least 50% of the total interests in partnership capital and profits were sold or exchanged within a 12-month period. The EIN of the terminated partnership should continue to be used. See Regulations section 301.6109-1(d)(2)(iii). Do not use the EIN of the prior business unless you became the “owner” of a corporation by acquiring its stock. 2 However, do not apply for a new EIN if the existing entity only (a) changed its business name, (b) elected on Form 8832 to change the way it is taxed (or is covered by the default rules), or (c) terminated its partnership status because at least 50% of the total interests in partnership capital and profits were sold or exchanged within a 12-month period. The EIN of the terminated partnership should continue to be used. See Regulations section 301.6109-1(d)(2)(iii). Do not use the EIN of the prior business unless you became the “owner” of a corporation by acquiring its stock. 4 However, grantor trusts that do not file using Optional Method 1 and IRA trusts that are required to file Form 990-T, Exempt Organization Business Income Tax Return, must have an EIN. For more information on grantor trusts, see the Instructions for Form 1041. 4 However, grantor trusts that do not file using Optional Method 1 and IRA trusts that are required to file Form 990-T, Exempt Organization Business Income Tax Return, must have an EIN. For more information on grantor trusts, see the Instructions for Form 1041. 5 A plan administrator is the person or group of persons specified as the administrator by the instrument under which the plan is operated. 5 A plan administrator is the person or group of persons specified as the administrator by the instrument under which the plan is operated. 6 Entities applying to be a Qualified Intermediary (QI) need a QI-EIN even if they already have an EIN. See Rev. Proc. 2000-12. 6 Entities applying to be a Qualified Intermediary (QI) need a QI-EIN even if they already have an EIN. See Rev. Proc. 2000-12. 7 See also Household employer on page 4 of the instructions. Note. State or local agencies may need an EIN for other reasons, for example, hired employees. 7 See also Household employer on page 4 of the instructions. Note. State or local agencies may need an EIN for other reasons, for example, hired employees. 8 See Disregarded entities on page 4 of the instructions for details on completing Form SS-4 for an LLC. 8 See Disregarded entities on page 4 of the instructions for details on completing Form SS-4 for an LLC. 9 An existing corporation that is electing or revoking S corporation status should use its previously-assigned EIN. 9 An existing corporation that is electing or revoking S corporation status should use its previously-assigned EIN. 3 3 2 Form 2678 (Rev. June 2011) Employer/Payer Appointment of Agent OMB No. 1545-0748 Department of the Treasury — Internal Revenue Service Use this form if you want to request approval to have an agent file returns and make deposits or payments of employment or other withholding taxes or if you want to revoke an existing appointment. Form 2678 (Rev. June 2011) Employer/Payer Appointment of Agent OMB No. 1545-0748 Department of the Treasury — Internal Revenue Service Use this form if you want to request approval to have an agent file returns and make deposits or payments of employment or other withholding taxes or if you want to revoke an existing appointment. For IRS use: • If you are an employer or payer who wants to request approval, complete Parts 1 and 2 and sign Part 2. Then give it to the agent. Have the agent complete Part 3 and sign it. • If you are an employer or payer who wants to request approval, complete Parts 1 and 2 and sign Part 2. Then give it to the agent. Have the agent complete Part 3 and sign it. Note. This appointment is not effective until we approve your request. See the instructions for filing Form 2678 on page 3. Note. This appointment is not effective until we approve your request. See the instructions for filing Form 2678 on page 3. • If you are an employer, payer, or agent who wants to revoke an existing appointment, complete all three parts. In this case, only one signature is required. • If you are an employer, payer, or agent who wants to revoke an existing appointment, complete all three parts. In this case, only one signature is required. Part 1: Why you are filing this form... (Check one) ✔ You want to appoint an agent for tax reporting, depositing, and paying. You want to revoke an existing appointment. Part 1: Why you are filing this form... (Check one) ✔ You want to appoint an agent for tax reporting, depositing, and paying. You want to revoke an existing appointment. For IRS use: Part 2: Employer or Payer Information: Complete this part if you want to appoint an agent or revoke an appointment. Part 2: Employer or Payer Information: Complete this part if you want to appoint an agent or revoke an appointment. 1 Employer identification number (EIN) 1 Employer identification number (EIN) — 2 Employer’s or payer’s name (not your trade name) 2 Employer’s or payer’s name (not your trade name) 3 Trade name (if any) 3 Trade name (if any) 4 Address — 4 Address Number Street Suite or room number City ZIP code State 5 Forms for which you want to appoint an agent or revoke the agent’s appointment to file. (Check all that apply.) For ALL employees/ payees For SOME employees/ payees ✔ Form 940, 940-PR (Employer's Annual Federal Unemployment (FUTA) Tax Return)* Form 941, 941-PR, 941-SS (Employer’s QUARTERLY Federal Tax Return) Form 943, 943-PR (Employer’s Annual Federal Tax Return for Agricultural Employees) Form 944, 944-PR, 944-SS, 944(SP) (Employer’s ANNUAL Federal Tax Return) Form 945 (Annual Return of Withheld Federal Income Tax) Form CT-1 (Employer’s Annual Railroad Retirement Tax Return) Form CT-2 (Employee Representative's Quarterly Railroad Tax Return) Number Street Suite or room number City 5 Forms for which you want to appoint an agent or revoke the agent’s appointment to file. (Check all that apply.) For ALL employees/ payees For SOME employees/ payees ✔ Form 940, 940-PR (Employer's Annual Federal Unemployment (FUTA) Tax Return)* Form 941, 941-PR, 941-SS (Employer’s QUARTERLY Federal Tax Return) Form 943, 943-PR (Employer’s Annual Federal Tax Return for Agricultural Employees) Form 944, 944-PR, 944-SS, 944(SP) (Employer’s ANNUAL Federal Tax Return) Form 945 (Annual Return of Withheld Federal Income Tax) Form CT-1 (Employer’s Annual Railroad Retirement Tax Return) Form CT-2 (Employee Representative's Quarterly Railroad Tax Return) ✔ ZIP code State ✔ *Generally you cannot appoint an agent to report, deposit, and pay taxes reported on Form 940, Employer's Annual Federal Unemployment (FUTA) Tax Return, unless you are a home care service recipient. Check here if you are a home care service recipient, and you want to appoint the agent to report, deposit, and pay FUTA taxes for you. See the instructions. *Generally you cannot appoint an agent to report, deposit, and pay taxes reported on Form 940, Employer's Annual Federal Unemployment (FUTA) Tax Return, unless you are a home care service recipient. Check here if you are a home care service recipient, and you want to appoint the agent to report, deposit, and pay FUTA taxes for you. See the instructions. I am authorizing the IRS to disclose otherwise confidential tax information to the agent relating to the authority granted under this appointment, including disclosures required to process Form 2678. The agent may contract with a third party, such as a reporting agent or certified public accountant, to prepare or file the returns covered by this appointment, or to make any required deposits and payments. Such contract may authorize the IRS to disclose confidential tax information of the employer/payer and agent to such third party. If a third party fails to file the returns or make the deposits and payments, the agent and employer/payer remain liable. I am authorizing the IRS to disclose otherwise confidential tax information to the agent relating to the authority granted under this appointment, including disclosures required to process Form 2678. The agent may contract with a third party, such as a reporting agent or certified public accountant, to prepare or file the returns covered by this appointment, or to make any required deposits and payments. Such contract may authorize the IRS to disclose confidential tax information of the employer/payer and agent to such third party. If a third party fails to file the returns or make the deposits and payments, the agent and employer/payer remain liable. Print your name here Sign your name here Date Print your title here / / HHCSR Best daytime phone Print your name here Sign your name here Date Print your title here / / Now give this form to the agent to complete. ■a For Paperwork Reduction Act Notice, see the instructions. Cat. No. 18770D Form 2678 (Rev. 6-2011) HHCSR Best daytime phone Now give this form to the agent to complete. ■a For Paperwork Reduction Act Notice, see the instructions. Cat. No. 18770D Form 2678 (Rev. 6-2011) Page 2 Form 2678 (Rev. 6-2011) Page 2 Form 2678 (Rev. 6-2011) Part 3: Agent Information: If you will be an agent for an employer or payer, or want to revoke an appointment, complete this part. Part 3: Agent Information: If you will be an agent for an employer or payer, or want to revoke an appointment, complete this part. 6 Agent’s employer identification number (EIN) 6 Agent’s employer identification number (EIN) 7 Agent’s name (not trade name) Seren Derin 7 Agent’s name (not trade name) Seren Derin 8 Trade name (if any) Stavros Ctr for Ind Liv Inc. 8 Trade name (if any) Stavros Ctr for Ind Liv Inc. 9 Address 9 Address 0 4 — 3 7 6 5 5 4 1 210 Old Farm Road Number Street Amherst City State Date / / Print your name here Seren Derin Print your title here Fiscal Director Best daytime phone Form 2678 (Rev. 6-2011) 3 7 6 5 Street 5 4 1 Suite or room number MA City State 01002 ZIP code Check here if the employer is a home care service recipient receiving home care services through a program administered by a federal, state, or local government agency. Under penalties of perjury, I declare that I have examined this form and any attachments, and to the best of my knowledge and belief, it is true, correct, and complete. 413-256-6692 — Amherst ZIP code Under penalties of perjury, I declare that I have examined this form and any attachments, and to the best of my knowledge and belief, it is true, correct, and complete. Sign your name here Number 01002 Check here if the employer is a home care service recipient receiving home care services through a program administered by a federal, state, or local government agency. 4 210 Old Farm Road Suite or room number MA 0 Sign your name here Date / / Print your name here Seren Derin Print your title here Fiscal Director Best daytime phone 413-256-6692 Form 2678 (Rev. 6-2011) Form 2678 (Rev. 6-2011) Instructions for Form 2678 Section references are to the Internal Revenue Code. Use this form if you want to request approval to have an agent file returns and make deposits or payments of employment or other withholding taxes or if you want to revoke an existing appointment. You cannot use a prior version of this form. All prior versions are obsolete and will not be accepted. • If you want to appoint an agent, check the box in Part 1 that says, “You want to appoint an agent for tax reporting, depositing, and paying,” and complete Part 2. Note. Generally you cannot appoint an agent to file an aggregate Form 940. Beginning with the 2010 tax year, if you are a home care service recipient you may request approval for an agent to report, file, and pay taxes on a Form 940, by checking the box in the footnote on line 5. At the time this form went to print, proposed regulations REG-137036-08 were issued to modify Regulations section 31.3504-1 to allow home care service recipients to appoint an agent to report, file, and pay taxes on Form 940. • If you are an agent and you want to accept an appointment, complete Part 3. If you are a corporate officer, partner, or tax matters partner, you must have the authority to execute this appointment of agent. Note. If the employer/payer will be making payments not covered by the appointment, the employer/payer must file all related returns and deposit and pay taxes for those payments. When completing line 5, check the box(es) “For SOME employees/payees.” • If you are an employer, payer, or agent and you want to revoke an existing appointment of an agent, check the box in Part 1 that says, “You want to revoke an existing appointment,” and complete Parts 2 and 3. However, only one signature is required. If an existing appointment is revoked, the IRS cannot disclose confidential tax information to anyone other than the employer/payer for periods after the appointment is revoked. Filing Form 2678 Send Form 2678 to the address for your location in the Where To File Chart later. We will send a letter to the agent after we have approved the request. Until we approve the request, the agent is not liable for filing any tax returns or making any deposits or payments. Filing Schedule R (Form 940) and Schedule R (Form 941) An agent for a home care service recipient that files an aggregate Form 940 must complete Schedule R (Form 940), Allocation Schedule for Aggregate Form 940 Filers, and file it with the aggregate Form 940. An agent that files an aggregate Form 941 must complete Schedule R (Form 941), Allocation Schedule for Aggregate Form 941 Filers, and file it with the aggregate Form 941. Page 3 Form 2678 (Rev. 6-2011) What are the reporting, deposit, and payment requirements after the IRS approves the appointment? Instructions for Form 2678 Agents must follow the procedures in Revenue Procedure 70-6 for employment taxes (unless you are a subagent for a state agent under Notice 2003-70) and Revenue Procedure 84-33 for backup withholding. Agents for employers who are home care service recipients receiving home care services through a program administered by a federal, state, or local government agency may also use this form. These agents are often referred to as “fiscal/employer agents” and “household employer agents.” All agents, employers, and payers remain liable for filing all returns and making all tax deposits and payments while this appointment is in effect. If an agent contracts with a third party, such as a reporting agent or certified public accountant, to prepare or file the returns covered by this appointment or to make any required tax deposits or payments and the third party fails to do so, the agent, employer, and payer remain liable. Use this form if you want to request approval to have an agent file returns and make deposits or payments of employment or other withholding taxes or if you want to revoke an existing appointment. You cannot use a prior version of this form. All prior versions are obsolete and will not be accepted. Privacy Act and Paperwork Reduction Act Notice. We ask for the information on Form 2678 to carry out the Internal Revenue laws of the United States. The principal purpose of this information is to permit you to appoint an agent to act on your behalf. You do not have to appoint an agent; however, if you choose to appoint an agent, you must provide the information requested on Form 2678. Our authority to collect this information is section 3504. Section 6109 requires you and the agent to provide your identification numbers. Failure to provide this information could delay or prevent processing your appointment of agent. Intentionally providing false information could subject you and the agent to penalties. You are not required to provide the information requested on a form that is subject to the Paperwork Reduction Act unless the form displays a valid OMB control number. Books or records relating to a form or its instructions must be retained as long as their contents may become material in the administration of any Internal Revenue law. Generally, tax returns and return information are confidential, as required by section 6103. However, section 6103 allows or requires the IRS to disclose or give the information shown on this form to others as described in the Code. For example, we may disclose your tax information to the Department of Justice for civil and criminal litigation, and to cities, states, the District of Columbia, and U.S. commonwealths and possessions for use in administering their tax laws. We may also disclose this information to other countries under a tax treaty, to federal and state agencies to enforce federal nontax criminal laws, or to federal law enforcement and intelligence agencies to combat terrorism. The time needed to complete and file Form 2678 will vary depending on individual circumstances. The estimated average time is 2 hrs., 12 minutes. If you have comments concerning the accuracy of this time estimate or suggestions for making Form 2678 simpler, we would be happy to hear from you. You can send comments by email to *taxforms@irs.gov. Enter “Form 2678” on the subject line. Or write to: Internal Revenue Service, Tax Products Coordinating Committee, SE:W:CAR:MP:T:T:SP, 1111 Constitution Ave., NW, IR-6526, Washington, DC 20224. Do not send Form 2678 to this address. Instead, see the Where To File Chart later. Section references are to the Internal Revenue Code. • If you want to appoint an agent, check the box in Part 1 that says, “You want to appoint an agent for tax reporting, depositing, and paying,” and complete Part 2. Note. Generally you cannot appoint an agent to file an aggregate Form 940. Beginning with the 2010 tax year, if you are a home care service recipient you may request approval for an agent to report, file, and pay taxes on a Form 940, by checking the box in the footnote on line 5. At the time this form went to print, proposed regulations REG-137036-08 were issued to modify Regulations section 31.3504-1 to allow home care service recipients to appoint an agent to report, file, and pay taxes on Form 940. • If you are an agent and you want to accept an appointment, complete Part 3. If you are a corporate officer, partner, or tax matters partner, you must have the authority to execute this appointment of agent. Note. If the employer/payer will be making payments not covered by the appointment, the employer/payer must file all related returns and deposit and pay taxes for those payments. When completing line 5, check the box(es) “For SOME employees/payees.” • If you are an employer, payer, or agent and you want to revoke an existing appointment of an agent, check the box in Part 1 that says, “You want to revoke an existing appointment,” and complete Parts 2 and 3. However, only one signature is required. If an existing appointment is revoked, the IRS cannot disclose confidential tax information to anyone other than the employer/payer for periods after the appointment is revoked. Filing Form 2678 Send Form 2678 to the address for your location in the Where To File Chart later. We will send a letter to the agent after we have approved the request. Until we approve the request, the agent is not liable for filing any tax returns or making any deposits or payments. Filing Schedule R (Form 940) and Schedule R (Form 941) An agent for a home care service recipient that files an aggregate Form 940 must complete Schedule R (Form 940), Allocation Schedule for Aggregate Form 940 Filers, and file it with the aggregate Form 940. An agent that files an aggregate Form 941 must complete Schedule R (Form 941), Allocation Schedule for Aggregate Form 941 Filers, and file it with the aggregate Form 941. Page 3 What are the reporting, deposit, and payment requirements after the IRS approves the appointment? Agents must follow the procedures in Revenue Procedure 70-6 for employment taxes (unless you are a subagent for a state agent under Notice 2003-70) and Revenue Procedure 84-33 for backup withholding. Agents for employers who are home care service recipients receiving home care services through a program administered by a federal, state, or local government agency may also use this form. These agents are often referred to as “fiscal/employer agents” and “household employer agents.” All agents, employers, and payers remain liable for filing all returns and making all tax deposits and payments while this appointment is in effect. If an agent contracts with a third party, such as a reporting agent or certified public accountant, to prepare or file the returns covered by this appointment or to make any required tax deposits or payments and the third party fails to do so, the agent, employer, and payer remain liable. Privacy Act and Paperwork Reduction Act Notice. We ask for the information on Form 2678 to carry out the Internal Revenue laws of the United States. The principal purpose of this information is to permit you to appoint an agent to act on your behalf. You do not have to appoint an agent; however, if you choose to appoint an agent, you must provide the information requested on Form 2678. Our authority to collect this information is section 3504. Section 6109 requires you and the agent to provide your identification numbers. Failure to provide this information could delay or prevent processing your appointment of agent. Intentionally providing false information could subject you and the agent to penalties. You are not required to provide the information requested on a form that is subject to the Paperwork Reduction Act unless the form displays a valid OMB control number. Books or records relating to a form or its instructions must be retained as long as their contents may become material in the administration of any Internal Revenue law. Generally, tax returns and return information are confidential, as required by section 6103. However, section 6103 allows or requires the IRS to disclose or give the information shown on this form to others as described in the Code. For example, we may disclose your tax information to the Department of Justice for civil and criminal litigation, and to cities, states, the District of Columbia, and U.S. commonwealths and possessions for use in administering their tax laws. We may also disclose this information to other countries under a tax treaty, to federal and state agencies to enforce federal nontax criminal laws, or to federal law enforcement and intelligence agencies to combat terrorism. The time needed to complete and file Form 2678 will vary depending on individual circumstances. The estimated average time is 2 hrs., 12 minutes. If you have comments concerning the accuracy of this time estimate or suggestions for making Form 2678 simpler, we would be happy to hear from you. You can send comments by email to *taxforms@irs.gov. Enter “Form 2678” on the subject line. Or write to: Internal Revenue Service, Tax Products Coordinating Committee, SE:W:CAR:MP:T:T:SP, 1111 Constitution Ave., NW, IR-6526, Washington, DC 20224. Do not send Form 2678 to this address. Instead, see the Where To File Chart later. Form 2678 (Rev. 6-2011) Page Where To File Chart 4 Form 2678 (Rev. 6-2011) Page Then use this address ... Department of the Treasury, Internal Revenue Service, Cincinnati, OH 45999 Where To File Chart If you are in ... Connecticut Delaware District of Columbia Illinois Indiana Kentucky Maine Maryland Massachusetts Michigan New Hampshire New Jersey New York North Carolina Ohio Pennsylvania Rhode Island South Carolina Vermont Virginia West Virginia Wisconsin Department of the Treasury, Internal Revenue Service, Ogden, UT 84201 Alabama Alaska Arizona Arkansas California Colorado Florida Georgia Hawaii Idaho Iowa Kansas Louisiana Minnesota Mississippi Missouri Montana Nebraska Nevada New Mexico North Dakota Oklahoma Oregon South Dakota Tennessee Texas Utah Washington Wyoming No legal residence or place of business in any state Department of the Treasury, Internal Revenue Service, Ogden, UT 84201 No legal residence or place of business in any state Department of the Treasury, Internal Revenue Service, Ogden, UT 84201 Exempt organization or government entity Department of the Treasury, Internal Revenue Service, Ogden, UT 84201-0046 Exempt organization or government entity Department of the Treasury, Internal Revenue Service, Ogden, UT 84201-0046 If you are in ... Connecticut Delaware District of Columbia Illinois Indiana Kentucky Maine Maryland Massachusetts Michigan New Hampshire New Jersey New York North Carolina Ohio Pennsylvania Rhode Island South Carolina Vermont Virginia West Virginia Wisconsin Alabama Alaska Arizona Arkansas California Colorado Florida Georgia Hawaii Idaho Iowa Kansas Louisiana Minnesota Mississippi Missouri Montana Nebraska Nevada New Mexico North Dakota Oklahoma Oregon South Dakota Tennessee Texas Utah Washington Wyoming Then use this address ... Department of the Treasury, Internal Revenue Service, Cincinnati, OH 45999 Department of the Treasury, Internal Revenue Service, Ogden, UT 84201 4 Rev. 12/00 Form M-2848 Power of Attorney and Declaration of Representative Rev. 12/00 Form M-2848 Power of Attorney and Declaration of Representative Massachusetts Department of Revenue See separate instructions. Please print or type. Massachusetts Department of Revenue See separate instructions. Please print or type. Part 1 . Power of Attorney Part 1 . Power of Attorney A Name of taxpayer(s) A Name of taxpayer(s) Social Security number(s) Social Security number(s) Number and street, including apartment number or rural route Federal Identification number Number and street, including apartment number or rural route Federal Identification number City/Town State City/Town State Zip B Hereby appoint(s) the following individual(s) as attorney(s)-in-fact to represent the taxpayer(s) before any office of the Massachusetts Department of Revenue for the following tax rnatter(s) (specify the type(s) of tax and year(s) or period(s) (date of death if estate tax))· Name SEREN DERIN Type of tax (individual , corporate, etc.) B Hereby appoint(s) the following individual(s) as attorney(s)-in-fact to represent the taxpayer(s) before any office of the Massachusetts Department of Revenue for the following tax rnatter(s) (specify the type(s) of tax and year(s) or period(s) (date of death if estate tax))· Telephone number Address STAVROS C. I. L. P.O. BOX 2130, AMHERST MA 01004 (413)256-6692 Name ALL Telephone number Address STAVROS C. I. L. P.O. BOX 2130, AMHERST MA 01004 SEREN DERIN Year(s) or period(s) (date ol death if estate tax) INCOME TAX WITHHOLDING, TA-l Zip Type of tax (individual , corporate, etc.) (413)256-6692 Year(s) or period(s) (date ol death if estate tax) INCOME TAX WITHHOLDING, TA-l ALL C The attorney(s)-in-fact (or any of them) are authorized, subject to any limitations set forth below or to revocation, to receive confidential information and to C The attorney(s)-in-fact (or any of them) are authorized, subject to any limitations set forth below or to revocation, to receive confidential information and to perform any and all acts that the principal(s) can perform with respect to the above specified tax matters, such as the authority to sign any agreements, consents or other documents.The authority does not include the power to substitute another representative (unless specifically added below) or the power to receive refund checks. perform any and all acts that the principal(s) can perform with respect to the above specified tax matters, such as the authority to sign any agreements, consents or other documents.The authority does not include the power to substitute another representative (unless specifically added below) or the power to receive refund checks. List any specific additions or deletions to the acts otherwise authorized in this power of attorney: List any specific additions or deletions to the acts otherwise authorized in this power of attorney: D Originals of notices and other written communications go to the taxpayer(s). Send copies of all notices and all other written communications addressed to the taxpayer(s) in proceedings involving the above tax matters to: to the taxpayer(s) in proceedings involving the above tax matters to: 1 []! the appointee first named above, or 2 0 D Originals of notices and other written communications go to the taxpayer(s). Send copies of all notices and all other written communications addressed 1 []! the appointee first named above, or 2 (name of another appointee designated above) 0 (name of another appointee designated above) This power of attorney revokes all earlier powers of attorney on file with the Department of Revenue for the same tax matters and years or periods covered by this power of attorney, except the following (specify to whom granted, date and address including Zip code or attach copies of earlier powers) : This power of attorney revokes all earlier powers of attorney on file with the Department of Revenue for the same tax matters and years or periods covered by this power of attorney, except the following (specify to whom granted, date and address including Zip code or attach copies of earlier powers) : E Signature of or for taxpayer(s). If signed by a corporate officer, partner, or fiduciary on behalf of the taxpayer, I certify that I have the authority to execute this power of attorney on behalf of the taxpayer. E Signature of or for taxpayer(s). If signed by a corporate officer, partner, or fiduciary on behalf of the taxpayer, I certify that I have the authority to execute this power of attorney on behalf of the taxpayer. Signature Title (if applicable) Date Signature EMPLOYER Title (if applicable) Date EMPLOYER If signing for a taxpayer who is not an individual, type or print your name Signature Title (if applicable) If signing for a taxpayer who is not an individual, type or print your name Date Signature Title (if applicable) Date - ----- -- - - - -- - - - - - - - - - - - -- - -- - -- - - -- -- F If the power of attorney is granted to a person other than an attorney, certified public accountant, public accountant or enrolled agent, the taxpayer(s) signature must be witnessed or notarized below. The person(s) signing as or for the taxpayer(s) (check and complete one): D - ---, - ----- -- - - - -- - - - - - - - - - - - -- D is/are known to and signed in the presence of the two disinterested witnesses whose signatures appear here: Date Signature of witness Date Signature of witness Date Signature of witness Date D appeared this day before a notary public and acknowledged this power of attorney as a voluntary act and deed. Signature of notary appeared this day before a notary public and acknowledged this power of attorney as a voluntary act and deed. Signature of notary Date Date Part 2. Declaration of Representative. All representatives must complete this section. I declare that I am not currently under suspension or disbarment from practice within the Commonwealth or in any jurisdiction, that I am aware of regulations governing the practice of attorneys, certified public accountants, public accountants, enrolled agents and others, and that I am one of the following: All representatives must complete this section. I declare that I am not currently under suspension or disbarment from practice within the Commonwealth or in any jurisdiction, that I am aware of regulations governing the practice of attorneys, certified public accountants, public accountants, enrolled agents and others, and that I am one of the following: 1 a member in good standing of the bar of the highest court of the jurisdiction shown below; 1 a member in good standing of the bar of the highest court of the jurisdiction shown below; 2 duly qualified to practice as a certified public accountant or public accountant in the jurisdiction shown below; 2 duly qualified to practice as a certified public accountant or public accountant in the jurisdiction shown below; 3 enrolled as an agent under the requirements of Treasury Department Circular No. 230; 3 enrolled as an agent under the requirements of Treasury Department Circular No. 230; 4 a bona fide officer of the taxpayer organization; 4 a bona fide officer of the taxpayer organization; 5 a full-time employee of the taxpayer; 5 a full-time employee of the taxpayer; 6 a member of the taxpayer's immediate family (spouse, parent, child or sibling); 6 a member of the taxpayer's immediate family (spouse, parent, child or sibling); 7 a fiduciary for the taxpayer; 7 a fiduciary for the taxpayer; 8 other (attach statement) 8 other (attach statement) and that I am authorized to represent the taxpayer identified in Part 1 for the tax matters specified there. and that I am authorized to represent the taxpayer identified in Part 1 for the tax matters specified there. Designation (insert appropriate number from above list) 2.5M 6/01 CRP0101 Jurisdiction (state, etc.) or enrollment card number - - -- -- The person(s) signing as or for the taxpayer(s) (check and complete one): is/are known to and signed in the presence of the two disinterested witnesses whose signatures appear here: Part 2. Declaration of Representative. - -- F If the power of attorney is granted to a person other than an attorney, certified public accountant, public accountant or enrolled agent, the taxpayer(s) signature must be witnessed or notarized below. Signature of witness D - -- Signature 1 Date G) printed on recycled paper Designation (insert appropriate number from above list) 2.5M 6/01 CRP0101 Jurisdiction (state, etc.) or enrollment card number Signature 1 Date G) printed on recycled paper - ---, - ' ··-- -- ---- - - - - · -·· -- - - - - -- - - - ' ··-- -- ---- - - - - Form M-2848 Instructions General Information To protect the confidentiality of tax records, Massachusetts law generally prohibits the Department of Revenue from disclosing information contained in tax returns or other documents filed with it to persons other than the taxpayer or the taxpayer's representative. For your protection, the Department requires that you file a power of attorney before it will release tax information to your representative. The power of attorney will also allow your representative to act on your behalf to the extent you indicate. Use Form M-2848, Power of Attorney and Declaration of Representative, for this purpose if you choose. You may file a power of attorney without using Form M-2848, but it must contain the same information as Form M-2848 would. You may use Form M-2848 to appoint one or more individuals to represent you in tax matters before the Department of Revenue. You may use Form M-2848 for any matters affecting any tax imposed by the Commonwealth, and the power granted is limited to these tax matters. Filing the Power of Attorney. You must file the original, a photocopy or facsimile transmission (fax) of the power of attorney with each DOR office in which your representative is to represent you. You do not have to file another copy with other DOR officers or counsel who later have the matter under consideration unless you are specifically asked to provide an additional copy. Revoking a Power of Attorney. If you previously filed a power of attorney and you want to revoke it, you may use Form M-2848 to change your representatives or alter the powers granted to them. File the form with the office of DOR in which you filed the earlier power. The new power of attorney will revoke the earlier one for the same matters and tax periods unless you specifically state otherwise. If you want to revoke a power of attorney without executing a new one, send a signed statement to each office of DOR in which you filed the earlier power of attorney you are now revoking . List in this statement the name and address of each representative whose authority is being revoked . How to Complete Form M-2848 Part 1. Power of Attorney A. Taxpayer's name, identification number and address. For individuals: Enter your name, Social Security number and address in the space provided. If a joint return is involved, and you and your spouse are designating the same representative(s), also enter your spouse's name and Social Security number, and your spouse's address (if different). For a corporation, partnership or association: Enter the name, federal identification number and business address. If the power of attorney for a partnership will be used in a tax matter in which the name and Social Security number of each partner have not previously been sent to DOR, list the name and Social Security number of each partner in the available space at the end of the form or on an attached sheet. For a trust: Enter the name, title and address of the fiduciary, and the name and federal identification number of the trust. For an estate: Enter the name, title and address of the decedent's personal representative , and the name and identification number of the estate. The identification number for an estate is the decedent's Social Security number and includes the federal identification number if the estate has one. B. Appointee. Enter the name(s), address(es) and telephone number(s) of the individual(s) you appoint. Your representative must be an individual and may not be an organization, firm or partnership. Tax matters and years or periods. Consider each tax imposed by the Commonwealth for each tax period as a separate tax matter. In the columns provided, clearly identify the type(s) of tax(es) and the year(s) or period(s) for which the power is granted. You may list any number of years or periods and types of taxes on the same power of attorney. If the matter relates to estate tax, enter the date of the taxpayer's death instead of the year or period. If the power of attorney will be used in connection with a penalty that is not related to a particular tax type, such as personal income or corporate , enter the section of the General Laws which authorizes the penalty in the ''type of tax" column. C. Powers granted by Form M-2848. Your signature on Form M-2848 authorizes the individual(s) you designate (your representative or "attorneyin-facf') generally to perform any act you can perform. This includes executing waivers and offers of waivers of restrictions on assessment or collection of deficiences in taxes, and waivers of notice of disallowance of a claim for credit or refund . It also includes executing consents extending the legally allowed period for assessment or collection of taxes. The authority does not include the power to substitute another representative (unless specifically added to Form M-2848) or the power to receive refund checks. If you do not want your representative to be able to perform any of these or other specific acts, or if you want to give your representative the power to delegate authority or substitute another representative , insert language excluding or adding these acts in the blank space provided. D. Where you want copies to be sent. The Department of Revenue routinely sends originals of all notices to the taxpayer. You may also have copies of all notices and all other written communications sent to your representative. Please check box 1 if you want copies of all notices or all communications sent to the first appointee named at the top of the form . Check box 2 if you want copies sent to one of your other appointees. In this case, list the name of the appointee. E. Signature of taxpayer(s). For individuals: If a joint return is involved and both husband and wife will be represented by the same individual(s), both must sign the power of attorney unless one authorizes the other (in writing) to sign for both. In that case, attach a copy of the authorization. However, if the spouses are to be represented by different individuals, each may execute a power of attorney. For a partnership: All partners must sign unless one partner is authorized to act in the name of the partnership. A partner is authorized to act in the name of the partnership if under state law the partner has authority to bind the partnership. For a corporation or association: An officer having authority to bind the entity must sign . If you are signing the power of attorney for a taxpayer who is not an individual, such as a corporation or trust, please type or print your name on the line below the signature line at the bottom of the form. F. Notarizing or witnessing the power of attorney. A notary public or two individuals with no stake in the tax matter must witness a power of attorney unless it is granted to an attorney, certified public accountant, public accountant or enrolled agent. Part 2. Declaration of Representative Your representative must complete Part 2 to make a declaration containing the following : 1. A statement that the representative is authorized to represent you as a certified public accountant, public accountant, attorney, enrolled agent, member of your immediate family, etc. If entering "eighf' in the "designation" column, attach a statement indicating your relationship to the taxpayer. 2. The jurisdiction recognizing the representative , if applicable. For an attorney, certified public accountant or public accountant: Enter in the "jurisdiction" column the name of the state, possession, territory, commonwealth or District of Columbia that has granted the declared professional recognition. For an enrolled agent: Enter the enrollment card number in the "jurisdiction" column. 3. The signature of the representative and the date signed. · -·· -- - - - - -- - - Form M-2848 Instructions General Information To protect the confidentiality of tax records, Massachusetts law generally prohibits the Department of Revenue from disclosing information contained in tax returns or other documents filed with it to persons other than the taxpayer or the taxpayer's representative. For your protection, the Department requires that you file a power of attorney before it will release tax information to your representative. The power of attorney will also allow your representative to act on your behalf to the extent you indicate. Use Form M-2848, Power of Attorney and Declaration of Representative, for this purpose if you choose. You may file a power of attorney without using Form M-2848, but it must contain the same information as Form M-2848 would. You may use Form M-2848 to appoint one or more individuals to represent you in tax matters before the Department of Revenue. You may use Form M-2848 for any matters affecting any tax imposed by the Commonwealth, and the power granted is limited to these tax matters. Filing the Power of Attorney. You must file the original, a photocopy or facsimile transmission (fax) of the power of attorney with each DOR office in which your representative is to represent you. You do not have to file another copy with other DOR officers or counsel who later have the matter under consideration unless you are specifically asked to provide an additional copy. Revoking a Power of Attorney. If you previously filed a power of attorney and you want to revoke it, you may use Form M-2848 to change your representatives or alter the powers granted to them. File the form with the office of DOR in which you filed the earlier power. The new power of attorney will revoke the earlier one for the same matters and tax periods unless you specifically state otherwise. If you want to revoke a power of attorney without executing a new one, send a signed statement to each office of DOR in which you filed the earlier power of attorney you are now revoking . List in this statement the name and address of each representative whose authority is being revoked . How to Complete Form M-2848 Part 1. Power of Attorney A. Taxpayer's name, identification number and address. For individuals: Enter your name, Social Security number and address in the space provided. If a joint return is involved, and you and your spouse are designating the same representative(s), also enter your spouse's name and Social Security number, and your spouse's address (if different). For a corporation, partnership or association: Enter the name, federal identification number and business address. If the power of attorney for a partnership will be used in a tax matter in which the name and Social Security number of each partner have not previously been sent to DOR, list the name and Social Security number of each partner in the available space at the end of the form or on an attached sheet. For a trust: Enter the name, title and address of the fiduciary, and the name and federal identification number of the trust. For an estate: Enter the name, title and address of the decedent's personal representative , and the name and identification number of the estate. The identification number for an estate is the decedent's Social Security number and includes the federal identification number if the estate has one. B. Appointee. Enter the name(s), address(es) and telephone number(s) of the individual(s) you appoint. Your representative must be an individual and may not be an organization, firm or partnership. Tax matters and years or periods. Consider each tax imposed by the Commonwealth for each tax period as a separate tax matter. In the columns provided, clearly identify the type(s) of tax(es) and the year(s) or period(s) for which the power is granted. You may list any number of years or periods and types of taxes on the same power of attorney. If the matter relates to estate tax, enter the date of the taxpayer's death instead of the year or period. If the power of attorney will be used in connection with a penalty that is not related to a particular tax type, such as personal income or corporate , enter the section of the General Laws which authorizes the penalty in the ''type of tax" column. C. Powers granted by Form M-2848. Your signature on Form M-2848 authorizes the individual(s) you designate (your representative or "attorneyin-facf') generally to perform any act you can perform. This includes executing waivers and offers of waivers of restrictions on assessment or collection of deficiences in taxes, and waivers of notice of disallowance of a claim for credit or refund . It also includes executing consents extending the legally allowed period for assessment or collection of taxes. The authority does not include the power to substitute another representative (unless specifically added to Form M-2848) or the power to receive refund checks. If you do not want your representative to be able to perform any of these or other specific acts, or if you want to give your representative the power to delegate authority or substitute another representative , insert language excluding or adding these acts in the blank space provided. D. Where you want copies to be sent. The Department of Revenue routinely sends originals of all notices to the taxpayer. You may also have copies of all notices and all other written communications sent to your representative. Please check box 1 if you want copies of all notices or all communications sent to the first appointee named at the top of the form . Check box 2 if you want copies sent to one of your other appointees. In this case, list the name of the appointee. E. Signature of taxpayer(s). For individuals: If a joint return is involved and both husband and wife will be represented by the same individual(s), both must sign the power of attorney unless one authorizes the other (in writing) to sign for both. In that case, attach a copy of the authorization. However, if the spouses are to be represented by different individuals, each may execute a power of attorney. For a partnership: All partners must sign unless one partner is authorized to act in the name of the partnership. A partner is authorized to act in the name of the partnership if under state law the partner has authority to bind the partnership. For a corporation or association: An officer having authority to bind the entity must sign . If you are signing the power of attorney for a taxpayer who is not an individual, such as a corporation or trust, please type or print your name on the line below the signature line at the bottom of the form. F. Notarizing or witnessing the power of attorney. A notary public or two individuals with no stake in the tax matter must witness a power of attorney unless it is granted to an attorney, certified public accountant, public accountant or enrolled agent. Part 2. Declaration of Representative Your representative must complete Part 2 to make a declaration containing the following : 1. A statement that the representative is authorized to represent you as a certified public accountant, public accountant, attorney, enrolled agent, member of your immediate family, etc. If entering "eighf' in the "designation" column, attach a statement indicating your relationship to the taxpayer. 2. The jurisdiction recognizing the representative , if applicable. For an attorney, certified public accountant or public accountant: Enter in the "jurisdiction" column the name of the state, possession, territory, commonwealth or District of Columbia that has granted the declared professional recognition. For an enrolled agent: Enter the enrollment card number in the "jurisdiction" column. 3. The signature of the representative and the date signed. FISCAL INTERMEDIARY PROGRAM FISCAL INTERMEDIARY PROGRAM Consent to Use Payroll Processing Agent Consent to Use Payroll Processing Agent ȱȱȱȱȱȱ¢ȱȱȱ¡ȱęȱȱȱȱ ¢ȱǻǼȱȱȱȱȱȱȱĴȱǻǼȱȱȱȱ¢ȱ processing agent, PAI Services, LLC. ȱȱȱȱȱȱ¢ȱȱȱ¡ȱęȱȱȱȱ ¢ȱǻǼȱȱȱȱȱȱȱĴȱǻǼȱȱȱȱ¢ȱ processing agent, PAI Services, LLC. ȱȱȱȱȱȱȱǰȱ¢ȱȱȱ¢ȱǰȱȱ ȱȱȱǰȱȱȱȱȱ¢ȱǯȱȱȱȱȱǰȱȱȱ ȱȱ ȱ¢ȱȱȱȱȱȱ ȱDZ ȱȱȱȱȱȱȱǰȱ¢ȱȱȱ¢ȱǰȱȱ ȱȱȱǰȱȱȱȱȱ¢ȱǯȱȱȱȱȱǰȱȱȱ ȱȱ ȱ¢ȱȱȱȱȱȱ ȱDZ • ȱȱȱ¢ȱǰȱȱȱȱȱȱȱǯ • ȱȱȱ ȱȱȱȂȱȱȱȱȱ • ȱȱȱ¢ȱǰȱȱȱȱȱȱȱǯ • ȱȱȱ ȱȱȱȂȱȱȱȱȱ • • • • • • deposit program. ȱȱȱ ȱȱȱȱȱȱȱ¡ǰȱȱ ¢ȱȱȱ¡ǯ ȱȱȱ¢ȱ¡ȱ ȱȱȱȱ¢ȱȱ ¢ȱ¡Dzȱȱ¡ȱȱȱ¡ǯ ȱȱȱȱȱ¡ǯ ȱȱȱ¢ȱ¡ȱ ȱȱ ȱȱĴȱ ȱȱȱȱ ȱȱ¡ǯ ȱȱȱ ȱȱȱȱȱşŚŗǰȱȱşŚŖȱȱȱşŚŖȱ ȱȱȬŘȱȱȬřǯ ȱȱȱ ȱȱ ȱȱĴȱȱȱŗǰȱ ȱȬŗȱȱ ȱȱ¢ȱȱǯ • • • • • • deposit program. ȱȱȱ ȱȱȱȱȱȱȱ¡ǰȱȱ ¢ȱȱȱ¡ǯ ȱȱȱ¢ȱ¡ȱ ȱȱȱȱ¢ȱȱ ¢ȱ¡Dzȱȱ¡ȱȱȱ¡ǯ ȱȱȱȱȱ¡ǯ ȱȱȱ¢ȱ¡ȱ ȱȱ ȱȱĴȱ ȱȱȱȱ ȱȱ¡ǯ ȱȱȱ ȱȱȱȱȱşŚŗǰȱȱşŚŖȱȱȱşŚŖȱ ȱȱȬŘȱȱȬřǯ ȱȱȱ ȱȱ ȱȱĴȱȱȱŗǰȱ ȱȬŗȱȱ ȱȱ¢ȱȱǯ ȱȱ ȱȱ Date Date ȱ ȱ ȱ ŘŗŖȱȱȱ ȱ ǯǯȱ¡ȱŘŗřŖȱ ȱ ǰȱȱŖŗŖŖŚ ȱ ǻŞŖŖǼȱŚŚŘȬŗŗŞśȱȦȱ ȱ ǻŚŗřǼȱŘśŜȬŜŜşŘȱȦ ȱȱȱȱ ǯęǯ ȱȱ¡ȱǛDZȱŗȬŞŞŞȬŝŝřȬŚŘŞŗȱ ŗŖȦŘŖȦŘŖŖś ȱ ŘŗŖȱȱȱ ȱ ǯǯȱ¡ȱŘŗřŖȱ ȱ ǰȱȱŖŗŖŖŚ ȱ ǻŞŖŖǼȱŚŚŘȬŗŗŞśȱȦȱ ȱ ǻŚŗřǼȱŘśŜȬŜŜşŘȱȦ ȱȱȱȱ ǯęǯ ȱȱ¡ȱǛDZȱŗȬŞŞŞȬŝŝřȬŚŘŞŗȱ ŗŖȦŘŖȦŘŖŖś


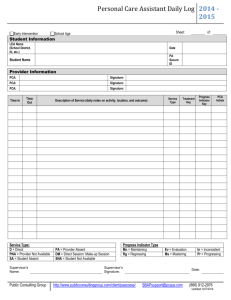
![See our handout on Classroom Access Personnel [doc]](http://s3.studylib.net/store/data/007033314_1-354ad15753436b5c05a8b4105c194a96-300x300.png)