Inguinal Lymph Nodes Management In Squamous Cell Carcinoma
advertisement

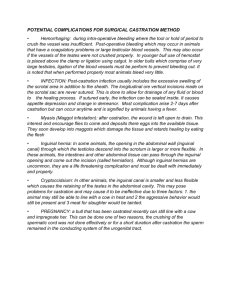
Article ID: WMC001565 2046-1690 Inguinal Lymph Nodes Management In Squamous Cell Carcinoma Of The Anal Canal Corresponding Author: Dr. Saleh M Abbas, Surgeon, Surgery - Australia Submitting Author: Dr. Saleh M Abbas, Surgeon, Surgery - Australia Article ID: WMC001565 Article Type: Review articles Submitted on:20-Feb-2011, 06:33:08 AM GMT Published on: 22-Feb-2011, 08:50:03 PM GMT Article URL: http://www.webmedcentral.com/article_view/1565 Subject Categories:GENERAL SURGERY Keywords:Carcinoma, Radiotherapy, Inguinal Nodes How to cite the article:Abbas S M. Inguinal Lymph Nodes Management In Squamous Cell Carcinoma Of The Anal Canal . WebmedCentral GENERAL SURGERY 2011;2(2):WMC001565 WebmedCentral > Review articles Page 1 of 9 WMC001565 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 07:35:37 AM Inguinal Lymph Nodes Management In Squamous Cell Carcinoma Of The Anal Canal Author(s): Abbas S M Abstract Background Current issues in the management of clinically negative inguinal lymph nodes in squamous cell carcinoma of the anal canal. Quality of the available evidence. Background The first line of management of squamous cell carcinoma (SCC) of the anal canal is chemo-radiation. The radiation field includes, in addition to the anal region and the perirectal nodes, the iliac and both inguinal triangles to target the inguinal nodes. More recently a selective approach has been investigated in patients with non-palpable inguinal nodes utilizing sentinel node biopsy and PET scan. Methods Medline was searched using the keywords, squamous cell carcinoma, anal canal, inguinal lymph nodes, sentinel node and radiotherapy. Relevant articles were reviewed with regard to the management of inguinal nodes in SCC of the anal canal. Results: Currently the management of clinically normal inguinal nodes in SCC of the anal canal is prophylactic radiation of both inguinal areas. Clinically involved nodes are included in the radiation field plus a boost of radiation to the groin that harbor involved nodes. The radiation is refined recently by intensity modulation radiotherapy (IMR) to involve the diseased area and minimize radiation exposure of normal adjacent tissues. Alternatively, more recently, a selective approach with utilization of sentinel node biopsy and radiation to microscopically involved nodal areas has been described. Conclusion: The treatment of clinically normal inguinal nodes is currently by prophylactic radiation of both inguinal regions. It is possible that in the future radiation of clinically normal inguinal may become more selective with an increasing reliance on sentinel node biopsy. Further studies are needed in this field to assess the efficacy of this approach. Although Squamous cell carcinoma (SCC) of the anal canal is an uncommon disease it is the most common malignant tumor of the anal canal accounting for 90% of malignant tumors at this site. Survival is determined essentially by two factors; the size of the tumor and lymph node spread. Patients with no clinical evidence of nodal disease have a ten-year survival of 73% compared with 53% in those with nodal disease.1 Historically the treatment of SCC of the anal canal was abdominoperineal resection; this involves wide dissection of the ischiorectal fossa with clearance of pararectal lymph nodes with en bloc excision of the posterior vaginal wall in women 2. The current management of SCC of the anal canal is chemoradiotherapy, which includes infusion of 5-flourouracil with or without mitomycin and radiation fields that include the primary tumor and the pelvic and inguinal lymph nodes.3, 4, 5, Surgery is reserved for patients who have an incomplete response, residual disease and those with later disease recurrence. The lymphatic drainage of tumors of the anal canal is bidirectional and depends on the tumor location in relation to the dentate line. Above the dentate line most of the lymph drains in a cephalad direction along the inferior rectal artery to the origin of the inferior mesenteric artery, also along the territory of the middle rectal artery to the iliac nodes. Below the dentate line it drains to the inguinal nodes along the femoral artery. Hence the lymphatic drainage is to the ipsilateral inguinal lymph nodes. The probability of nodal spread is relative to the tumor size (T stage). 1 When the primary tumor is clearly located laterally, the inguinal metastasis nearly always is homolateral to the primary tumor. Midline tumors and locally advanced lesions usually show bilateral inguinal and pararectal lymph node involvement. In the Lyon series bilateral involvement was seen only when the primary tumor involved the medial part of the anal canal. 6 Overall, inguinal nodal involvement occurs in 10-25% of patients 7, 8,9, 10. Using bipedal lymphangiography in a group of patients with anal cancer Davey et al demonstrated metastasis to external iliac lymph nodes in 7 out of 28 patients (25%).11 CT detected disease in the external iliac nodes in only one of these patients. WebmedCentral > Review articles Page 2 of 9 WMC001565 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 07:35:37 AM Lymph node involvement is related to the T stage of the tumor with nodal metastases seen in 0-10% of T1 and 2 lesions and 40- 50% of T3 and 4 disease (table 1).12, 11 At the time of diagnosis local tumor extent is T1: 8.5%; T2: 51.1%; T3: 30.4%; T4: 10%.1 Pelvic lymph node involvement correlates with increasing risk of pelvic relapse and residual disease after definitive radio-chemotherapy. Pelvic nodes are routinely targeted within the radiation field of the primary tumor and therefore their involvement or otherwise are unlikely at this stage to change the approach of treatment. However this is not the case for inguinal lymph nodes. Clinical examination and CT scan are not sensitive for detecting inguinal node metastases due to the fact that the size of the lymph node does not accurately predict the likelihood of metastatic disease and 44% of involved nodes are less than 5 mm in maximal diameter.12 Currently the treatment of clinically negative inguinal nodes is prophylactic radiation given by inclusion of both inguinal regions in the radiation field with a radiation boost if the nodes are clinically involved. More recently a selective approach has been explored utilizing staging information obtained from sentinel node biopsy and PET scan. We conducted this review to assess the current strategies for dealing with treatment of clinically negative inguinal lymph nodes. Methods The literature was searched (Medline and Embase) using the keywords, squamous cell carcinoma, anal canal, inguinal lymph nodes, sentinel node and radiotherapy. The relevant articles were reviewed with regard to the management of clinically negative inguinal nodes in SCC of the anal canal. Implications of Lymph node involvement for survival The presence of metastatic disease in the inguinal nodes reflects the local extent of the disease and is a marker for advanced disease (T3 and T4). It is also a marker for the presence of systemic disease at gross or microscopic level, which is associated with an increased likelihood of incomplete response to radio-chemotherapy, resulting in loco-regional recurrence, systemic metastases and reduced overall survival.2, 13 Inguinal lymph node metastases may occur later in a metachronous manner after curative chemo-radiotherapy in about 8% of patients,and this is also associated with reduced survival. 6 Treatment failure that manifests as local recurrence or WebmedCentral > Review articles persistent disease is still amenable to treatment, usually by inguinal node dissection, but this event is associated with reduced 5 year overall survival of 40-64%.14, 15, 6 Molecular studies have failed to show any possible association between tumor genetics and tumor behavior with regard to nodal metastasis or aggressive behavior and overall survival. Deletion of cancer suppressor genes such as the p53 and Rb genes has no effect on nodal invasion.16 In patients with clinically involved inguinal nodes treated with definitive chemo- radiotherapy there is an increased risk of loco-regional failure in the regional lymph nodes, which translates into a 5-year survival of 40% after salvage nodal dissection.17, 18 Options for treatment Chemo-radiotherapy SCC of the anus is generally considered a slowly growing disease with a low tendency for systemic dissemination. Therefore loco-regional control assumes great importance in improving disease outcome. Before the advent of curative chemo-radiation the options for inguinal node treatment depended on clinical circumstances and lymph node dissection was performed only for clinically involved nodes.2, 14, 6 The management of clinically negative nodes was either wait and watch with node dissection for regional failure that occurs in 5-25% of cases or elective node dissection at the time of original surgery for the anal canal tumor.18, 10 Currently, chemo-radiotherapy is usually employed as a definitive treatment for anal canal cancer. The radiation field involves the anal canal, perineum, pelvic lymph nodes and bilateral inguinal lymph nodes.3,5,6,14,17,18 Chemo-radiotherapy is the treatment of choice fordisease in the inguinal nodes with a cure rate of 90%4, 21. The Nigro protocol is widely used. This involves 30 Grays of radiotherapy at 2 Gy per day, five days a week for three weeks to the primary tumor and to the pelvic and inguinal lymph nodes with both inguinal areas involved in the radiation field. Chemotherapy is given in the form of 5-fluorouracil intravenous infusions (1gm /m2) on days 1-4 of the radiation therapy and repeated on days 29-32 of the treatment regimen. Mitomycin C is given in the form of an intravenous bolus (15 mg/m2) on day 1 of the cycle.3 In a modification of the Nigro protocol Gerard et al 6 reported their experience in Lyon, France for 27 patients with clinically involved nodes at the time of original presentation. Patients were treated with lymph node dissection followed by chemo-radiotherapy with 5FU 1gm /m2 for four days of continuous infusion and cisplatinum 80 mg/m2 on Day 2 after standard Page 3 of 9 WMC001565 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 07:35:37 AM hydration. The radiation treatment was initiated 3 weeks after the end of the first cycle of chemotherapy. The inguinal area was irradiated with a separate direct field using a mixed beam of telecobalt and electrons. The involved inguinal area was irradiated at a dose of 45-50 Gy over 5 weeks through the antero-posterior or postero-anterior field with an additional electron boost. This group of patients was followed up for 6 years. At the end of the treatment, local control of the inguinal area was observed in 25 of the 27 patients (86%). In long-term follow-up, two patients developed contralateral inguinal metastases that were controlled by inguinal dissection and irradiation. An incomplete response was seen in two patients who had fixed inguinal nodes. Other institutions have adopted a similar approach and have achieved similar results.9, 18 Another option is inguinal irradiation with concomitant chemotherapy using 5- Flourouracil and mitomycin or cisplatinum. Radiation of the involved nodes is given according to a protocol that involves a large antero-posterior or postero-anterior field including the inguinal node areas (45 Gy in 25 fractions over five weeks). The clinically involved inguinal fields are boosted up to 65 Gy.19-23 There is no standard recommendation for patients who present with clinically non-involved inguinal nodes. Commonly, such patients receive prophylactic bilateral radiotherapy and elective inguinal dissection is not recommended. Alternatively these patients receive no treatment for the inguinal nodes and are followed up with regular clinical evaluation for inguinal node disease development. Long term follow up studies have shown that 80- 90% of those patients will have no inguinal node disease development.1, 6, 23 However, there is approximately a 15% chance of disease recurrence particularly in patients with locally advanced disease (T3 and T4) with clinically non-involved inguinal nodes. In these patients elective irradiation of non-involved inguinal regions may minimize the risk of inguinal nodes disease development. Three recent randomized trials have compared, mitomycin-based chemotherapy with radiotherapy or radiotherapy without chemotherapy, these studies also analyzed elective node radiation versus no radiation in patients with clinically negative nodes; and concluded that prophylactic irradiation of bilateral inguinal regions in normal inguinal nodes reduced the development of lymph node disease to less than 5%.20; however that part of the study was not randomized and was only a subgroup analysis. For those who develop metachronous metastases, which usually happen within six months of initial treatment, chemo-radiotherapy is the treatment of first choice. WebmedCentral > Review articles Inguinal node dissection is reserved for those who fail to respond or relapse after initial response 8. None of the available studies had considered the inclusion of the inguinal region in the field of radiation stratified by the T stage of the disease, given the fact that the higher the T stage the more likely would be a microscopic disease in the clinically non-palpable inguinal nodes. Complications of Radiation Radiation therapy to the inguinal region with concomitant chemotherapy as part of the protocol for anal canal cancer has proven to be safe and effective in preventing local recurrence. Death is a rare event as a complication of chemoradio toxicity and has been reported to occur in approximately 2% of patients.21; but that is not related to inguinal radiation, rather a complication of the whole treatment. With the increasing use of intensity modulation radiotherapy (IMR), the radiation dose is focused on the target area to avoid normal adjacent tissues. Still systemic complications of chemotherapy are significant. However radiotherapy to the inguinal region is not without its risks. Recognized complications specific to inguinal node radiation that have been reported by various centers are femoral neck fracture, radionecrosis of the femoral head, iliac artery stenosis and inguinal fibrosis leading to lymphedema of the leg. Cicchini et al reported a single case of penile shaft necrosis following inguinal irradiation due to radiation-induced thrombosis24. These complications are rare; usually occur when therapeutic doses given rather than elective doses, but they can be serious in nature. The Role of Surgery The role of surgery is controversial. Currently lymph node dissection is usually reserved for disease recurrence in the inguinal region.13, 14. Alternatively, as noted above, some centers provide elective node dissection for patients with clinically involved nodes at the time of first presentation 6. Selective Approach Since it is desirable to avoid irradiation of lymphatic fields that are not involved in macroscopic or microscopic disease, a selective approach for the management of the inguinal nodes has been evaluated in more recent studies. A selective approach to management of inguinal lymph nodes in anal SCC depends on accurate staging. A number of methods have been utilized to achieve this. Sentinel Lymph Node Biopsy Sentinel node biopsy has been studied by Bobin et al 25 who evaluated 35 patients with clinically N0 disease using a combination of blue dye and Tc99 radiocolloid mapping and followed patients for 18 Page 4 of 9 WMC001565 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 07:35:37 AM months. None of the patients, who had a pathologically negative sentinel node, had disease recurrence. Sentinel node biopsy proved to be a sensitive and safe procedure. As noted above it has been demonstrated that midline tumors usually have bilateral lymphatic drainage. Perera et al performed the procedure on 12 patients and advocated sentinel node biopsy as a safe technique for detecting metastatic disease in the inguinal nodes in patients with anal SCC26. It also proved to be useful as a useful technique to detect micrometastatic deposits in clinically normal inguinal nodes. There are no clinical studies that managed inguinal nodes with no radiation based on the results of the sentinel node biopsy; therefore it is not possible to estimate the possibility of nodal recurrence if this form of treatment is utilized. Therefore these results suggest that sentinel lymph node biopsy may have a role in guiding a more selective approach for patients with anal cancer although plainly studies with larger numbers are required. 27, 28. The role of sentinel node biopsy role is still in its early stages and may play an important role in the future to manage clinically non-palpable inguinal nodes. PET scanning: PET scanning is an established modality that is useful in the clinical management of SCC of the head and neck and esophagus. PET scanning for anal SCC provides accurate staging of disease and may alter treatment planning by identifying inguinal node involvement not apparent on clinical examination.In one study with clinically negative nodes at presentation 66% of inguinal nodes identified by PET scan were FNA positive for metastatic disease.33 In another study FDG-PET/CT detected abnormal nodes in 20% of groins that were normal by CT, and in 23% without abnormality on physical examination. Furthermore, 17% of groins negative by both CT and physical examination showed abnormal uptake on FDG-PET/CT. PET upstaged 17% with unsuspected pelvic/inguinal nodal disease 29. Currently PET scan is effective in monitoring disease response to treatment and in detection of recurrence. An important pitfall of using PET scan is the false positive detection of inguinal nodes, typically these nodes turns out to have reactive follicular hyperplasia as confirmed on histopathology of the removed nodes. Since the uptake and retention of 18F-FDG (Flourine-18-flourodesoxy-glycose) depends on the metabolic activity of the tissue 30. This problem is especially important in assessing patients with HIV who have generalized lymphadenopathy as part of their HIV infection; such nodes are potentially positive WebmedCentral > Review articles on PET scan and mostly turn out to be reactive hyperplasia. Conclusions The current treatment options for inguinal lymph nodes in patients with SCC of the anal canal vary according to local protocols and preferences. The most widely used approach is prophylactic bilateral inguinal radiation for those with clinically negative nodes and for patients with clinically positive nodes a radiation boast of the involved nodes is added. This approach is associated with good results. Although there is some evidence to support the routine irradiation of the clinically negative inguinal lymph nodes, the issue has not been addressed in the context of the T stage of the disease and there are no randomized trials to answer the question. That should be interpreted carefully taken into consideration the complications of radiotherapy and the consequence of disease recurrence in the inguinal nodes, which would require further radiotherapy or inguinal nodes dissection. Metachronous metastases are amenable to chemo-radiotherapy with good responses in particular when this occurs within six months of the initial treatment. Surgical lymph node dissection is reserved for primary failure of chemo-radiation (residual disease) and for recurrent disease. It is possible that in the future a selective approach will be adopted more often for patients with clinically negative inguinal nodes, particularly in patients with early stage disease. This will likely depend on the wider application of sentinel node sampling and PET scanning to detect nodal disease. Such treatment is desirable, as patients with negative inguinal nodes can avoid potential complications of inguinal node radiation. More work is required to prove the efficacy of sentinel node sampling and PET scan evaluation for selection of clinically node negative patients who will benefit from radiation therapy Meanwhile prophylactic radiation of clinically negative nodes remains widely practiced to prevent inguinal nodes recurrence, which would require further radiation or surgery. References 1. Touboul E, Schlienger M, Buffat L, Lefkopoulos D, Pene F, Parc R, Tiret E, Gallot D, Malafosse M, Laugier A. Epidermoid carcinoma of the anal canal. Results of curative intent radiation therapy in a series of 270 patients. Cancer 1994; 6: 1569-79. 2. Clark J, Ptrelli N, Mittelman A. Epidermoid Page 5 of 9 WMC001565 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 07:35:37 AM carcinoma of the anal canal. Cancer 1986; 57: 400-6. 3. Nigro ND, Seydel HG, Considine B, Vatkevicius VK, Leichman L, Kinzie JJ. Combined preoperative radiation and chemotherapy for squamous cell carcinoma of the anal canal. Cancer 1983; 51: 1826-9. 4. Cummings BJ, Thomas GM, Keane TJ, Haward AR, Rider WD. Radiation therapy in the treatment of anal canal carcinoma. Dis Col Rectum 1982; 25:778-82. 5. Henderson RH, Parsons JT, Morgan L, Million RR. Elective ilioinguinal lymph node irradiation. Int Radiat Oncol Biol Phys 1984; 10: 811-9. 6. Gerard JP, Chapet O, Samiei F, Morignat E, Isaac S, Paulin C, Romestaing P, Favrel V, Mornex F, Bobin JY. Management of inguinal node metastases in patients with carcinoma of the anal canal: experience in a series of 270 patients treated in Lyon and review of the literature. Cancer 2001; 92:77-84. 7. Boman BM, Moertel CG, O'Connel J, Scott M, Weiland LH, Beart RW, et al. Carcinoma of the anal canal. A clinical and pathologic study of 188 cases. Cancer 1984;54: 114-25. 8. Fuchshuber PR, Rodriguez-Bigas M, Webert, Petrelli NJ. Anal canal and perianal epidermoid cancer. J Am Coll Surg 1997; 85: 494-505. 9. Papillon J, Montbarbon JF. Epidermoid carcinoma of the anal canal. A series of 276 cases. Dis Colon Rectum 1987; 30: 324-33. 10. Pinna Pintor M, Northover JMA, Nicholls RJ. Squamous cell carcinoma of the anus at one hospital from 1948 to 1984. Br J Surg 1989. 11. Wade DS, Herrera L, Castillo NB, Petrelli NJ. Metastases to the lymph nodes in epidermoid carcinoma of the anal canal by a clearing technique. Surg Gynecol Obstet, 1989; 169: 238-42. 12. Davey P, Saibil EA, Wong R. Bipedal lymphangiography in the management of carcinoma of the anal canal. Br J Radiol 1996; 69:632-5. 13. Goldon GT, Horsley JS. Surgical management of epidermoid carcinoma of the anus. Am J Surg Pathol 1974, 131:275-80. 14. Mullen JT, Rodriguez-Bigas MA, Chang GJ, Barcenas CH, Crane CH, Skibber JM, Feig BW. Results of surgical salvage after failed chemoradiation therapy for epidermoid carcinoma of the anal canal. Ann Surg Oncol 2007; 14: 478-83. 15. Greenall MJ, Magill GB, Quan SH, DeCosse JJ. Recurrent epidermoid cancer of the anus. Cancer 1986; 57: 1437-41 . 16. Indinnimeo M, Cicchini C, Stazi A, Giarnieri E, French D, Limiti MR, Ghini C, Vecchione A. Human papilloma virus infection and p53 nuclear overexpression in anal canal carcinoma. J Exp Clin Cancer Res 1999; 18: 47-52. 17. Valentini V, Mantello G, Luzi S, Macchia G, WebmedCentral > Review articles Manfrida S, Smaniotto D. Cancer of the anal canal and local control. Rays 1998; 23: 586-94. 18. Gerard JP, Ayzac L, Hun D, Romestaing P, Ardiet JM, Mornex F. Treatment of anal canal carcinoma with high dose radiation therapy and concomitant flourouraci- cisplatinum. Long term results in 95 patients. Radiother Oncol 1998; 46: 249-56. 19. Cummings BJ, Keane TJ, O'Sullivan B, Wong CS, Catton CN. Epidermoid anal cancer: treatment by radiation alone or by radiation and 5-fluorouracil with and without mitomycin C. Int J Radiat Oncol Biol Phys 1991; 21: 115-25. 20. Flam M, John M, Pajak TF, Petrelli N, Myerson R, Doggett S, et al. Role of Mitomycin in combination with fluorouracil and radiotherapy and of salvage chemoradiation in the definitive non surgical treatment of epidermoid carcinoma of the anal canal: results of a Phase III randomized intergroup study. J Clin Oncol 1996; 14: 2527-39. 21. Peiffert D, Seitz JF, Rougier P, François E, Cvitkovic F, Mirabel X, Nasca S, Ducreux M, Hannoun-Levi JM, Lusinchi A, Debrigode E, Conroy T, Pignon JP, Gérard JP. Preliminary results of a phase II study of high-dose radiation therapy and neoadjuvant plus concomitant 5-fluorouracil with CDDP chemotherapy for patients with anal canal cancer: a French cooperative study. Ann Oncol. 1997 ;8:575-81. 22. James R, Pointon R, Martin S. Local radiotherapy in the management of squamous carcinoma of the anus. Br J Surg 1985; 72: 282-5. 23. UKCCR. Anal Cancer Trial Working Party. Epidermoid anal cancer: results from the UKCCCR randomized trial of radiotherapy alone versus radiotherapy 5 fluorouracil and mitomycin. Lancet 1996; 348: 1049-54. 24. Cicchini C, Stazi A, Ciardi A, Ghini C, Inindinnimeo M. An unusual late radiotherapy-related complication requiring surgery in anal canal carcinoma. J Surg Oncol 2000; 74: 167-70. 25. Bobin JY, Gerard JP, Chapet O, Romestaing P, Isaac S. Lymphatic mapping and inguinal sentinel lymph node biopsy in anal canal cancers to avoid prophylactic inguinal irradiation. Cancer Radiother 2003; 7 suppl 1:85s-90s. 26. Perera D, Pathma-Nathan N, Rabbitt P, Hewett P, Rieger N. Sentinel Node Biopsy for Squamous-Cell Carcinoma of the Anus and Anal Margin. Dis Col and Rectum 2003; 8: 1027-1031 27. Ulmer C, Bembenek A, Gretschel S, Markwardt J, Koswig S , Schneider U, Schlag PM, Refined Staging by Sentinel Lymph Node Biopsy to individualize Therapy in Anal Cancer. Ann of Surg Oncol, 11:259S–262S. Page 6 of 9 WMC001565 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 07:35:37 AM 28. Péley G, Farkas E, Sinkovics I, Kovács T, Keresztes S, Orosz Z, Köves I. Inguinal sentinel lymph node biopsy for staging of anal cancer. Scandinavian Journal of Surgery 91: 336–338, 2002. 29. D. Nagle, D. Henry, A. Iagaru, J. Mastoris, L. Chmielewski, J. Rosenstock The utility of PET scanning in the management of squamous cell carcinoma of the anus. 2006 ASCO Annual Meeting. Journal of Clinical Oncology, 2006 ASCO Annual Meeting Proceedings Part I. Vol 24, No. 18S (June 20 Supplement), 2006: 4152. 30. B. Nguyen, D. Joon, V. Khoo, G. Quong, M. Chao, M. Wada, M. Joon, A. See, M. Feigen, K. Rykers. Assessing the impact of FDG-PET in the management of anal cancer. Radiotherapy and Oncology 2008; 87 : 376-382. WebmedCentral > Review articles Page 7 of 9 WMC001565 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 07:35:37 AM Illustrations Illustration 1 Table 1 TNM Staging of Squamous Cell Carcinoma of the anal canal Primary tumor (T) T1: Tumor 2 cm or less in greatest dimension T2: Tumor more than 2 cm but not more than 5 cm in greatest dimension T3: Tumor more than 5 cm in greatest dimension T4: Tumor of any size that invades adjacent organ(s), Regional lymph nodes N0: No regional lymph node metastasis N1: Metastasis in perirectal lymph node(s) N2: Metastasis in unilateral internal iliac and/or inguinal lymph node(s) N3: Metastasis in perirectal and inguinal lymph nodes and/or bilateral internal iliac and/or inguinal lymph nodes Distant metastasis (M) M0: No distant metastasis M1: Distant WebmedCentral > Reviewmetastasis articles Page 8 of 9 WMC001565 Downloaded from http://www.webmedcentral.com on 24-Dec-2011, 07:35:37 AM Disclaimer This article has been downloaded from WebmedCentral. With our unique author driven post publication peer review, contents posted on this web portal do not undergo any prepublication peer or editorial review. It is completely the responsibility of the authors to ensure not only scientific and ethical standards of the manuscript but also its grammatical accuracy. Authors must ensure that they obtain all the necessary permissions before submitting any information that requires obtaining a consent or approval from a third party. Authors should also ensure not to submit any information which they do not have the copyright of or of which they have transferred the copyrights to a third party. Contents on WebmedCentral are purely for biomedical researchers and scientists. They are not meant to cater to the needs of an individual patient. The web portal or any content(s) therein is neither designed to support, nor replace, the relationship that exists between a patient/site visitor and his/her physician. Your use of the WebmedCentral site and its contents is entirely at your own risk. We do not take any responsibility for any harm that you may suffer or inflict on a third person by following the contents of this website. WebmedCentral > Review articles Page 9 of 9