Medication Reconciliation - Canadian Patient Safety Institute
advertisement

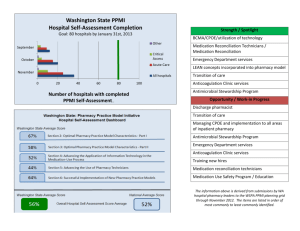
Rapid Fire Presentations Fraser Health Region - BC Capital Health Region – AB Northern Health Region - BC Providence Health Care - BC Vancouver Coastal Health – BC BC Mental Health and Addiction Services – BC BREAK Interior Health Region - BC Vancouver Island Health Region - BC Winnipeg Regional Health - MB Calgary Health Region - AB Children’s and Woman’s - BC Medication Reconciliation Janice Munroe Pharmacy Medication Safety Coordinator November 29, 2005 Where are we in Fraser Health? ¾ Executive level support ¾ Senior level multidisciplinary Steering Committee ¾ Identification of Pilot site ¾ Peace Arch Hospital ¾ Engagement of leaders at pilot site ¾ Identification of Project Team leads and members ¾ Co-leads ¾ Multidisciplinary Team ¾ Draft Project Charter Pilot Team - Project Plan ¾ Finalize Project Charter ¾ Develop Project Timelines ¾ Process flow mapping ¾ Identify resources required to complete Items for consideration…… ¾ Initial pilot area – admission vs discharge ¾ Site Project Team evolution as spread occurs ¾ Spread to other FH sites – multiple vs single? ¾ Community involvement – phase I or II or?? The Road Ahead….. ¾ Impossible to envision all of the issues that will arise ¾ Strong executive support ¾ Goal of the dedicated multidisciplinary team is to improve patient care ¾ Working together we will succeed! Rapid Fire Presentations Fraser Health Region - BC Capital Health Region – AB Northern Health Region - BC Providence Health Care - BC Vancouver Coastal Health - BC Interior Health Region - BC BC Mental Health and Addiction Services - BC Vancouver Island Health Region - BC Winnipeg Regional Health - MB Calgary Health Region - AB Children’s and Woman’s - BC Safer Healthcare Now!Medication Reconciliation Suburban/Rural Capital Health, AB Who? Primary/Secondary care sites • Westview Health Centre- Stony Plain • Redwater Health Centre• Fort Saskatchewan Health Centre • Devon General Hospital • Leduc Community Hospital • Sturgeon Community Hospital September 2005 9 September 2005 10 Our Team Project Coordinator – Esther Nelles (0.4 FTE) Pharmacists Maryann Chmilar (0.5 FTE) RN - 0.5 FTE Educator - 0.5 FTE Nurse ClinicianSturgeon Community Hospital (1.0 FTE) September 2005 11 Next Steps Hire the remaining members of the team. December- informing the stakeholders of the plan and its implications September 2005 12 Rapid Fire Presentations Fraser Health Region - BC Capital Health Region – AB Northern Health Region - BC Providence Health Care - BC Vancouver Coastal Health - BC Interior Health Region - BC BC Mental Health and Addiction Services - BC Vancouver Island Health Region - BC Winnipeg Regional Health - MB Calgary Health Region - AB Others... 13 Medication Reconciliation in Northern BC Presenters: Cam Egli and Greg Atherton Northern Health 9 Safer Healthcare Now! – Multi-disciplinary teams established in each of three HSDA’s z Each team’s membership varies – Medication Reconciliation “team” is reporting to NI HSDA working Group z Members: Greg Atherton (Rx) – Quesnel – Cam Egli (Rx) - Regional Director – Bruna Schnepf (RN and Admin) – Omineca Director of Nursing – RN and MD in Quesnel - TBA – 15 Northern Health ¾ NH Team is just forming ¾ Initial meeting planned in December ¾ Aim statement ¾ Reduce the mean number of unintentional discrepancies at admission on the pilot unit by 50% within three months ¾ Baseline data - yet to be compiled ¾ Plan for the region ¾ Start with pilot project in Quesnel (GR Baker Hospital) ¾ Roll out to one site within each HSDA (Dawson Creek and Smithers) ¾ NH-wide roll out coupled to new CIS 16 Northern Health ¾ Complexities we face: ¾ ¾ ¾ Many software programs in NH Rx Geography Human resources 17 Rapid Fire Presentations Fraser Health Region - BC Capital Health Region – AB Northern Health Region - BC Providence Health Care - BC Vancouver Coastal Health - BC BC Mental Health and Addiction Services - BC Interior Health Region - BC Vancouver Island Health Region - BC Winnipeg Regional Health - MB Calgary Health Region - AB Children’s and Woman’s - BC Medication Reconciliation Vancouver Coastal Health Providence Health Care Providence Healthcare • St. Paul’s Hospital – 426 tertiary acute care beds • Mount St. Joseph Hospital – 128 community acute care beds – 100 residential care beds • Holy Family Hospital – 142 residential care beds – 76 rehab beds • St. Vincent’s Hospitals – 369 residential care beds • Youville – 84 residential care beds September 2005 20 Medication Reconciliation at PHC • Team formed ~ 2 ½ years ago – Pharmacy, nursing, pharmacy IT – Acute and Residential care • Focusing on transitions at: – Admitting – Transfer • Acute Æ Acute • Acute Æ Residential – Discharge September 2005 21 Regionalization of Pharmacy Services VCH/PHC Beds by Site and Type 800 600 Acute - Tertiary Beds Acute - Community Residential 400 Rehab 200 0 0 1 September 2005 2 3 Site 4 5 6 22 Opportunities for Reconciliation Opportunities for Reconciliation 800 Community Contracted Facilities 600 Acute - Tertiary Beds Acute - Community Residential 400 Rehab 200 0 0 1 September 2005 2 3 Site 4 5 6 23 Regional Medication Reconciliation Initiatives • Report to Regional Medicine Council • Teams at – – – – – Richmond Vancouver Acute PHC Lions Gate Sunshine Coast/Garibaldi September 2005 24 Pharmacy Startup Meeting • • • • • • • • Availability of data Extraction of data User access Current processes Pilot Membership Resources Evaluation September 2005 25 Pharmacy Startup Meeting • Decisions – VA, NS and PHC to focus on the discharge process – RGH under discussion – Sunshine coast to focus on admission process • Tasks – – – – Define membership at local level Structure Start-up meeting Discharge prescription feasibility and implementation cost September 2005 26 Regional Medication Reconciliation Initiatives September 2005 27 Rapid Fire Presentations Fraser Health Region - BC Capital Health Region – AB Northern Health Region - BC Providence Health Care - BC Vancouver Coastal Health - BC BC Mental Health and Addiction Services - BC Interior Health Region - BC Vancouver Island Health Region - BC Winnipeg Regional Health - MB Calgary Health Region - AB Others... Lions Gate Hospital North Shore Coast Garibaldi VCH Team: Romilda Ang: Director Professional Practice Derek Andrews: Pharmacy Computer Coordinator Mark Collins: Pharmacy Clinical Coordinator Baseline Survey Emergency Department October 2005 ER pharmacist 18 admitted patients over 6 days. N = 121 Rx’s Average = 7 Rx’s per patient (n = 2-17) 35 min. per patient Baseline discrepancy rate Mean Discrepancy Rate Number/ Patient Undocumented Intentional (Documentation Accuracy) 0.6 Unintentional (Rate of error) 0.7 Incidence of Intended Therapy: None AND Intentional = 80% (MRSI) Patients with discrepancy Patients (N=18) Discrepancy Number Percent Intentional 14 78 % Unintentional 4 22% Undocumented 7 39% Undocum. OR Uninten. 9 50 % Information Systems: Testing McKesson Computer Upgrade Home Medication Reports Medication Reconciliation Report Medication Discharge Reconciliation Report Discharge Planning Report Rapid Fire Presentations Fraser Health Region - BC Capital Health Region – AB Northern Health Region - BC Providence Health Care - BC Vancouver Coastal Health - BC BC Mental Health and Addiction Services - BC Interior Health Region - BC Vancouver Island Health Region - BC Winnipeg Regional Health - MB Calgary Health Region - AB Others... MEDICATION RECONCILIATION Nov. 29, 2005 B.C. Mental Health and Addiction Services Medication Reconciliation Committee Riverview Hospital Forensic Psychiatric Institute Forensic Clinics Representation from Nursing, Pharmacy, Medicine September 2005 36 Admission Reconciliation Staff education/awareness Collect baseline data Getting started kit Retrospective analysis of patient charts in 3 different areas: Riverview Hospital (Forensic Psychiatric Institute, and Forensic Clinics) Intentional discrepancy Undocumented intentional/unintentional September 2005 Pharmacy, nursing, medicine 37 Admission Reconciliation Meet to discuss Results of baseline data Plan next steps Staffing requirements Do we need to modify the forms for AR? Team make-up Barriers/ Challenges September 2005 38 NEXT…. September 2005 39 BREAK September 2005 40 Rapid Fire Presentations Fraser Health Region - BC Capital Health Region – AB Northern Health Region - BC Providence Health Care - BC Vancouver Coastal Health - BC BC Mental Health and Addiction Services - BC Interior Health Region - BC Vancouver Island Health Region - BC Winnipeg Regional Health - MB Calgary Health Region - AB Others... Interior Health Medication Reconciliation Norma Malanowich Regional Director, Pharmacy 43 Very Early Stages of Planning & Definition Pharmacy Lead Medication Reconciliation 1. Specific populations of patients admitted from Emergency – Pilots at Kelowna General Hospital and Royal Inland Hospital 2. Medication Reconciliation incorporated into pharmacy anticoagulation service and medication consultation process. – Pilot locations to be determined: Vernon Jubilee Hospital + ??? 3. Admission to Residential Care 44 Nursing Lead Medication Reconciliation 1. Patient Discharge – Pilot facilities and units tbd 45 Team Composition • Sponsored by Quality, Pharmacy, and site Medication Safety and Advisory Committees • Multi-disciplinary teams created for each pilot 46 How to get started and avoid the pitfalls: We’re here to learn from you! Rapid Fire Presentations Fraser Health Region - BC Capital Health Region – AB Northern Health Region - BC Providence Health Care - BC Vancouver Coastal Health - BC BC Mental Health and Addiction Services - BC Interior Health Region - BC Vancouver Island Health Region - BC Winnipeg Regional Health - MB Calgary Health Region - AB Children’s and Woman’s - BC MEDICATION RECONCILIATION Richard Bachand Pharm D Department of Pharmacy November 29th, 2005 September 2005 48 Team Newly formed Team Leader Nurse Manager Clinical Nurse Leader Clinical Nurse Educator Pharmacy Resident Surgeon One of our “Big dot” projects with an executive sponsor September 2005 49 Focus Medication reconciliation “ on admission” Where? 1 to 2 Surgical Units Planning on involving the pre-admission clinics (PAC) Baseline data In progress Developed • Pharmacist consult – medication reconciliation form (BPMH) • Home Medication Reconciliation and Order Form September 2005 50 CHALLENGES ¾ Manpower resources ¾ Culture ¾ Complex systems September 2005 51 Rapid Fire Presentations Fraser Health Region - BC Capital Health Region – AB Northern Health Region - BC Providence Health Care - BC Vancouver Coastal Health - BC BC Mental Health and Addiction Services - BC Interior Health Region - BC Vancouver Island Health Region - BC Winnipeg Regional Health - MB Calgary Health Region - AB Others... Medication Reconciliation Current Status within the Winnipeg Regional Health Authority Regional Approach Proposal & Budget Leadership buy-in Role of the Project Management Office (PMO) Standardized form and process Site Selection Recruitment of unionized staff September 2005 54 GOAL To develop & implement a regional MedRec process throughout the continuum of care including: admission to an acute care unit referral to home care primary care September 2005 55 Objectives È the mean # undocumented intentional discrepancies by 75% by December 31, 2006. È the mean # unintentional discrepancies by 50% by December 31, 2006. Ç the MedRec Success Index by 50% by December 31, 2006. Spread the MedRec Process to 100% of Medicine/Family medicine acute care units by December 31, 2006. The MedRec Process is completed within 24 hours in 90% of patients upon admission. September 2005 56 Framework Pilot units Acute care - General/Family Medicine - 6 Home care - 2 Primary Care - 2 Initial focus admission process standardized form and process include allergies September 2005 57 Framework Spread to other units Pilot units start testing/development of the transfer/discharge process Project Team Staffing frontline staff 12 - 0.4 EFT nurses 2 pharmacists (1.6 EFT total) September 2005 58 Pre-Planning Education for project team Oct 4 workshop Overview of med reconciliation, model for improvement Oct 24, 25 focus on process improvement “hands on” PDSA cycles Ongoing as needed Site visits September 2005 59 Pre-Planning Regional Project Team Meetings Pre-PDSA work networking with other teams baseline audit develop draft med reconciliation form flow charting template for how to perform med history criteria for pharmacist involvement develop local teams communication plan September 2005 60 Challenges Multi-site pilot units Baseline audit Communication Spread Unions Forms Committee(s) Scheduling of project team September 2005 61 Baseline Audit Diltiazem CD 120 mg OD 240 mg MD changed Ramipril 10 mg OD Amiodarone 100 mg OD Clopidogrel (HOLD) Ranitidine 150 mg OD Prednisone 5 mg OD Acetazolamide 250 mg OD 10 mg MD changed Atorvastatin 10 mg OD Glyburide 5 mg BID Salbutamol 2 puffs BID QID Pilocarpine 2% 1 drop to BOTH eyes QID RIGHT eye September 2005 62 Challenges Multi-site pilot units Baseline audit Communication Spread Unions Forms Committee(s) Scheduling of project team September 2005 63 Questions? Rapid Fire Presentations Fraser Health Region - BC Capital Health Region – AB Northern Health Region - BC Providence Health Care - BC Vancouver Coastal Health - BC BC Mental Health and Addiction Services - BC Interior Health Region - BC Vancouver Island Health Region - BC Winnipeg Regional Health - MB Calgary Health Region - AB Children’s and Woman’s - BC Medication Reconciliation Calgary Health Region, Alberta Presented by: Jamie Stroud, QI Consultant, Internal Medicine, Unit 74 RGH and Debbie Friesen, Clinical Pharmacist, Unit 32 FMC Who’s on What? – Vancouver, BC. November 29, 2005 Team Make-up • Unit 74 RGH •1 •2 •2 •1 •1 •1 •0 physician clinical pharmacists clinical nurse educators unit manager QI consultant transition coordinator RNs Who’s on What? – Vancouver, BC. November 29, 2005 Initial Flow Map Who’s on What? – Vancouver, BC. November 29, 2005 Unit 74 Baseline Measures (n=20) Success Index – 68.9% Mean # of Undocumented Intentional Discrepancies – 3.05 Mean # of Unintentional Who’s on What? – Vancouver, BC. Discrepancies – 0.50 November 29, 2005 Unit 74 – Next Steps • Refine team • Understand variability • Brainstorm ideas for change • Set goals • Complete Improvement charter • Select area for improvement • Prepare for PDSA cycle #1 Who’s on What? – Vancouver, BC. November 29, 2005 Team Make-up • Unit 32 FMC • 1 QI physician • 2 Hospitalist physicians • 2 clinical pharmacists • 1 APC nurse manager • 1 QI consultant • 1 staff nurse • 1 hospitalist nurse liaison • 1 program manager family Who’s on What? – medicine Vancouver, BC. November 29, 2005 Improving the Process (Unit 32) CALGARY HEALTH REGION FAMILY PHYSICIAN: ____________________________________ COMMUNITY PHARMACY: _______________________________ Medication Allergies/Intolerances (include specific patient reaction if known): PRE-ADMISSION MEDICATION LIST PRESCRIPTION MEDICATIONS ON ADMISSION Dosing Interval Hold or D/C Route Change Medication Name & Dose Continue (pills, eye drops, patches, inhalers, etc.) Reason for Change/ Hold/ Discontinuation NON-PRESCRIPTION MEDICATIONS (OTC’s, herbals, etc.) Source of Medication List (check all used): Review of medication vials Who’s on What? – Vancouver, BC. Family Physician list Review of patient medication list EMS record Patient recall Wellnet list Family Recall Medication Administration Record from another facility Pharmacy list Other (specify): November 29, 2005 Measures for Unit 32 (FMC) Success Index: Baseline - 56.9% (Improvement over time) Goal: 85% (increase by 50%); Stretch Goal: 100% (increase by 75%) Mean # of undocumented intentional discrepancies: Baseline - 1.2 (Documentation accuracy) Goal: 0.3 (decrease by 75%); Stretch Goal: 0.2 (decrease by 80%) Mean # of unintentional discrepancies: Baseline - 1.7 (Rate of error) Goal: 1.275 (decrease by 25%); Stretch Goal: 0.42 (decrease by 75%) Who’s on What? – Vancouver, BC. November 29, 2005 Success Index 100 P e rc e nt 80 60 40 Baseline (n=24) PDSA 1: Form Version 1 (n=7) PDSA 2: Form Version 2 (n=5) PDSA 3: Form Version 3 (n=11) 20 0 Aug.-Sep., 2005 Who’s on What? – Vancouver, BC. Oct. 12, 2005 Oct. 25, 2005 Nov. 16/17, 2005 November 29, 2005 M e a n # o f D is c r e p a n c ie s Mean # of Undocumented Discrepancies 1.8 1.6 1.4 1.2 1 0.8 0.6 0.4 0.2 0 Baseline (n=24) Aug.-Sep., 2005 Who’s on What? – Vancouver, BC. PDSA 1: Form Version 1 (n=7) Oct. 12, 2005 PDSA 2: Form Version 2 (n=5) Oct. 25, 2005 PDSA 3: Form Version 3 (n=11) Nov. 16/17, 2005 November 29, 2005 M e a n # o f D is c r e p a n c ie s Mean # of Unintentional Discrepancies 2 1.8 1.6 1.4 1.2 1 0.8 0.6 0.4 0.2 0 Baseline (n=24) PDSA 1: Form Version 1 (n=7) PDSA 2: Form Version 2 (n=5) PDSA 3: Form Version 3 (n=11) Aug.-Sep., 2005 Who’s on What? – Vancouver, BC. Oct. 12, 2005 Oct. 25, 2005 Nov. 16/17, 2005 November 29, 2005 Next Steps • Additional PDSA Cycles • Further explore Nursing role • Explore use of form by multiple health care professionals • Pilot screening tool • Monitor progress Who’s on What? – Vancouver, BC. November 29, 2005 Rapid Fire Presentations Fraser Health Region - BC Capital Health Region – AB Northern Health Region - BC Providence Health Care - BC Vancouver Coastal Health - BC Interior Health Region - BC Vancouver Island Health Region - BC Winnipeg Regional Health - MB Saskatoon Health Region - SK Calgary Health Region - AB Children’s and Woman’s - BC Medication Reconciliation BCCH Emergency Department The Team Dr. Jeffrey Hung – Medicine, ED Denise Hudson – Quality Initiatives, ED Norma Donovan – CNC, ED Faye Kingdon – Programme Manager, ED Judy Komori – Leader, Quality Safety & Risk Management Kim Shearer – Sr. Practice Leader, Nursing Projects Ian Sheppard – Director, Pharmacy September 2005 80 Current & Future Plans Start in the Children’s Emergency Department Collect baseline data Refine data collection and analysis tools; implement fully in Emergency Develop a “roll out” plan for the rest of C&W – paediatrics and maternity September 2005 81 Baseline Data To be collected in December 2005 Chart Audit (retrospective) September 2005 seen in the Emergency department, and admitted to an inpatient unit, and taking 5 for more medications 82 Challenges Resource challenges Time for staff who have been assigned to do the work, and Staff with IT skills needed to search and/or write custom reports to find the required information in electronic databases Finding the patients who meet the criteria September 2005 83 Charter September 2005 84 AIM Statements September 2005 85 Lunch Time! Thank you very much…