ICD-10-CM/PCS Coding Changes for Surgery
advertisement

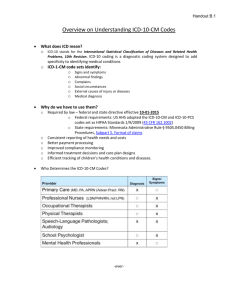
ICD-10-CM/PCS: Coding and Clinical Documentation Changes Surgery Presented by: Angie Audler, MBA, RHIT, CCS, CPC, AHIMA Approved ICD-10-CM/PCS Trainer Copyright c 2015 Confidential and Proprietary Information Disclaimer • This PowerPoint presentation is an education tool to provide basic information for coding. The information is the sole view of the author and was put together based on experience, research and expertise in the coding profession. It is not intended to be an exhaustive review and should not be considered a substitution for Coding Guidelines. The presenter does not accept any responsibility or liability with regard to errors, omissions misinterpretations or misuse by the audience. Copyright c 2015 Confidential and Proprietary Information Today’s Topics • • • • Brief Overview of ICD-10-CM/PCS How does ICD-10 Impact you as a Provider Common Surgery ICD-10 Codes Clinical Documentation Awareness Tips for ICD-10 Copyright © 2015 Confidential and Proprietary Information Compliance Date • October 1, 2015 – Date of service on or after 10/01/2015 for office and other outpatient services (including Hospital Observation) • ED and Observation services prior to 10/1 with overlap on or after 10/1 will use ICD9 codes for reporting – Discharge date on or after 10/01/2015 for hospital inpatient discharges – Claims for services prior to 10/1/2015 will continue to flow through systems utilizing ICD-9-CM diagnosis and ICD-9-CM Vol. 3 procedure codes (for facilities) for a period of time 4 CMS Concession Source: Healthcare IT News 7/6/2015 • CMS has indicated that "a valid ICD-10 code will be required on all claims starting Oct. 1, 2015.“ – 1. Claims denials. "While diagnosis coding to the correct level of specificity is the goal for all claims, for 12 months after ICD-10 implementation, Medicare review contractors will not deny physician or other practitioner claims billed under the Part B physician fee schedule through either automated medical review or complex medical record review based solely on the specificity of the ICD-10 diagnosis code as long as the physician/practitioner used a valid code from the right family," CMS officials wrote in a guidance document. Copyright c 2015 Confidential and Proprietary Information CMS Concession Source: Healthcare IT News 7/6/2015 • 2. Quality reporting and other penalties. "For all quality reporting completed for program year 2015 Medicare clinical quality data review contractors will not subject physicians or other Eligible Professionals (EP) to the Physician Quality Reporting System (PQRS), Value Based Modifier (VBM), or Meaningful Use 2 (MU) penalty during primary source verification or auditing related to the additional specificity of the ICD-10 diagnosis code, as long as the physician/EP used a code from the correct family of codes," CMS explained. "Furthermore, an EP will not be subjected to a penalty if CMS experiences difficulty calculating the quality scores for PQRS, VBM, or MU due to the transition to ICD-10 codes." Copyright c 2015 Confidential and Proprietary Information CMS Concession Source: Healthcare IT News 7/6/2015 • 3. Payment disruptions. “If Medicare contractors are unable to process claims as a result of problems with ICD-10, CMS will authorize advance payments to physicians,” AMA president Steven Stack, MD, noted on the group’s website. Copyright c 2015 Confidential and Proprietary Information CMS Concession Source: Healthcare IT News 7/6/2015 • 4. Navigating transition problems. CMS intends to create a communication center of sorts, including an ICD-10 Ombudsman, "to help receive and triage physician and provider issues." The center will also "identify and initiate“ resolution of issues caused by the new code sets, officials added. Copyright c 2015 Confidential and Proprietary Information Brief Overview of ICD-10-CM/PCS • ICD-10 is composed of two parts: – ICD-10-CM (clinical modification) – ICD-10-PCS (procedural coding system) Copyright c 2015 Confidential and Proprietary Information The Difference Between ICD-10-CM/PCS • ICD-10-CM – Replaces ICD-9-CM Vol. 1 & 2 Codes – ICD-10-CM will be used to identify diagnosis codes in all health care settings • ICD-10-PCS – Replaces ICD-9 Vol. 3 Procedure Codes (facility use only) ICD-10PCS will be used by facilities to report procedures in the hospital inpatient setting • Physicians and Other Healthcare Professionals will continue to use CPT and HCPCS (Level II) codes to report office and other procedures and services • Hospital Outpatient Departments/OPSurgery and Ambulatory Surgery Centers will also continue to use CPT and HCPCS (Level II) codes for reporting outpatient procedures and ancillary services Copyright c 2015 Confidential and Proprietary Information ICD-10-PCS • Under ICD-10, new and cutting-edge technology that have been problematic to code in ICD-9 will be assigned based on surgeon’s documentation in the operative note – – – – – – – Type of surgery Body system Root operation Body part Approach Device Qualifiers (e.g. biopsy, second site, etc.) Copyright c 2015 Confidential and Proprietary Information Overview of ICD-10-CM • The transition to ICD-10 affects all HIPAA-covered entities – hospitals, physicians, allied health professionals, home health, skilled nursing, etc.; as well as payers, business associates – billing companies, vendors, clearinghouses • Non-covered entities (e.g. automobile insurance and worker’s compensation programs are not required to transition to ICD-10), although it is recommended Copyright © 2015 Confidential and Proprietary Information ICD-10-CM Changes • There are three main categories of changes in ICD-10-CM - Definition Changes - Differences in Terminology - Increased Documentation Specificity • ICD-10 doesn’t affect coding only; it involves physician reporting, billing, information technology, and revenue management Copyright © 2015 Confidential and Proprietary Information Comparison 14 ICD-10-CM • Although there are approximately 70,000 codes in ICD-10, specialists will use only a small subset of those codes • You will be surprised at how much of this work you are already doing • Over 1/3 of the expansion codes are due to laterality (physicians are already documenting right, left, bilateral) – If bilateral and there is no specific code for bilateral, you code both right and left sides 15 Overview of ICD-10-CM • ICD-9 codes will no longer be maintained once ICD-10 is implemented • A claim cannot contain both ICD-9-CM and ICD-10-CM (CMS Transmittal 950, effective 10/1/2013) 16 Risk Mitigation • Denials can run high for “not medically necessary reasons” • In the beginning there is risk of payers not fully mapping procedures with new allowed diagnosis reasons – Be prepared for short term reduced revenues 17 Louisiana Medicaid Source: Modern Healthcare, 9/4/2015 • Four State Medicaid Programs will NOT Transition to ICD-10 by 10/1 • CMS will allow four states - California, Louisiana, Maryland and Montana - to use a "crosswalk technique" to continue using the older code sets for Medicaid fee-forservice programs because their claims processing systems in these four states are unable to use the new ICD-10 codes. • Under the crosswalk technique, the Medicaid programs will convert claims using the ICD10 system into ICD-9 codes to calculate payments • Some provider groups and healthIT experts say the use of such a technique could result in payment delays and other issues. • It was not stated whether this applies to straight Medicaid and/or the Medicaid Bayou Plans. Stay tuned for additional information to be released • 18 Administrative Considerations • Reimbursement • Potential effect of delays, initial decrease in coder productivity • (Industry estimates 20-30% reduction in coder productivity due to additional specificity; physician queries; loss of memorized codes; learning curve.) • Decrease in physician/provider productivity due to additional specificity needed in charting; additional specificity needed for orders; additional specificity for authorizations; answering queries; increased selection on charge tickets and/or order sets 19 ICD-10-CM Structure 20 ICD-10-CM Structure • The seventh character represents a visit encounter or sequelae (condition resulting from a previous disease; also known as Late Effects) for injuries and external causes. The seventh character extender must always be the seventh character of a code. • A hyphen “-” at the end of an ICD-10 code in the Alphabetic Index indicates that additional characters are required. • Placeholder: An “x” is used as a fifth character in certain six character codes to allow for future expansion. An “x” is also used as a placeholder when a code has less than six characters and the code requires a seventh character. • • • • For Example: Adverse effect of calcium-channel blockers, initial encounter T46.1x5A Exposure to electric transmission lines, initial encounter W85.xxxA Post-procedural cardiogenic shock, initial encounter T81.11xA 21 Noteworthy Changes that Fall into Other Specialty Areas Clinical Area ICD-9-CM Codes ICD-10-CM Codes Fractures 787 17099 Pregnancy 1104 2155 Diabetes 69 239 Hypertension 33 14 ESRD 11 5 Brain Injury 292 574 22 Considerations • Font (System and Penmanship) – Watch I (alpha) vs. 1 (numeric) – Watch O (alpha) vs. 0 (numeric) – Watch Z (alpha) vs. 2 (numeric) 23 Reporting Differences, Trending and Analytic Modifications • Converting from ICD9 to ICD10 more than triples the number of available codes • Looking at historical data becomes problematic unless you can identify and capture needed information from the two coding systems • Simple forward mapping will not be sufficient for most providers to make a successful transition Copyright © 2015 MEDKODER LLC Confidential and Proprietary Information 24 ICD-10-CM • You will need to map your most frequently used ICD-9-CM codes to ICD-10-CM • Due to the number of code choices with some diagnoses, there may be some challenges with charge ticket/superbill options and EHR template “drop-downs” Copyright © 2015 Confidential and Proprietary Information General Equivalency Maps (GEMS) • CMS’ GEMS (General Equivalency Maps) demonstrate the complexity involved in moving between the two coding systems Copyright © 2015 MEDKODER LLC Confidential and Proprietary Information 26 ICD9/ICD10 Relationships 1:1, Cluster, Combination, Complex • Individual ICD-9 codes that map to several ICD-10 code alternatives; • Individual ICD-9 codes that map to a set of two of more ICD10 codes; • Two or more ICD-9 codes that map to individual ICD-10 codes; • ICD-9 codes with no representation in ICD-10; • ICD-9 codes with an exact match in ICD-10; and • Individual ICD-9 codes that map to codes with similar but not identical meanings in ICD-10 Copyright © 2015 MEDKODER LLC Confidential and Proprietary Information 27 CMS General Equivalent Mappings Source: http://firstillinoishfma.org/wp-content/uploads/McGladrey-ICD-10-April-2013.pdf Copyright © 2015 MEDKODER LLC Confidential and Proprietary Information 28 Documentation Awareness • Physicians are becoming more aware of the value of clinical data and the relationships between their professional profiles and the diagnosis (ICD-9/ICD-10) and procedure codes (CPT) assigned • If the clinical documentation and the codes do not accurately and specifically represent the work you do, it could poorly reflect through reporting and impact your future reimbursement Copyright c 2015 Confidential and Proprietary Information ICD-10 Will Have a Direct Impact on Physicians Through….. • Physician quality profiles (PQRS, VBPM, P4P) – mortality and morbidity reporting – Not every insurer is profiling physicians yet, but there are several other entities that do (e.g. Health Grades – licensing backgrounds and disciplinary information) – Payers that profile use their own home-grown grading systems that use claims data to determine both “quality” and “efficiency” Copyright © 2015 Confidential and Proprietary Information Provider Profiling • Not all care or every specialty can be measured • Most programs focus on specific types of physicians and services • Most common specialties profiled: Cardiology Pediatrics Pulmonary Allergy OB/GYN Rheumatology Endocrinology Nephrology Infectious Disease Family medicine Neurology Internal Medicine Orthopedics Copyright © 2015 Confidential and Proprietary Information Provider Profiling • Most common diagnoses monitored: – All of the major heart, lung and organ diseases – The most prevalent viruses and inflammation – Screening for cancers and depression – Immunization compliance rates Copyright c 2015 Confidential and Proprietary Information Provider Profiling • Provider Efficiency - Payers compare a physician’s data to their local market benchmarks for cost of resources used in delivering healthcare - ICD-10 codes will capture the management of chronically ill patients Copyright © 2015 Confidential and Proprietary Information Manage Your Profile • Payers will provide you with feedback on your scores in the quality and efficiency areas profiled • Reports include details on the patients used for scoring • Validate or refute the findings, as these scores may have an impact on your bottom line in 2017 with governmental and third party payers Copyright © 2015 Confidential and Proprietary Information Do You Code Your Own Services? • If you do not code your services, then training will be limited to ICD-10 concepts of the specialty and documentation changes • If you do your own coding, then you will need training on the code set and coding guidelines – Be sure to read the Chapter Specific Guidelines located in front of the ICD-10CM coding manual Copyright © 2015 Confidential and Proprietary Information HIPAA Regulations • HIPAA regulations require providers and thirdparty payers to adhere to Official Guidelines for Coding and Reporting • A violation of coding guidelines is a violation of HIPAA Copyright © 2015 MEDKODER LLC Confidential and Proprietary Information 36 Unspecified Code Assignment • Surveys indicate that as much as 50% of current physician documentation cannot be coded to appropriate level of specificity with ICD-10 resulting in unspecified code use • Many unspecified codes in ICD-10-CM include the note: *Codes with a greater degree of specificity should be considered first Copyright © 2015 Confidential and Proprietary Information Unspecified Codes • Sometimes the use of unspecified codes makes sense – Early in the course of evaluation – Secondary diagnoses not directly being treated by that provider but impacts that encounter – Generalist vs specialist • Area of expertise – the diagnosis may not be in the providers scope of expertise and will need to get the opinion of a specialist • Payers are discouraging the use of unspecified codes – When providers review their severity and risk scores it may impact their reimbursement because it won’t have the specificity in their codes that are needed to justify higher levels and better reimbursement 38 Table of Drugs and Chemicals Underdosing Adverse Effect Poisoning, Assault Poisoning, Intentional Self-harm Copyright © 2015 MEDKODER LLC Confidential and Proprietary Information Poisoning, Undetermined Substance Poisoning, Accidental (unintentional) • The Table of Drugs and Chemicals Headings better describe the circumstance of the encounter • It also contains a new columns for “Adverse Effect” and “Underdosing” 39 Underdosing (Of Medication Regimen) (Z91.12-, Z91.13-) • New concept term in ICD-10 (patient is taking less of a medication than prescribed) • Today’s terminology – Non-compliance of medication Documentation Awareness When documenting Underdosing of medication regimen include: • • • • Intentional Unintentional Non-compliance Reason – financial hardship; age related debility • The medical condition is sequenced first, with the underdosing listed as a secondary diagnosis 40 Underdosing or Failure in Dosage During Medical or Surgical Care (Y63.6, Y63.8 - Y63.9) • Y63- describes the circumstance causing an injury, not the nature of the injury • It should not be used as a principal diagnosis (always list as secondary) Copyright c 2015 Confidential and Proprietary Information Initial vs. Subsequent Encounters • One of the biggest misconceptions inherent to ICD-10 is the qualifier term “subsequent” encounter • The designation subsequent is meant to describe the patient has received active treatment (initial) and the physician is now providing routine care (subsequent) during the healing or recovery phase Copyright c 2015 Confidential and Proprietary Information Physician vs. Facility Requirements • Although physicians will continue to use CPT codes to report their procedures and services, you will need to remain cognizant of the documentation specificity that hospitals will need to report procedures/services with ICD10-PCS for inpatients Copyright c 2015 Confidential and Proprietary Information ICD-10-PCS Code Structure Character 1 Character 2 Character 3 Character 4 Character 5 Character 6 Character 7 Section Body System Root Operation Body Part Approach Device Qualifier Copyright c 2015 Confidential and Proprietary Information Inpatient Procedures • New and cutting-edge technology that have been problematic to code for hospitals in ICD-9 will be assigned in ICD-10-PCS based on surgeon’s documentation in the operative note – Type of surgery – e.g. medical, surgical – Body system – e.g. Heart and Great Vessels – Root operation – e.g. Ablation, Bypass, Excision, Revision, etc. – Body part – e.g. Coronary arteries, veins – Approach – e.g. open, percutaneous – Device – e.g. stent, none – Qualifiers (e.g. biopsy, second site, bifurcation, etc.) Copyright c 2015 Confidential and Proprietary Information General Documentation Tips Incorporating these aspects into your documentation will result in an accurate picture in the patient’s severity of illness and risk of mortality • Use adjectives (acute, chronic, acute-on-chronic, mild, moderate, severe, persistent) • Indicate cause and effect (due to or secondary to) • Be specific about the aspects of the disease (use current terminology) • Specify the anatomical site • Use exact dates Copyright c 2015 Confidential and Proprietary Information Clear Clinical Documentation Avoid using “history of” when documenting a current, chronic condition; in coding “history of” means the patient no longer has the condition Copyright © 2015 Confidential and Proprietary Information Put M.E.A.T. in Documentation for Healthy Audits • Problem lists must show evaluation and treatment for each condition that relates to a diagnosis code • Monitor -signs, symptoms, disease progression, disease regression • Evaluate - test results, medication effectiveness, response to treatment • Address - ordering tests, discussion, review records, counseling • Treat - medications, therapies, other modalities Copyright © 2015 Confidential and Proprietary Information Ordering Diagnostic/Therapeutic Services • Governmental and third party payers require the performing provider (hospital ancillary departments, outpatient freestanding centers, independent labs, etc.) to provide ICD9/10 codes for outpatient diagnostic and/or therapeutic testing/services that they perform and submit for payment on behalf of your patients • These providers rely on you, the ordering physician, to submit the appropriate diagnosis code at the time of ordering to establish medical necessity for the test ordered Copyright © 2015 Confidential and Proprietary Information CMS FAQ 7579 – Refills (Medicaid Requirement) • If a payer/pharmacy requires a diagnosis code for a prescription and the prescriber reports an ICD-9 diagnosis code because it is prescribed prior to the October 1, 2015 ICD-10 implementation date, what diagnosis code must be reported if that same prescription is filled and processed after the October 1, 2015 ICD-10 implementation date? • When conducting a standard transaction, medical data code sets (ICD-9 and ICD-10) that are valid at the time that the service is provided (prescription fill date) must be used (45 CFR 162.1000).For example: A prescription, reporting an ICD9 diagnosis code, is dated 09/20/2015. The prescription is filled and processed by the pharmacy on 10/02/2015. CMS FAQ 7579 - Refills • The Date of Service reported by the pharmacy on the claim is 10/02/2015 (even though the prescription was written 09/20/2015). • The claim, when submitted on 10/02/2015, is required to report an ICD-10 diagnosis code. A prescription, reporting an ICD-9 diagnosis code, is dated 08/01/2015. CMS FAQ 7579 - Refills • Refills for the prescription occur monthly and four refills are allowed. The prescription is filled and processed by the pharmacy 08/01/2015. An ICD-9 code is reported, if a diagnosis code is required. • The same prescription is refilled and processed by the pharmacy on 09/01/2015. An ICD-9 is reported. • The same prescription is refilled and processed by the pharmacy on 10/01/2015. An ICD-10 code must now be reported. • The same prescription is refilled and processed by the pharmacy 11/01/2015. An ICD-10 code must be reported. • The refill date of service is the date that the prescription is filled and processed, not the date the prescription was written. This is especially relevant for prescriptions that may be scheduled for automatic refills. ICD-10 Specialty Specific Diagnoses • The diagnoses reviewed today are not all-inclusive, but serve as a guide to improving clinical documentation, correct coding with ICD-10 and capturing severity, acuity, and risk of mortality for the patients you serve • The diagnoses listed are top ICD-9 diagnosis codes obtained from the Network that providers are using today. The mappings are a result of current code/documentation. In order to capture the greatest level of specificity, compare your current documentation with code options in the coding manual to determine opportunities for documentation improvement. Copyright c 2015 Confidential and Proprietary Information Some ICD-10 Areas That Require Attention • • • • • • • Site (upper, mid, lower), especially neoplasms Laterality (right, left, bilateral) Severity (acute, chronic, acute-on-chronic) Cause (etiology, manifestation, complications, organisms) Acquired vs. congenital conditions Diagnosis not addressed in note Diagnosis missing clinical detail such as type of disease/injury • Pathology or radiographic findings not documented by attending provider • Stage (CKD or pressure ulcer) Copyright c 2015 Confidential and Proprietary Information Suture Removal ICD-9-CM ICD-10-CM V58.32 Encounter for removal of sutures Z48.02 Encounter for removal of sutures Copyright c 2015 Confidential and Proprietary Information Dysphagia ICD-9-CM ICD-10-CM 787.20 Dysphagia, unspecified R13.10 Dysphagia, unspecified ** There are more specific code choice selections available in ICD-10-CM. These include: R13.11 Dysphagia, oral phase R13.12 Dysphagia, oropharyngeal phase R13.13 Dysphagia, pharyngeal phase R13.14 Dysphagia, pharyngoesophageal phase R13.19 Other dysphagia Copyright c 2015 Confidential and Proprietary Information Clinical Documentation Awareness Tips Gastrointestinal Documentation Awareness Fever •Document the cause if known e.g. drug induced, post procedural Diarrhea has many combination codes in ICD-10 where it is included as a manifestation • Document the cause e.g. Infectious, postgastrectomy, toxic, allergic, drug-induced, etc Clinical Documentation Awareness Tips Gastrointestinal Coding Awareness Etiology if known to identify condition to code in lieu of the sign/symptom of abdominal pain. Laterality e.g. left, right Anatomical location e.g. upper, lower, epigastric, etc. Gastrointestinal ICD-9-CM ICD-10-CM 787.01 Nausea & Vomiting R11.2 Nausea with vomiting, unspecified 787.02 Nausea alone R11.0 Nausea 787.03 Vomiting alone R11.11 Vomiting without nausea R11.12 Projectile vomiting R11.13 Vomiting of fecal matter R11.14 Bilious vomiting 564.00 Constipation K59.00 Constipation, unspecified K59.01 Slow transit constipation K59.02 Outlet dysfunction constipation K59.09 Other constipation 787.91 Diarrhea R19.7 Diarrhea NOS K59.1 Functional diarrhea Barrett’s Esophagus ICD-9-CM ICD-10-CM 530.85 Barrett's esophagus K22.70 Barrett’s esophagus without dysplasia K22.710 Barrett’s esophagus with low grade dysplasia K22.711 Barrett’s esophagus with high grade dysplasia K22.719 Barrett’s esophagus with dysplasia, unspecified Copyright c 2015 Confidential and Proprietary Information CA Esophagus ICD-9-CM ICD-10-CM 150.9 Malignant neoplasm of esophagus, unspecified site C15.9 Malignant neoplasm of esophagus, unspecified * Use additional code to identify: • alcohol abuse or dependence (F10.-) Copyright © 2015 MEDKODER LLC Confidential and Proprietary Information 61 GERD ICD-9-CM ICD-10-CM 530.81 Esophageal reflux K21.0 Gastro-esophageal reflux disease with esophagitis K21.9 Gastro-esophageal reflux disease without esophagitis Copyright c 2015 Confidential and Proprietary Information Anemia Anemia Documentation Awareness • Documentation of Anemia should include the type of anemia: -- Nutritional -- Hemolytic -- Aplastic -- Due to blood loss -- Other (please specify) • Include in documentation if Anemia is due to nutrition or mineral deficits, resulting in a nutritional anemia • Document if the Anemia is due to a neoplasm (primary and/or secondary) • Document whether the ANEMIA is “related to or due to” chemo or radiotherapy treatments • Document any “cause–and-effect” relationship between the intervention and the blood or immune disorder • Document the specific drug if anemia is drug-induced • Link any laboratory findings to a related diagnosis (if appropriate) • Document any associated diagnoses/conditions Copyright © 2015 MEDKODER LLC Confidential and Proprietary Information 63 Anemia ICD-9-CM ICD-10-CM 285.9 Anemia, unspecified D64.9 *Anemia, unspecified *There are more specific code choice selections available in ICD-10-CM. These include: D64.81 Anemia due to antineoplastic chemotherapy D63.0 Anemia in neoplastic disease D61.1 Aplastic anemia due to antineoplastic chemotherapy Copyright © 2015 MEDKODER LLC Confidential and Proprietary Information 64 Autoimmune Hemolytic Anemias ICD-9-CM ICD-10-CM 283.0 Autoimmune hemolytic anemias D59.0 Drug-induced autoimmune hemolytic anemia D59.1 Other autoimmune hemolytic anemias * Use additional code for adverse effect, if applicable, to identify drug (T36-T50 with fifth or sixth character 5) Copyright © 2015 MEDKODER LLC Confidential and Proprietary Information 65 Abdominal Pain ICD-9-CM ICD-10-CM 789.00 Abdominal pain, unspecified R10.0 Acute abdomen R10.10 Upper abdominal pain, unspecified R10.11 Right upper quadrant pain R10.12 Left upper quadrant pain R10.13 Epigastric pain R10.2 Pelvic and perineal pain R10.30 Lower abdominal pain, unspecified R10.31 Right lower quadrant pain R10.32 Left lower quadrant pain R10.33 Periumbilical pain R10.84 Generalized abdominal pain R10.9 Unspecified abdominal pain Copyright c 2015 Confidential and Proprietary Information Anal Fissure ICD-9-CM ICD-10-CM 565.0 Anal fissure K60.0 Acute anal fissure K60.1 Chronic anal fissure K60.2 Anal fissure, unspecified Copyright c 2015 Confidential and Proprietary Information Clinical Documentation Awareness Tips Enteritis / Crohn’s Documentation Awareness Site: e.g. small, large, both With complication: e.g. abscess, fistula, intestinal obstruction, rectal bleeding Enteritis / Crohn’s Disease ICD-9-CM ICD-10-CM 555.9 Regional enteritis of unspecified site K50.90 Crohn’s disease, unspecified, without complications ** Use additional code to identify manifestations, such as: pyoderma gangrenosum (L88) * There are more specific code choice selections available in ICD-10-CM. These include: K50.00 Crohn’s disease of small intestine without complications Copyright c 2015 Confidential and Proprietary Information Crohn’s Disease ICD-9-CM ICD-10-CM K50.011 Crohn’s disease of small intestine with rectal bleeding K50.012 Crohn’s disease of small intestine with intestinal obstruction K50.013 Crohn’s disease of small intestine with fistula K50.014 Crohn’s disease of small intestine with abscess K50.018 Crohn’s disease of small intestine with other complication K50.019 Crohn’s disease of small intestine with unspecified complications Copyright c 2015 Confidential and Proprietary Information Crohn’s Disease ICD-9-CM ICD-10-CM K50.10 Crohn’s disease of large intestine without complications K50.111 Crohn’s disease of large intestine with rectal bleeding K50.112 Crohn’s disease of large intestine with intestinal obstruction K50.113 Crohn’s disease of large intestine with fistula K50.114 Crohn’s disease of large intestine with abscess K50.118 Crohn’s disease of large intestine with other complication Copyright c 2015 Confidential and Proprietary Information Crohn’s Disease ICD-9-CM ICD-10-CM K50.119 Crohn’s disease of large intestine with unspecified complications K50.80 Crohn’s disease of both small and large intestine without complications K50.811 Crohn’s disease of both small and large intestine with rectal bleeding K50.812 Crohn’s disease of both small and large intestine with intestinal obstruction K50.813 Crohn’s disease of both small and large intestine with fistula K50.814 Crohn’s disease of both small and large intestine with abscess Copyright c 2015 Confidential and Proprietary Information Crohn’s Disease ICD-9-CM ICD-10-CM K50.818 Crohn’s disease of both small and large intestine with other complication K50.819 Crohn’s disease of both small and large intestine with unspecified complications K50.911 Crohn’s disease, unspecified, with rectal bleeding K50.912 Crohn’s disease, unspecified, with intestinal obstruction K50.913 Crohn’s disease, unspecified, with fistula K50.914 Crohn’s disease, unspecified, with abscess K50.918 Crohn’s disease, unspecified, with other complication K50.919 Crohn’s disease, unspecified, with unspecified complications Diabetes Mellitus ICD-9-CM ICD-10-CM Type • Type I • Type 2 • Secondary diabetes mellitus Type • Type 1 • Type 2 • Drug/chemical induced • Due to underlying condition • Specified Type Control • Controlled • Uncontrolled Control • Inadequately controlled • Out of control • Poorly controlled • Hypoglycemia • Hyperglycemia Manifestation/Complication • Hyperosmolarity • Ketoacidosis • Neurological manifestations • Other coma • Peripheral circulatory disorder • Renal Manifestations • Other specified manifestations • Without Complications Manifestation/Complication • Arthropathy • Circulatory complications • Hyperosmolarity • Hypoglycemia • Ketoacidosis • Kidney complications • Neurological complications • Ophthalmic complications • Oral complications • Skin complications • Without complications Insulin Use Insulin Use • No longer required for Type 1 • For Type 2 any long-term or current use is reported 74 Diabetes Mellitus ICD-9-CM Code ICD-10-CM Code(s) 250.00 – Diabetes mellitus without mention of complications type II or unspecified type, not states as controlled E11.9 – Type 2 diabetes mellitus without complications Diabetes Mellitus Documentation Awareness Capturing the correct code for Diabetes Mellitus requires clear and precise documentation of the underlying cause. Diabetes mellitus codes in ICD-10 reflect combination codes. The components of the combination codes are: • Type of Diabetes • Body System Affected • Specified complications/manifestations affecting the body system 75 Diabetes Mellitus Documentation Awareness Type of Diabetes • Drug or Chemical Induced (E09) – (anticonvulsants; antihypertensive drugs including diuretics and beta blockers; antipsychotic drugs including lithium and antidepressants; antiretroviral drugs; chemotherapy drugs; hormone supplements including anabolic steroids, contraceptives, estrogen, growth hormones and hormones for prostate cancer) • Due to an underlying condition (E08) • Type I diabetes (E10) – controlled/not specified; uncontrolled • Type 2 diabetes (E11) – controlled/not specified; uncontrolled • Other specified diabetes (E13) – secondary diabetes mellitus – controlled/not specified; uncontrolled For Type 2 diabetes mellitus and secondary diabetes mellitus, any long-term or current use of insulin is reported as an additional code. You may report more than one diabetes code for patients with multiple complications or when multiple body systems are affected as a result of the diabetes. Secondary diabetes is defined as a diabetic condition with an underlying cause other than genetics or environmental conditions (includes due to drugs, chemicals, medical conditions, surgical procedures or trauma) 76 Diabetes Diabetes Mellitus Documentation Awareness Body System Affected • Circulatory complications • Hyperosmolarity • Kidney complications • Ketoacidosis • Other coma • Neurological complications • Ophthalmic complications • Other specified complications/manifestations • Unspecified complications/manifestations • Without complications/manifestations 77 Diabetes Mellitus Documentation Awareness Specified complications/manifestations affecting the body system • • • • • • • • • • Circulatory complications – peripheral Hyperosmolarity Hypoglycemia (with or without coma) Kidney complications – diabetic nephropathy; chronic kidney disease; other Ketoacidosis – with or without coma Neurological complications – amyotrophy; autonomic polyneuropathy; mononeuropathy, polyneuropathy; other; unspecified Ophthalmic complications – diabetic retinopathy (mild, moderate or severe nonproliferative with or without macular edema); diabetic cataract; other Other specified complications/manifestations – skin complications (dermatitis, foot ulcer; other skin ulcer; other skin complications; oral complications (periodontal disease; other) Unspecified complications/manifestations Without complications/manifestations 78 Clinical Documentation Awareness Tips Hypertension Documentation Awareness Type: e.g. essential or secondary Causal relationship: e.g. relationship between hypertension and renals, pulmonary, heart • Note: The Hypertension Table in ICD-10-CM has been eliminated. The same code is used regardless of whether the hypertension is described as benign, malignant or whether or not a qualifier is used Hypertension ICD-9-CM 401.0 Malignant HTN 401.1 Benign HTN 401.9 Unspecified ICD-10-CM I10 Essential (primary) hypertension 80 Cleft Palate ICD-9-CM ICD-10-CM 749.00 Cleft palate unspecified 749.01 Cleft palate, unilateral, complete 749.02 Cleft palate, unilateral, incomplete 749.03 Cleft palate, bilateral, complete 749.04 Cleft palate, bilateral, incomplete 749.20 Cleft palate with cleft lip, unspecified Q35 Cleft palate Q35.1 Cleft hard palate Q35.3 Cleft soft palate Q35.5 Cleft hard palate with cleft soft palate Q35.7 Cleft uvula Q35.9 Cleft palate, unspecified Q36 Cleft lip Q36.0 Cleft lip, bilateral Q36.1 Cleft lip, median Q36.9 Cleft lip, unilateral Q37 Cleft palate with cleft lip Copyright c 2015 Confidential and Proprietary Information Cleft Palate ICD-9-CM ICD-10-CM Q37.0 Cleft hard palate with bilateral cleft lip Q37.1 Cleft hard palate with unilateral cleft lip Q37.2 Cleft soft palate with bilateral cleft lip Q37.3 Cleft soft palate with unilateral cleft lip Q37.4 Cleft hard and soft palate with bilateral cleft lip Q37.5 Cleft hard and soft palate with unilateral cleft lip Q37.8 Unspecified cleft palate with bilateral cleft lip Q37.9 Unspecified cleft palate with unilateral cleft lip Documentation Awareness Tips Fracture Documentation Awareness Type: e.g. open, closed, stress, pathologic, etc. Anatomical location: e.g. nasal, distal, proximal, index, ring, etc. Laterality e.g. left, right, bilateral Site: e.g. distal pole, middle third, body, hook process, larger/smaller multangular, neck, shaft, base, etc. Healing status: e.g. malunion, nonunion, delayed healing, etc. Encounter of care: e.g. initial, subsequent, sequelae Alignment: e.g. displaced, non displaced Classification: e.g. Bennett’s, Rolando’s, etc. Etiology: e.g. traumatic, pathologic (age, osteopenia) Encounter of care • An initial encounter is used when the patient is receiving active treatment (surgical treatment, ER encounter, evaluation by a new physician) • A subsequent encounter is used once active treatment has been completed and is receiving care during the recovery phase. (cast change, cast removal, medication adjustment, removal of a fixation device, follow-up visits after fracture treatment) Documentation Awareness Tips 7th digit for injury section – Fx nasal bones Category S02, S12, S22, S32, S92, A Initial encounter for closed fracture B Initial encounter for open fracture D Subsequent encounter for fracture with routine healing G Subsequent encounter for fracture with delayed healing K Subsequent encounter for fracture with nonunion S Sequela Fracture Nasal Bones ICD-9-CM ICD-10-CM 802.0 Fracture of nasal bones, closed S02.2xxA Fracture of nasal bones, initial encounter for closed fracture S02.2xxD Fracture of nasal bones, subsequent encounter for fracture with routine healing S02.2xxG Fracture of nasal bones, subsequent encounter for fracture with delayed healing S02.2xxK Fracture of nasal bones, subsequent encounter for fracture with nonunion S02.2xxS Fracture of nasal bones, sequela Copyright c 2015 Confidential and Proprietary Information Gallstones ICD-9-CM ICD-10-CM 574.20 Calculus of gallbladder without K80.20 Calculus of gallbladder without mention of cholecystitis, without mention cholecystitis without obstruction of obstruction Copyright c 2015 Confidential and Proprietary Information Inguinal hernia ICD-9-CM ICD-10-CM 550.90 Inguinal hernia, without mention of obstruction or gangrene, unilateral or unspecified (not specified as recurrent) K40.90 Unilateral inguinal hernia, without obstruction or gangrene, not specified as recurrent Copyright c 2015 Confidential and Proprietary Information Sinusitis ICD-9-CM ICD-10-CM 473.9 Unspecified sinusitis (chronic) J32.9 Chronic sinusitis, unspecified • Use additional code to identify: Exposure to environmental tobacco smoke (Z77.22) • Exposure to tobacco smoke in the perinatal period (P96.81) • History of tobacco use (Z87.891) • Occupational exposure to environmental tobacco smoke (Z57.31) Tobacco dependence (F17-) • Tobacco use (Z72.0) Copyright c 2015 Confidential and Proprietary Information Sinusitis ICD-9-CM ICD-10-CM ** There are more specific code choice selections available in ICD-10-CM. These include: J32.0 Chronic maxillary sinusitis J32.1 Chronic frontal sinusitis J32.2 Chronic ethmoidal sinusitis J32.3 Chronic sphenoidal sinusitis J32.4 Chronic pansinusitis J32.8 Other chronic sinusitis Copyright c 2015 Confidential and Proprietary Information Tobacco Abuse/Dependence ICD-9-CM 305.1 Tobacco abuse/dependence ICD-10-CM F17.211 Nicotine dependence , cigarettes, in remission F17.213 Nicotine dependence, cigarettes, with withdrawal F17.218 Nicotine dependence, cigarettes, with other nicotineinduced disorders F17.221 Nicotine dependence , chewing tobacco, in remission F17.223 Nicotine dependence, chewing tobacco, with withdrawal F17.228 Nicotine dependence, chewing tobacco, with other nicotine-induced disorders Z72.0 Tobacco use Chronic Tonsillitis ICD-9-CM ICD-10-CM 474.00 Chronic tonsillitis J35.01 Chronic tonsillitis • Use additional code to identify: Exposure to environmental tobacco smoke (Z77.22) • Exposure to tobacco smoke in the perinatal period (P96.81) • History of tobacco use (Z87.891) Occupational exposure to environmental tobacco smoke • (Z57.31) • Tobacco dependence (F17-) • Tobacco use (Z72.0) Copyright c 2015 Confidential and Proprietary Information Morbid Obesity ICD-9-CM ICD-10-CM 278.01 Morbid obesity E66.01 Morbid (severe) obesity due to excess calories * Code first obesity complicating pregnancy, childbirth and the puerperium, if applicable (O99.21-) **Use additional code to identify body mass index (BMI), if known (Z68-) Copyright c 2015 Confidential and Proprietary Information Intensive Behavioral Therapy (IBT) for Obesity Body Mass Index (BMI), Adult ICD-9-CM ICD-10-CM V85.30 BMI 30.0-30.9, adult Z68.30 BMI 30.0-30.9, adult V85.31 BMI 31.0-31.9, adult Z68.31BMI 31.0-31.9, adult V85.32 BMI 32.0-32.9, adult Z68.32 BMI 32.0-32.9, adult V85.33 BMI 33.0-33.9, adult Z68.33 BMI 33.0-33.9, adult V85.34 BMI 34.0-34.9, adult Z68.34 BMI 34.0-34.9, adult V85.35 BMI 35.0-35.9, adult Z68.35 BMI 35.0-35.9, adult V85.36 BMI 36.0-36.9, adult Z68.36 BMI 36.0-36.9, adult V85.37 BMI 37.0-37.9, adult Z68.37 BMI 37.0-37.9, adult V85.38 BMI 38.0-38.9, adult Z68.38 BMI 38.0-38.9, adult V85.39 BMI 39.0-39.9, adult Z68.39 BMI 39.0-39.9, adult Body Mass Index (BMI), Adult ICD-9-CM ICD-10-CM V85.41 BMI 40.0-44.9, adult Z68.41BMI 40.0-44.9, adult V85.42 BMI 45.0-49.9, adult Z68.42 BMI 45.0-49.9, adult V85.43 BMI 50.0-59.9, adult Z68.43 BMI 50.0-59.9, adult V85.44 BMI 60.0-69.9, adult Z68.44 BMI 60.0-69.9, adult V85.45 BMI 70 and over, adult Z68.45 BMI 70 and over, adult Chronic Suppurative Otitis Media ICD-9-CM ICD-10-CM 382.3 Unspecified chronic suppurative otitis media H66.3x1 Other chronic suppurative otitis media, right ear H66.3x2 Other chronic suppurative otitis media, left ear H66.3x3 Other chronic suppurative otitis media, bilateral H66.3x9 Other chronic suppurative otitis media, unspecified ear *Use additional code for any associated perforated tympanic membrane (H72-) Copyright c 2015 Confidential and Proprietary Information Chronic Suppurative Otitis Media ICD-9-CM ICD-10-CM • Use additional code to identify: Exposure to environmental tobacco smoke (Z77.22) • Exposure to tobacco smoke in the perinatal period (P96.81) • History of tobacco use (Z87.891) • Occupational exposure to environmental tobacco smoke (Z57.31) Tobacco dependence (F17-) • Tobacco use (Z72.0) Copyright c 2015 Confidential and Proprietary Information Perforation of Tympanic Membrane ICD-9-CM ICD-10-CM 384.20 Perforation of tympanic membrane, unspecified H72.90 Unspecified perforation of tympanic membrane, unspecified ear ** Code first any associated otitis media (H65-, H66.1-, H66.2-, H66.3-, H66.4-, H66.9-, H67-) H72.91 Unspecified perforation of tympanic membrane, right ear H72.92 Unspecified perforation of tympanic membrane, left ear H72.93 Unspecified perforation of tympanic membrane, bilateral Copyright c 2015 Confidential and Proprietary Information Perforation of Tympanic Membrane ICD-9-CM ICD-10-CM ** There are more specific code choice selections available in ICD-10-CM. These include: H72.00 Central perforation of tympanic membrane, unspecified ear H72.01 Central perforation of tympanic membrane, right ear H72.02 Central perforation of tympanic membrane, left ear H72.03 Central perforation of tympanic membrane, bilateral H72.10 Attic perforation of tympanic membrane, unspecified ear H72.11 Attic perforation of tympanic membrane, right ear Copyright c 2015 Confidential and Proprietary Information Perforation of Tympanic Membrane ICD-9-CM ICD-10-CM H72.12 Attic perforation of tympanic membrane, left ear H72.13 Attic perforation of tympanic membrane, bilateral H72.2x1 Other marginal perforations of tympanic membrane, right ear H72.2x2 Other marginal perforations of tympanic membrane, left ear H72.2x3 Other marginal perforations of tympanic membrane, bilateral H72.2x9 Other marginal perforations of tympanic membrane, unspecified ear Copyright c 2015 Confidential and Proprietary Information Perforation of Tympanic Membrane ICD-9-CM ICD-10-CM H72.811 Multiple perforations of tympanic membrane, right ear H72.812 Multiple perforations of tympanic membrane, left ear H72.813 Multiple perforations of tympanic membrane, bilateral H72.819 Multiple perforations of tympanic membrane, unspecified ear H72.821 Total perforations of tympanic membrane, right ear H72.822 Total perforations of tympanic membrane, left ear H72.823 Total perforations of tympanic membrane, bilateral H72.829 Total perforations of tympanic membrane, unspecified ear Screening Codes • Documentation for screenings must include any abnormal finding which would be listed secondary to the screening codes • Screening codes in ICD-10 can be broken down by the condition, procedure, or anatomic location depending on the type of screening Copyright © 2015 MEDKODER LLC Confidential and Proprietary Information 101 Screening ICD-9-CM ICD-10-CM V76.2 Special screening examination for malignant neoplasm of cervix Z12.4 Encounter for screening malignant neoplasm of cervix V74.5 Screening examination for venereal disease Z11.3 Screening examination for venereal disease V76.44 Special screening for malignant neoplasm of prostate Z12.5 Encounter for screening malignant neoplasm of prostate V76.51 Special screening for malignant neoplasms of colon Z12.11 Encounter for screening malignant neoplasm of colon V72.84 Preoperative examination, unspecified Z01.812 Encounter for preprocedural laboratory examination Z01.818 Encounter for other preprocedural examination V77.91 Screening for lipoid disorders Z13.220 Encounter for screening for lipoid disorders V73.81 Special screening for HPV Z11.51 Encounter for screening for HPV History of Colon Polyps ICD-9-CM ICD-10-CM V10.05 Personal history of malignant neoplasm of large intestine Z85.038 Personal history of other malignant neoplasm of large intestine Z85.030 Personal history of malignant carcinoid tumor of large intestine Copyright c 2015 Confidential and Proprietary Information Table of Neoplasms Copyright © 2015 MEDKODER LLC Confidential and Proprietary Information Unspecified Behavior Uncertain Benign CA in-situ Malignant Secondary Neoplasm, neoplastic Malignant Primary • The Neoplasm Table is formatted similarly to the table in ICD-9-CM and contains the same Headings 104 Neoplasm Documentation Neoplasm Documentation Awareness Documentation should include: • Behavior - Malignant (primary, secondary, in-situ) Document any secondary sites - Benign - Unspecified behavior - Of certain histological behavior • Laterality (right/left) • Anatomical site (topography) • Other condition(s) associated with malignancy – (dehydration, anemia, etc.) • Complication(s) associated with neoplasm • Include estrogen receptor status (if applicable) • History of: - Has the malignancy been excised or eradicated? - Is there still treatment being provided for the primary and/or secondary site? - Is there evidence of remaining malignancy at the primary site? • Document any associated diagnoses/conditions Copyright © 2015 MEDKODER LLC Confidential and Proprietary Information 105 Neoplasms • Overlapping sites • Laterality – Left vs. Right • C50.2 Malignant neoplasm, of upper-inner quadrant of breast) – C50.21 Malignant neoplasm of upper-inner quadrant of breast, female • C50.211 Malignant neoplasm of upper-inner quadrant of right female breast • C50.212 Malignant neoplasm of upper-inner quadrant of left female breast • C50.219 Malignant neoplasm of upper-inner quadrant of unspecified female breast Copyright © 2015 MEDKODER LLC Confidential and Proprietary Information 106 CA of Breast ICD-9-CM ICD-10-CM 174.9 Malignant neoplasm of breast (female, unspecified) C50.919 Malignant neoplasm of unspecified site of unspecified female breast * Use additional code to identify estrogen receptor status (Z17.0, Z17.1) Copyright © 2015 MEDKODER LLC Confidential and Proprietary Information 107 Postmastectomy Lymphedema Syndrome ICD-9-CM ICD-10-CM 457.0 Postmastectomy lymphedema syndrome I97.2 Postmastectomy lymphedema syndrome Copyright © 2015 MEDKODER LLC Confidential and Proprietary Information 108 Breast Implants • Breast implants without complications – Z98.82 • If the patient previously had breast implants but they have been removed – Z98.86 (Hx breast implant removal) • Complications from breast implants (e.g. rupture of breast implant) – T85.49xA – The only code reported is the complication code Copyright c 2015 Confidential and Proprietary Information Cosmetic Plastic Surgery, Other (Breast Augmentation, Face Lift, etc.) ICD-9-CM ICD-10-CM Z41.1: Encounter for cosmetic surgery Z41.2: Encounter for routine and ritual male circumcision Z41.3: Encounter for ear piercing Z41.8: Encounter for other procedures for purposes other than remedying health state Z41.9: Encounter for procedure for purposes other than remedying health state, unspecified Copyright c 2015 Confidential and Proprietary Information Swelling, Mass or Lump in Head and Neck ICD-9-CM ICD-10-CM 784.2 Swelling, mass, or lump in head and R22.0 Localized swelling, mass and lump, neck head R22.1 Localized swelling, mass and lump, neck Copyright c 2015 Confidential and Proprietary Information Benign Neoplasm of Colon ICD-9-CM ICD-10-CM 211.3 Benign neoplasm of colon D12.0 Benign neoplasm of cecum D12.1 Benign neoplasm of appendix D12.2 Benign neoplasm of ascending colon D12.3 Benign neoplasm of transverse colon D12.4 Benign neoplasm of descending colon D12.5 Benign neoplasm of sigmoid colon D12.6 Benign neoplasm of colon, unspecified D12.7 Benign neoplasm of rectosigmoid junction K63.5 Polyp of colon Copyright c 2015 Confidential and Proprietary Information CA of Colon ICD-9-CM ICD-10-CM 153.9 Malignant neoplasm of colon, unspecified site C18.9 Malignant neoplasm of colon, unspecified Copyright © 2015 MEDKODER LLC Confidential and Proprietary Information 113 CA of Rectum ICD-9-CM ICD-10-CM 154.1 Malignant neoplasm of rectum C20 Malignant neoplasm of rectum Copyright © 2015 MEDKODER LLC Confidential and Proprietary Information 114 CA Pancreas ICD-9-CM ICD-10-CM 157.9 Malignant neoplasm of pancreas, part unspecified C25.9 Malignant neoplasm of pancreas, unspecified * Use additional code to identify: • alcohol use and dependence (F10.-) Copyright © 2015 MEDKODER LLC Confidential and Proprietary Information 115 Benign Neoplasm of the Colon ICD-9-CM ICD-10-CM 211.3 Benign neoplasm colon D12.6 Benign neoplasm of colon, unspecified • There are more specific code choice selections available in ICD-10-CM. • These include: D12.0 Benign neoplasm of cecum D12.1 Benign neoplasm of appendix D12.2 Benign neoplasm of ascending colon D12.3 Benign neoplasm of transverse colon D12.4 Benign neoplasm of descending colon D12.5 Benign neoplasm of sigmoid colon Copyright c 2015 Confidential and Proprietary Information Vocal Cord Polyp 478.4 Polyp of vocal cord or larynx J38.1 Polyp of vocal cord and larynx * Use additional code to identify: Exposure to environmental tobacco smoke (Z77.22) Exposure to tobacco smoke in the perinatal period (P96.81) History of tobacco use (Z87.891) Occupational exposure to environmental tobacco smoke (Z57.31) Tobacco dependence (F17-) Tobacco use (Z72.0) Copyright c 2015 Confidential and Proprietary Information GI Bleeding ICD-9-CM ICD-10-CM 578.9 Hemorrhage of gastrointestinal tract, unspecified K92.2 Gastrointestinal hemorrhage, unspecified Copyright c 2015 Confidential and Proprietary Information Diverticular Disease ICD-9-CM ICD-10-CM 562.10 Diverticulosis of colon (without hemorrhage) 562.11 Diverticulitis of colon without mention of hemorrhage K57.30 Diverticulosis of large intestine without perforation or abscess without bleeding K57.32 Diverticulitis of large intestine without perforation or abscess without bleeding K57.20 Diverticulitis of large intestine with perforation and abscess without bleeding Copyright c 2015 Confidential and Proprietary Information Urosepsis • Urosepsis will not be considered synonymous with sepsis. It has no default code in the Alphabetic Index. • Should a Provider use this term he/she must be queried for clarification Copyright c 2015 Confidential and Proprietary Information Urinary Tract Infection ICD-9-CM ICD-10-CM 599.0 Urinary Tract Infection, unspecified N39.0 Urinary Tract Infection, site not specified *Use additional code to identify infectious agent (B95-B97) **There are more specific code choice selections available in ICD-10-CM These include: N30.00 Acute cystitis without hematuria N30.01 Acute cystitis with hematuria N30.10 Interstitial cystitis chronic without hematuria N30.11 Interstitial cystitis chronic with hematuria N30.20 Other chronic cystitis without hematuria N30.21 Other chronic cystitis with hematuria Urinary Tract Infection ICD-9-CM ICD-10-CM N30.30 Trigonitis without hematuria N30.31 Trigonitis with hematuria N30.40 Irradiation cystitis without hematuria N30.41 Irradiation cystitis with hematuria N30.80 Other cystitis without hematuria N30.81 Other cystitis with hematuria N30.90 Cystitis, unspecified without hematuria N30.91 Cystitis, unspecified with hematuria N15.9 Renal tubulo-interstitial disease, unspecified N34.1 Nonspecific urethritis N34.2 Other urethritis 122 Sepsis Clinical Documentation Awareness In ICD-10, there will no longer be a designation for “septicemia”; bacteremia (R78.81) or bacterial sepsis will be preferred. Specify whether bacteremia is due to septic condition in the body or is transient due to a procedure or unknown cause Sepsis documentation should include: • the source of the infection if known • the patient’s signs and symptoms of sepsis • the presence of organ failure (renal, respiratory hepatic, etc.) related to sepsis • whether positive blood cultures are clinically significant or contaminates • other factors such as immunocompromise (diabetes, steroid therapy, malnutrition, immunoglobulin deficiency, chemotherapy) • the likely relationship to implanted devices Copyright c 2015 Confidential and Proprietary Information Sepsis ICD-9-CM ICD-10-CM 995.91 Sepsis A41.9 Sepsis, unspecified organism Copyright c 2015 Confidential and Proprietary Information HIV Source: www.cdc.gov/nchs/icd/icd10cm.htm Topic ICD-10-CM Code Ranges Documentation Tips/Guidelines HIV HIV Asymptomatic AIDS Z21 – HIV currently asymptomatic B20 - AIDS Code only confirmed cases Confirmation does not require positive serology or culture for HIV-only; requires physician statement NOTE: Inpatient hospital guidelines are different. Known HIV or HIV-positive should be clearly documented. If patient admitted for HIVrelated disease or AIDS, first listed diagnosis is B20, then the additional codes for the related condition 125 Copyright © 2015 MEDKODER LLC Confidential and Proprietary Information Infectious Diseases Source: www.cdc.gov/nchs/icd/icd10cm.htm Topic ICD-10-CM Code Ranges Documentation Tips/Guidelines Infections Resistant to Antibiotics Z16 Resistance to antimicrobial drug Specify which antibiotic the organism is resistant to in the medical record MRSA Conditions MRSA Carrier/Colonization MRSA Susceptible/Colonization Usually appears as combination code that has the disease and causal organism together Z2.322 Carrier or suspected carrier of MRSA Z22321 Carrier or suspected carrier of methicillin susceptible Z22.321 MRSA susceptible with colonization Example: Pneumonia due to MRSA is code J15.212 . Do not use additional code for resistance to Penicillin, Z16.11. If a current infection does not have a combination code for MRSA, use the code to identify the condition and use B95.62 for MRSA organism Document carrier or 126 susceptibility to MRSA Copyright © 2015 MEDKODER LLC Confidential and Proprietary Information Asceptic Necrosis Source: www.cdc.gov/nchs/icd/icd10cm.htm Topic ICD-10-CM Code Range Documentation Tips/Guidelines Asceptic Necrosis M87.00 – M90.59 Specify in documentation whether due to drugs, trauma, idiopathic, asceptic necrosis or secondary osteonecrosis. Specify exact anatomic site as well as laterality (left or right). Copyright © 2015 MEDKODER LLC Confidential and Proprietary Information 127 Cellulitis Source: www.cdc.gov/nchs/icd/icd10cm.htm Topic ICD-10-CM Code Ranges Cellulitis Carbuncle/Furuncle L02.02 – L02.03 Cellulitis/Abscess/Onchyia/ L02.02 – L03.91 Paronychia Copyright © 2015 MEDKODER LLC Confidential and Proprietary Information Documentation Tips/Guidelines Specify carbuncle/furuncle and provide exact site location. Document specific body part, cellulitis, abscess, lymphangitis as appropriate Document right or left as appropriate 128 Carotid Artery Stenosis ICD-9-CM Icd-10-CM 433.10 Occlusion and stenosis of carotid artery without mention of cerebral infarction I65.21 Occlusion and stenosis of right carotid artery I65.22 Occlusion and stenosis of left carotid artery I65.23 Occlusion and stenosis of bilateral carotid arteries I65.29 Occlusion and stenosis of unspecified carotid artery Copyright c 2015 Confidential and Proprietary Information Chronic Pain 338.21 Chronic pain due to trauma G89.21 Chronic pain due to trauma ** Code also related psychological factors associated with pain (F45.42) 338.28 Other chronic postoperative pain G89.28 Other chronic postprocedural pain ** Code also related psychological factors associated with pain (F45.42) 338.4 Chronic pain syndrome G89.4 Chronic pain syndrome ** Code also related psychological factors associated with pain (G54.42-) Copyright © 2015 Confidential and Proprietary Information Peripheral Vascular Disease ICD-9-CM ICD-10-CM 443.9 Peripheral vascular disease, unspecified I73.9 Peripheral vascular disease, unspecified ** There are more specific code choice selections available. These include: I73.00 Raynaud’s syndrome without gangrene I73.01 Raynaud’s syndrome with gangrene I73.1 Thromboangiitis obliterans (Buerger’s disease) I73.81 Erythromelalgia I73.89 Other specified peripheral vascular diseases Copyright c 2015 Confidential and Proprietary Information Venous Insufficiency ICD-9-CM ICD-10-CM 459.81 Venous (peripheral) insufficiency, unspecified I87.2 Venous insufficiency (chronic) (peripheral) Copyright c 2015 Confidential and Proprietary Information Follow-up Examination, Following Surgery, Unspecified ICD-9-CM ICD-10-CM V67.00 Follow-up examination, following surgery, unspecified Z09 Encounter for follow-up examination after completed treatment for conditions other than malignant neoplasm ** Use additional code to identify any applicable history of disease code (Z86.-, Z87.-) Copyright c 2015 Confidential and Proprietary Information Clinical Documentation Awareness Tips Acute Myocardial Infarction Documentation Awareness Timeframe An AMI is now considered “acute” (or recent) for 4 weeks from the time of the incident, which is revised from ICD-9 period of 8 weeks NOTE: document the date of the recent MI Episode of care No longer captured in ICD-10 Subsequent AMI ICD-10 allows coding of a new MI that occurs during the 4 week acute period of the original AMI Type e.g. STEMI, NSTEMI Site STEMI requires site e.g. anterior wall, inferior wall and specific artery e.g. left main coronary artery, LAD diagonal, RCA, left circumflex oblique marginal NSTEMI – no additional information needed Acute Myocardial Infarction ICD-9-CM ICD-10-CM ICD-10-CM 410.0X AMI of anterolateral wall I21.09 STEMI involving other coronary artery of anterolateral wall I22.0 Subsequent STEMI of anterolateral wall 410.1X AMI of other anterior wall I21.09 STEMI involving other coronary artery of anterior wall I22.0 Subsequent STEMI of anterior wall 410.2X AMI of I21.19 STEMI involving other inferolateral wall coronary artery of inferolateral wall I22.1 Subsequent STEMI of inferolateral wall 410.3X AMI of inferoposterior wall I21.19 STEMI involving other coronary artery of inferoposterior wall I22.1 Subsequent STEMI of inferoposterior wall 410.4X AMI of other inferior wall I21.19 STEMI involving other coronary artery of inferior wall I22.1 Subsequent STEMI of inferior wall 410.5X AMI of 121.29 STEMI involving other other lateral wall sites I22.8 Subsequent STEMI of other sites Acute Myocardial Infarction (cont’d) ICD-10-CM I21.01 STEMI involving left main coronary artery I21.02 STEMI involving left anterior descending coronary artery I21.11 STEMI involving right coronary artery I21.21 STEMI involving left circumflex coronary artery Chest Pain and Shortness of Breath ICD-9-CM ICD-10-CM 786.50 Chest pain, unspecified R07.9 Chest pain, unspecified 786.51 Precordial pain R07.2 Precordial pain 786.52 Painful respiration R07.1 Chest pain on breathing 786.59 Chest pain, other R07.89 Chest pain, other R07.81 Pleurodynia R07.82 Intercostal pain 786.05 Shortness of Breath R06.02 Shortness of Breath Documentation Awareness Tips Open Wounds Documentation Awareness Wounds/lacerations require a higher specificity in ICD-10 Type e.g. puncture, open bite Location e.g. thumb, index, ring, little, middle Laterality e.g. left, right Involvement e.g. With nail damage, with foreign body Don’t forget the 7th character! Note: Each finger has a code set specific to the finger. Open Wound Finger ICD-9-CM ICD-10-CM 883.0 Open wound finger(s) w/o mention of complication S61.011- Laceration w/o FB of right thumb w/o damage to the nail 883.1 Open wound finger(s) w/ complication S61012- Laceration w/o FB of left thumb w/o damage to the nail 883.2 Open wound finger(s) w tendon involvement S61.021- Laceration w/ FB of right thumb w/o damage to the nail S61.022- Laceration w/ FB of left thumb w/o damage to the nail S61.031- Puncture wound w/o FB of right thumb w/o damage to nail S61.032- Puncture wound w/o FB of left thumb w/o damage to nail S61.041 -Puncture wound w/ FB of right thumb w/o damage to nail S61.042- Puncture wound w/ FB of left thumb w/o damage to nail S61.051- Open bite of right thumb w/o damage to nail S61.052- Open bite of right thumb w/o damage to nail Open Wound Finger (cont’d) ICD-9-CM ICD-10-CM 883.0 Open wound finger(s) w/o mention S61.111- Laceration w/o FB of right thumb w/ of complication damage to the nail 883.1 Open wound finger(s) w/ complication S61.112- Laceration w/o FB of left thumb w/damage to the nail 883.2 Open wound finger(s) w tendon involvement S61.121- Laceration w/ FB of right thumb w/ damage to the nail S61.122- Laceration w/ FB of left thumb w/ damage to the nail S61.131- Puncture wound w/o FB of right thumb w/ damage to nail S61.132- Puncture wound w/o FB of left thumb w/ damage to nail S61.141 -Puncture wound w/ FB of right thumb w/ damage to nail Open Wound Finger (cont’d) S61.142- Puncture wound w/ FB of left thumb w/ damage to nail S61.151- Open bite of right thumb w/ damage to nail S61.152- Open bite of right thumb w/ damage to nail Copyright c 2015 Confidential and Proprietary Information Documentation Awareness Tips Injury Knee Documentation Awareness Site: e.g. anterior horn, posterior horn Laterality 1: e.g. right, left, bilateral Laterality 2: e.g. medial, lateral, anterior, posterior Type: e.g. complex, bucket handle, peripheral Status: e.g. current, old Knee ICD-9-CM ICD-10-CM 836.0 Medial Meniscus Tear, S83.211 Buckle-handle tear of medial meniscus current knee injury, right knee 836.1 Lateral Meniscus Tear, knee S83.212 Buckle-handle tear of medial meniscus current injury, left knee S83.221 Peripheral tear of medial meniscus current injury, right knee S83.222 Peripheral tear of medial meniscus current injury, left knee S83.231 Complex tear of medial meniscus current injury, right knee Knee ICD-9-CM ICD-10-CM S83.232 Complex tear of medial meniscus current injury, left knee S83.251 Buckle-handle tear of lateral meniscus current injury, right knee S83.252 Buckle-handle tear of lateral meniscus current injury, left knee S83.261 Peripheral tear of lateral meniscus current injury, right knee S83.262 Peripheral tear of lateral meniscus current injury, left knee S83.271 Complex tear of lateral meniscus current injury, right knee S83.272 Complex tear of lateral meniscus current injury, left knee Knee ICD-9-CM ICD-10-CM 717.0 Old bucket handle tear medial meniscus, knee M23.211 Derangement of anterior horn of medial meniscus due to old tear or injury, right knee 717.1 Old anterior horn tear medial meniscus, knee M23.212 Derangement of anterior horn of medial meniscus due to old tear or injury, left knee 717.2 Old posterior horn tear medial M23.221 Derangement of posterior horn of meniscus, knee medial meniscus due to old tear or injury, right knee 717.41 Old bucket handle tear lateral M23.222 Derangement of posterior horn of meniscus, knee medial meniscus due to old tear or injury, left knee 717.42 Old anterior horn tear lateral meniscus, knee 717.43 Old posterior horn tear lateral meniscus, knee Knee ICD-10-CM M23.241 Derangement of anterior horn of lateral meniscus due to old tear or injury, right knee M23.242 Derangement of anterior horn of lateral meniscus due to old tear or injury, left knee M23.251 Derangement of posterior horn of lateral meniscus due to old tear or injury, right knee M23.252 Derangement of posterior horn of lateral meniscus due to old tear or injury, left knee Copyright c 2015 Confidential and Proprietary Information Knee ICD-9-CM 844.2 ACL tear, knee ICD-10-CM S83.511- Sprain of anterior cruciate ligament of right knee S83.512- Sprain of anterior cruciate ligament of left knee S83.521- Sprain of posterior cruciate ligament of right knee S83.522- Sprain of posterior cruciate ligament of left knee Knee ICD-9-CM ICD-10-CM 717.83 Old disruption of ACL M23.611 Other spontaneous disruption of anterior cruciate ligament of right knee 717.84 Old disruption of PCL M23.612 Other spontaneous disruption of anterior cruciate ligament of left knee M23.621 Other spontaneous disruption of posterior cruciate ligament of right knee M23.622 Other spontaneous disruption of posterior cruciate ligament of left knee Copyright c 2015 Confidential and Proprietary Information Training & Education Resources • Medkoder, LLC - http://www.medkoder.com - aaudler@medkoder.com • AAPC - http://www.aapc.com • AHIMA - http://www.ahima.org • CMS – http://www.cms.gov/Medicare/Coding/ICD10/Index.html – http://www.roadto10.org Copyright © 2015 Confidential and Proprietary Information 149 Questions Copyright © 2015 Confidential and Proprietary Information 150 Thank You! MEDKODER 200 Greenleaves Blvd. Suite 7 Mandeville, LA 70448 985-778-0962 phone | 800-421-9418 fax aaudler@medkoder.com support@medkoder.com http://medkoder.com Copyright © 2015 MEDKODER LLC Confidential and Proprietary Information 151